
Abstract
Background
Urinary retention (UR) is not common in women. There are numerous causes now recognized in women, broadly categorized as infective, pharmacological, neurological, anatomical, myopathic and functional. As opposed to the male, obstructive UR is unusual in women.
Methods
A 56-year-old woman presented with urinary retention. She reported difficulty in urination for more than 15 days. She had no history of urinary tract infection, bladder surgery and catheterization. Her physical examination revealed a soft tissue mass obstructing the external orifice of the urethra. After its partial removal the patient regained her ability to urinate.
Results
The patient underwent urological investigation. Ultrasound examination of the urinary system was normal. Cystoscopic examination revealed a papillary lesion with broad base floating along the bladder neck. The patient underwent transurethral resection of the bladder tumor.
Discussion
Pathological examination diagnosed papillary cystitis. She was scheduled for a regular follow-up with urine cytology, ultrasound and cystoscopy. One year after diagnosis the patient remains free of symptoms and no recurrence was observed.
Conclusions
Papillary and polypoid cystitis are benign lesions, however under certain circumstances they should be considered in the differential diagnosis of transitional cell carcinoma of the bladder. Lack of the prominent inflammation and edema that characterizes both papillary and polypoid cystitis, and absence of a history of recent bladder catheterization and presence of vesical fistula may facilitate the decision to biopsy the lesion. To our knowledge, this is the first case of papillary cystitis presenting with urinary retention in a woman to be reported in the literature.
Keywords
Introduction
Urinary retention (UR) is not common in women. Moreover, the epidemiology of female UR is not well documented (1). There are numerous causes now recognized in women, broadly categorized as infective, pharmacological, neurological, anatomical, myopathic and functional. As opposed to the male, obstructive UR is unusual in women. Initial management includes bladder drainage (intermittent or indwelling catheterization) if the woman is symptomatic or at risk of complications, and correcting likely causes. Investigations should be focused on identifying the underlying etiology and any reversible factor (1). In this report pelvic examination and cystoscopy diagnosed the first case reported in the literature of papillary cystitis presenting with urinary retention in a woman.
Methods
A 56-year-old woman presented with urinary retention. She also complained of difficulty in urination for more than 15 days. No fever, dysuria, frequent and painful urination were reported. She had no history of urinary tract infection, bladder surgery and catheterization. Her physical examination revealed a large well-demarcated hemorrhagic soft tissue mass obstructing the external orifice of the urethra. After its removal, the patient regained her ability to urinate. Abdominal ultrasound showed a normal shape and configuration of both kidneys. The urinary bladder was shown to have a normal wall and no residual urine was noted. Cystoscopic examination revealed a finger-like papillary lesion floating along the bladder neck (Fig. 1). The lesion had a broad base originating from the bladder neck. The patient underwent transurethral resection of the bladder tumor.
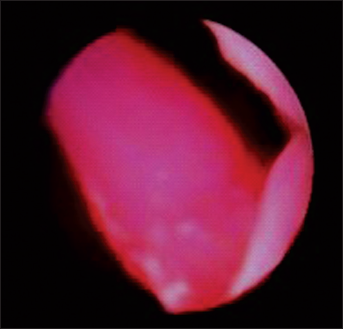
Cystoscopy image: A finger-like papillary lesion floats along the bladder neck.
Results
Pathological examination of both urethral and bladder neck tissue diagnosed papillary cystitis (Fig. 2). One year after diagnosis the patient remains free of symptoms and no recurrence was observed. To our knowledge, this is the first case reported in the literature of papillary cystitis presenting with urinary retention in a woman.
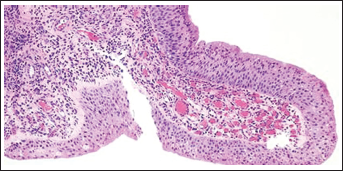
Pathology image.
