
Abstract
Hip fracture is becoming a major public health concern, with associated mortality and morbidity particularly in the elderly. This study aims to investigate factors (i.e. patient factors and hospital variables) associated with increased risk for delaying surgery after hip fractures, and to assess whether and to what extent timing was associated with mortality risk.
All patients aged 65 and over, resident in Emilia Romagna Region (Italy) and admitted to hospital for hip fracture (2009 - 2010) were selected. Data on surgical delay were adjusted using multilevel logistic regression model. A Cox proportional hazard model was fitted to a propensity score matched sample to assess mortality between delayed and early treated patients.
Of the 10, 995 patients included (mean age: 83.3 years), 44.9% underwent surgery within 2 days. Significant risk factors for delayed surgery were: gender (OR: 1.16), comorbidity (OR: 1.29), anticoagulant (OR: 7.64), antiplatelet medication (OR: 2.43), type of procedure (OR: 1.37) and day of admission (OR: Thu-Fri: 6.05; Sat-Sun: 1.17). Type of hospital and annual volume of hip fracture surgeries were not sufficient to explain hospital variability. A significant difference in mortality rate between early and delayed surgery emerged six months post surgery.
Introduction
Hip fracture is a major public health concern. It is associated with significant mortality and morbidity in the elderly. Hip fracture rates are raising rapidly due to longer life expectancy (1–3), with an estimated annual incidence of 87,000 hip fractures in people aged 45 years or older in Italy (4).
Surgery is recognised as the current treatment in the management of these patients, and early surgery is recommended by clinical guidelines (5–7). The issue of the timing of surgery in hip fracture is still debated and the effect of surgical treatment within 48 hours remains unclear (2, 8, 9). Although delay in surgery seems to be allowed when physiological stabilisation after injury is required, recently published studies show that factors other than patient conditions may influence timing (i.e. hospital characteristics such as volume, status, surgeon volume) (10–12). Therefore, when conducting multicentre studies, the methods for assessing surgical delay or mortality must be refined to take into account both the confounding effects of patient characteristics and the hierarchical nature of data. Multilevel methodology is the widely recognised method for explaining hospital level variability (13–15) and, in this case, it may be used to explain which factors were correlated with surgical delay.
The primary aim of this study was to investigate, by the multilevel model, the factors associated with increased risk for delaying surgery in patients with hip fractures discharged from all orthopaedic centres in Emilia Romagna Region (population 4,432,439), Italy. The secondary objective was to assess, through a propensity score matching adjustment, whether timing was associated with the risk of mortality (within one month after admission and from 1 to 6 months).
Materials and Methods
Context
The Emilia Romagna Region is located in the north of Italy and has a population of about 4,432,439. The proportion of population aged 65 years and over equals 22.4% (year 2010), with women comprising the majority of the elderly. The Regional Healthcare Service consists of 11 Local Health Authorities, 5 independent public hospitals, 1 scientific research hospital (Rizzoli Orthopaedic Institute), with a total of 57 public hospitals performing orthopaedic surgery. Hip fracture is a very frequent surgical procedure, with an incidence rate of 7.6 per 1,000 for people aged 65 and over (4.4 and 10 per 1,000 for males and females, respectively).
Design of the study
A retrospective cohort study was conducted using Emilia Romagna administrative database: patients with hip fractures and their coexisting medical conditions were identified by Hospital Discharge Records, while additional information were derived by record linkage with Pharmaceutical database and Mortality Registry. All patients aged 65 and over, resident in Emilia Romagna Region and admitted to a regional acute care hospital for a hip fracture (ICD-9-CM diagnosis codes: 820.0 - 820.9, in any position) between 1 January 2009 and 31 December 2010, were selected. The study excluded from the analysis patients hospitalised for hip fracture in the previous two years, with a malignant neoplasm in the index admission or in the previous two years, with multiple trauma, transferred from other acute care hospitals or patients who died without surgery within one day of admission.
First outcome was delayed surgery; surgery (distinguished in “total or partial hip replacement’, ICD-9-CM intervention codes 81.51-81.52, and in “reduction of fracture’, ICD-9-CM intervention codes 79.00, 79.05, 79.10, 79.15, 79.20, 79.25, 79.30, 79.35, 79.40, 79.45, 79.50, 79.55) was defined “delayed’ if it was not performed within two days of admission. Other outcomes were mortality within 30 days and mortality within 6 months after admission for hip fractures.
Since patients could be grouped into hospitals, data had a hierarchical structure.
First level (patient level) covariates were: age, sex, comorbidity, antiplatelet/anticoagulants assumption, type of surgery (hip replacement/reduction of fracture) and day of admission. Charlson Score Index (16, 17) was computed to assess comorbidity: diagnoses were identified on the basis of ICD-9-CM codes in the index admission and in the previous two years. Any antiplatelet/anticoagulation consumption either in the index admission or in the previous three months was considered. Day of admission was classified in three groups: Monday - Wednesday, Tuesday - Friday and Saturday - Sunday.
Second level (hospital level) covariates were annual volume of surgical procedures and status of hospital (teaching/no-teaching). Hospitals were classified in four classes (12) according to their annual volume of hip fracture surgeries: up to 45 (low volume), from 46 to 200 (medium volume), from 201 to 400 (high volume), more than 400 (very high volume).
Statistical analysis
Continuous variables were expressed as mean ± standard deviation and were compared by the unpaired t-test; categorical variables were expressed as counts and percentages and the comparison was performed by the chi-square test.
Due to the hierarchical nature of data, a multilevel logistic regression was carried out to assess the effect of covariates on delayed surgery, taking into account hospital level variability. The lack of fit between the model and the data was assessed by the deviance statistic (13–15, 18).
Propensity score, which is defined as the conditional probability of early treatment given the covariates (19, 20), was obtained through predicted probabilities estimated by the multilevel model. A propensity score matching analysis was then performed, thus permitting the selection of two well-matched groups (early vs delayed surgery) of 3,134 patients each. In the matched groups, continuous variables were compared by paired t-test, and categorical variables by McNemar's test. Standardised differences were computed for each of the baseline covariates to assess their balance before and after matching (21).
The cumulative incidence of death was estimated by Kaplan – Meier method and compared by Klein and Moeschberger test (22). To better evaluate mortality rates in the short and medium term, landmark analysis was performed with landmark setting at one month. Finally, after having assessed proportional hazards assumption with Schoenfeld test (23, 24) (no violation, p-value = 0.2985), a Cox proportional hazard model with robust standard error to account for clustering (21) was fitted to the matched sample.
The level of significance was set at 5% (p<0.05) and all statistical analysis were performed using SAS 9.1 system (SAS Institute, Cary, North Carolina).
Results
After exclusions, 11,872 patients were hospitalised for hip fracture in Emilia Romagna between 2009 and 2010. Surgically treated patients were mostly women (n = 8,532, 77.6%) and nearly half of them had a Charlson Comorbidity Index of 1 or more (n = 5,212, 47.4%). Compared with non-surgery patients, those treated surgically presented less comorbid diseases (Charlson Comorbidity Index of 1 or more: 47.4% vs 56.9%, p<.0001), assumed fewer drugs (anticoagulants assumption: 6.9% vs 9.2%, p = 0.0109) and were mainly admitted to teaching hospitals (27.6% vs 19.9%, p<.0001) or to hospitals with high (48.1% vs 43.2%, p = 0.0056) or very high (8.6% vs 3.9%, p<.0001) volume. Both mortality within 30 days and mortality within 6 months were significantly lower in patients with surgery (3.7% vs 17.9%, p<.0001 and 15.6% vs 30.3%, p<.0001, respectively).
Among patients treated surgically, 43.3% (n = 4,760) received a total/partial hip replacement, while 56.7% (n = 6,235) underwent surgical stabilisation. Moreover, almost half (n = 4,941, 44.94%) received surgery within 2 days.
To assess risk factors for delayed surgery and to evaluate mortality, patients not treated surgically were excluded from analyses. Multilevel logistic regression, taking into account hospital level variability, shows that only first level (patient level) variables had a significant influence on surgery delay (Fig. 1). Type of hospital and annual volume of hip fracture interventions (second level variables) were not sufficient to explain hospital variability. In fact, from empty model (that is, random intercept model without predictors) to final model (model with first, second level covariate and cross-level interactions), “between hospital variance” did not decrease. Therefore, risk factors for delayed surgery were the following: gender male, comorbidity, drug assumption, type of surgery and day of admission. Patients admitted to hospitals with very high volumes of surgery tended to have a slight lower risk of delayed surgery: the estimated coefficient of cross-level interaction term between day of admission and volume was negative (−0.6837) and just below the significance threshold (p-value = 0.0445).