Discussion
Papillary or polypoid cystitis is a reactive urothelial proliferation, which may follow bladder surgery and instrumentation, colo-vesical fistula, recurrent or untreated infection, long-standing urinary stents and indwelling catheterization (2). It occurs equally in females and males with an age range of 20 months to 79 years. It may appear as a single, thin, finger-like papilla or broad based edematous polypoid lesion. The first pattern commonly occurs along the bladder neck and it is associated to inflammation and bladder neck surgery, while the second is usually seen on the posterior wall and represents either catheter tip reaction or granulomatous inflammation secondary to colo-vesical fistula. Lesions displaying the first pattern are called polypoid cystitis while those displaying the second pattern are defined as papillary cystitis (3). Microscopically these lesions are characterized by congestion and edema of lamina propria and mild chronic inflammatory infiltrate (3). The lining epithelium shows orderly maturation with presence of surface umbrella cells, or it may show metaplasia (4). The pathophysiology of these entities is not fully understood, however, as both are associated with inflammation, they may relate to metaplastic changes in the urothelium covering them, or adjacent to them (4).
The most frequent cited symptoms associated to these entities include bladder obstruction (23%), gross hematuria (20%) and colo-vesicular fistula (13%). Only a small number report frequent and painful urination and voiding dysfunction (3.3%) (5). According to Lane and Epstein however, most patients (39.4%) with papillary or polypoid cystitis are asymptomatic in the follow-up status post-treatment of bladder and ureter carcinoma, during the follow-up after radiation for prostate cancer, on investigation of bladder/urethral stones and benign prostate hyperplasia (3).
On abdominal ultrasound, papillary and polypoid cystitis may appear as urinary bladder wall thickening accompanied by a variable number of small masses that protrude from the mucosa into its lumen. Cystoscopic appearance is an area of friable mucosal irregularity or edematous broad papillae. Lesions may be multifocal and can range up to 5 mm in size. It should be mentioned that there is an obvious overlap between the two ends of the spectrum (papillary and polypoid cystitis). In fact, while in both papillary and polypoid cystitis there is chronic inflammation in the stroma and blood vessels, inflammatory phenomena of papillary cystitis are more prominent. In addition the stroma of polypoid cystitis is typically edematous while that of papillary cystitis varies from edematous to more fibrous (4). For this reason, papillary cystitis is considering a more chronic phase of polypoid cystitis. Of note, the last is less likely to be associated with adjacent malignant lesions. In contrast, tumors of the sigmoid colon or cervix invading the bladder often co-exist with papillary cystitis, and practically, this pattern is more likely to be confused with papillary carcinoma (3). In fact, the thin papillae of papillary cystitis are difficult to distinguish from carcinoma on gross inspection. In microscopic examination however, the benign urothelium may be hyperplastic, but usually it is not as stratified as in a carcinoma, while umbrella cells are more often present. Additionally, large papillae of papillary cystitis rarely give rise to smaller papillae, a feature commonly seen in papillary carcinoma (5).
Conclusions
Papillary and polypoid cystitis are benign lesions, however under certain circumstances they should be considered in the differential diagnosis of transitional cell carcinoma of the bladder. Lack of the prominent inflammation and edema that characterizes both papillary and polypoid cystitis, and absence of a history of recent bladder catheterization and presence of vesical fistula may facilitate the decision to biopsy the lesion.
Riassunto
Una donna di 56 anni si è presentata all'ospedale con ritenzione urinaria. Ha riferito problemi di minzione per più di 15 giorni. Non aveva una storia di infezione del tratto urinario, né chirurgia o cateterizzazione della vescica. Il suo esame fisico ha rivelato un tumore di tessuto molle che promoveva dall'orifizio esterno dell'uretra. Dopo la sua rimozione la paziente ha riacquistato la capacità di urinare. L'ecografia del sistema urinario era normale. L'esame cistoscopico ha rivelato una lesione papillare, con base ampia galleggiante lungo il collo vescicale. La paziente è sottoposta a resezione transuretrale del tumore della vescica. L'esame patologico ha dimostrato cistite papillare. Dopo un anno di follow-up, la paziente è senza involuzione. A nostra conoscenza, questo è il primo caso di cistite papillare presentata con ritenzione urinaria femminile da riportare in letteratura.
Footnotes
There is no financial or other conflict of interest that might have biased the work.