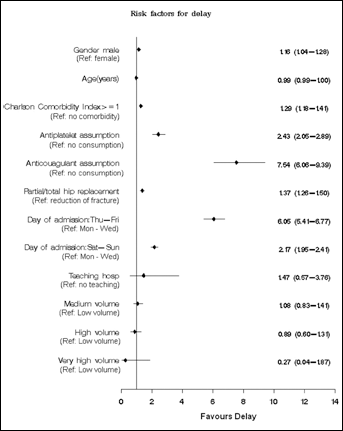
Multilevel model: Forest plots of the odds ratio for the risk of delayed surgery.
Time to surgery distinguished two groups: “early group” (timing within 2 days) and “delayed group” (timing over 2 days). Table I shows differences between groups before and after propensity score matching; as already seen in Figure 1, before matching the two groups were unbalanced. After propensity score matching in the two groups - counted 3.134 patients each – unbalance became negligible. In fact, standardised differences ranged from 0 to 0.035, proving a very good balance between early and delayed group.
Characteristics of Patients with Hip Fracture in the Study Population and After Matching
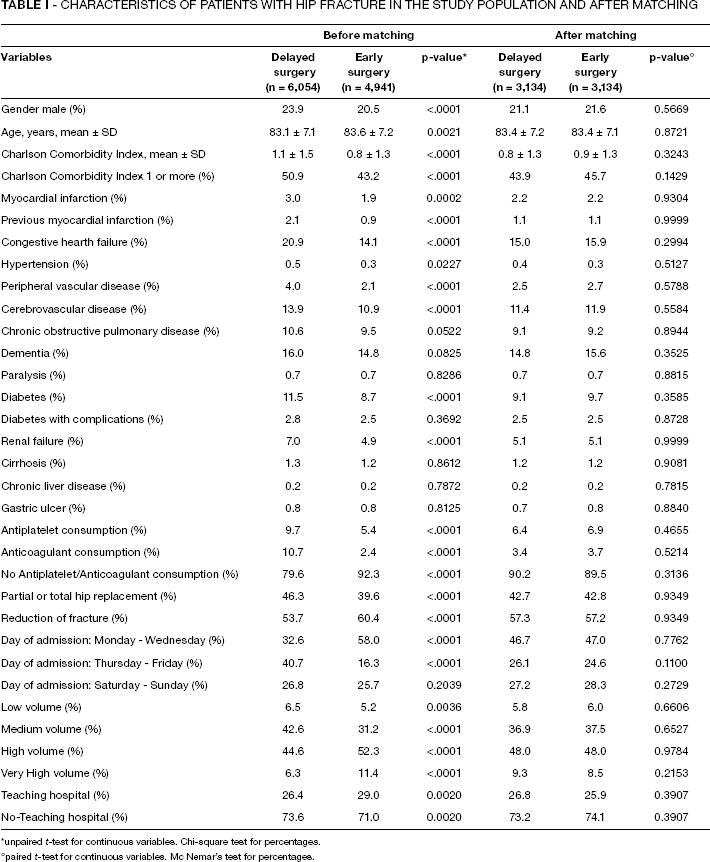
unpaired t-test for continuous variables. Chi-square test for percentages.
paired t-test for continuous variables. Mc Nemar's test for percentages.
After six months, a significant difference in death rates between groups was observed (Klein & Moeschberger test, p-value = 0.0176): as shown in Figure 2, the death rate was significantly higher in the delayed group (16.2% vs 14.4%). However, no difference was observed between early and delayed surgery in the first month (Klein & Moeschberger test, p-value = 0.9466). Indeed landmark analysis in Figure 3 shows that the higher risk of death related to delayed surgery is clear only after the first month (HR 0.84, CI 0.73-0.97).
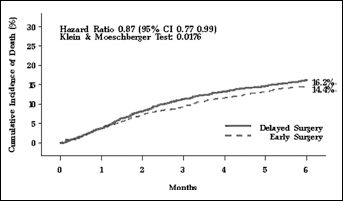
Propensity score adjusted cumulative incidence of death in matched groups.
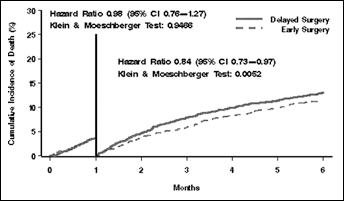
Propensity score adjusted cumulative incidence of death in matched groups (landmark analysis).
Discussion
Analysis of patients with hip fracture shows a broad difference between those managed surgically and those with no-procedure who suffer from severe comorbid conditions. Findings from our region confirm previous evidence gathered in the English-NHS setting (25), where death rates of non-treated patients were slightly higher than those treated surgically.
Although early intervention was strongly suggested by several guidelines on hip fracture management, in our context the number of patients who underwent surgery within two days seems to be limited (45% total) if compared to data from other European countries (25–27). No difference in mortality rate was observed between early and delayed surgery in the first month (HR: 0.98; CI: 0.76-1.27), whereas a significant difference in death rates emerged after six months (HR: 0.84; CI: 0.73-0.97). If those data were confirmed in the long run, mortality would likely to be even more affected by delay.
Even though a consensus on the impact of delay has not been achieved among the scientific community (2, 8, 12, 25), the benefits of early surgery were extensively acknowledged. Findings showed that in our region early surgery matters in terms of patient outcomes. Therefore, it becomes fundamental to understand which factors best explain the delay in surgery.
Multilevel analysis demonstrates that delay is mainly favoured by patient characteristics (gender, comorbidities, drug therapy and type of procedure). Contrary to the recommendations of SIGN guidelines (6, 28), either antiplatelet or anticoagulant consumption strongly discourages early surgery in favour of patient stabilisation. Between them, anticoagulant represents the main risk factor for delay. Waiting for surgery could be mainly due to the risks associated with intra-operative bleeding and spinal haematoma, as demonstrated by several authors (29, 30). In addition, the American Society of Regional Anaesthesia recommends stopping the anticoagulant for at least 7 days prior to administering neuroaxial anaesthesia (30) and anecdotally 10 days in many UK institutions. Performing early surgery in patients treated with anticoagulant is still debatable (31) and our results added further information on the clinical practice in our healthcare system. Comorbidities also require the stabilisation of medical problems in order to avoid perioperative complications. As expected, also type of procedure (i.e. partial or total hip replacement vs reduction of fracture) drives the time of surgery according to its complexity.
Results from multilevel model also show that delay is not significantly influenced by hospital features. Neither hospital status nor hospital volume determines the management of hip fracture in terms of early or delayed surgery; all conditions being equal, delay does not depend on the hospital characteristics. However, conclusive statements on the role of factors other than clinical variables could not be drawn up without mentioning the effect of “the day of admission”. Although the day is identified as a patient-level variable, it should be examined as a hospital organisational variable since it signals the effect of limitations of surgery availability from Thursday to Sunday. Previous studies on management of urgent surgery in different clinical domains (20, 32–34) and also in orthopaedics (35, 36) demonstrated that timing of intervention frequently depends on the availability of procedure and patients admitted on different days were associated with dissimilar probability of receiving early-surgery. Other authors (37) instead attributed the delay in surgery for patients with femoral fractures to organisational reasons in general. Our study confirms those results and extends the amount of evidence available on the orthopaedic field by using a robust methodology. The “day of admission effect” seems reduced (even if significance does not emerge) when considering centres with higher volumes. Moreover cross-level interactions show that the effect is partially reduced (p = 0.0445) in very high-volume centres. Therefore, it can be argued that very high volume centres may have implemented strategies to promptly manage urgent hip surgery. From a methodological perspective, the study has two main strengths. First, the multilevel model fits the hierarchical structure of data (e.g. patient and hospital level) and offers the opportunity to obtain robust results. Second, propensity score method was used to match cases of early and late surgery compensating the limits of the non-randomisation design of the study. As the proportion of patients (older than 65 years) with early surgery is limited in other Italian regions and abroad (12, 38, 42, 43), our findings could be very helpful in supporting the choices of clinicians and hospital managers concerning the management of patients with hip fracture.
The study presents several limitations associated with the use of administrative databases that do not provide complete clinical and organisational information. Data about ASA score and INR were not available as well as the actual hour of surgery. As a consequence, the severity of patient was estimated by Charlson Comorbidity Index and drug therapy, whereas time to surgery was approximated by the difference between the day of surgery and admission. In this way it was specified the cut-off of two days (in place of 48 hours) to define early/delayed surgery. Beyond administrative database weaknesses, it can also be argued that organisational aspects are context-specific.
However, our results provide an opportunity to examine the determinants of delay and its consequences in a comprehensive regional healthcare system through rigorous statistical methodology. Therefore, our findings could be used by both clinicians and hospital decision-makers to implement appropriate strategies to limit those delays that depend on organisational factors. With appropriate initiatives, they may shorten patient pain and improve his recovery and future life expectancy.
Footnotes
Financial support: None.
Conflict of interest: The authors declare that they have no competing interests.