
Abstract
Purpose
To report a case of retinal detachment in an eye with choroidal coloboma treated with pneumatic retinopexy and laser.
Methods
Case report.
Results
A 34-year-old woman who had had poor vision in her left eye since early childhood and high myopia in her right eye complained a sudden deterioration of vision in her left eye for 3 days. Fundus examination of the left eye showed a large choroidal coloboma, extending to the disc margin from 5–8 o'clock inferiorly and above the inferotemporal arcade, excluding the fovea and the parafovea. Superotemporal bullous detachment of the retina was also observed, including the macula. The patient underwent a pneumatic retinopexy with SF6 gas (0.5 cc) injection into the vitreous cavity. The following day laser was applied around the margin of the choroidal coloboma. Three months later, visual acuity was 20/200 and fundus examination disclosed a completely attached retina.
Conclusions
This case demonstrates the feasibility of using pneumatic retinopexy in selected cases.
Introduction
Coloboma of the fundus is a congenital defect caused by improper closure of the embryonal fissure during the fourth to fifth week of embryonic development that typically involves the inferonasal sector of the eye.
The prevalence of retinal detachment (RD) in eyes with choroidal coloboma (CC) has been reported to be 8%-40% (1). Retinal detachment and coloboma could be causally related or could be a coincidental occurrence. Where the coloboma is responsible etiologically for the RD, literature suggests, as first line treatment, pars plana vitrectomy with endolaser and silicone oil tamponade.
We report a case of RD related to CC, which regressed after pneumatic retinopexy and laser treatment. To our knowledge, this is the first documented case treated with pneumatic retinopexy and laser.
Case report
A 34-year-old woman who had had poor vision (20/200) in her left eye since early childhood and high myopia in her right eye (refractive error −7 D) was referred to the clinic complaining of sudden deterioration of vision in her left eye for 3 days. Her family history was unremarkable. Her medical history included cardiac anomalies such as arrhythmia, right ventricular hypertrophy, and right axial deviation.
A full ocular examination was performed. The best-corrected visual acuity (BCVA) of the right eye was 20/20 with correction of −7 D, while that of the left eye was finger counting with correction of −10 D. Intraocular pressure was 15 mmHg in the right eye and 12 mmHg in the left eye. Slit-lamp examination showed clear corneas and lenses in both eyes. The left eye had a coloboma of the iris, which manifested itself as a small notch in the inferonasal pupillary margin. Fundus examination of the right eye showed a myopic tigroid fundus with tilted disc and peripapillary atrophy. Fundus examination of the left eye showed a large choroidal coloboma, extending to the disc margin from 5-8 o'clock inferiorly and above the inferotemporal arcade, excluding the fovea and the parafovea. Superotemporal bullous detachment of the retina was observed including the macula (Figs. 1 and 2). No visible retinal break/hole was detected either in the retina or the intercalary membrane covering the coloboma. The patient underwent an injection (0.5 cc SF6) into the vitreous cavity followed by an anterior chamber paracentesis.
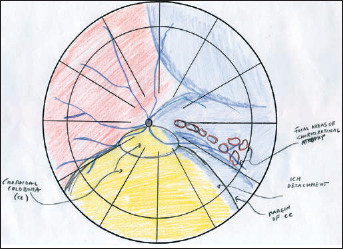
Fundus drawing showing retinal detachment and the detachment of the intercalary membrane (ICM) in the temporal margin of the coloboma. CC = choroidal coloboma.
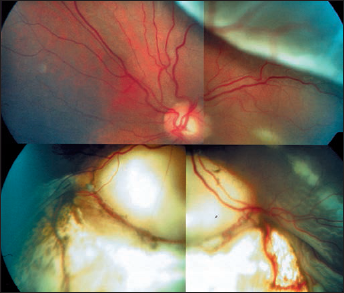
Preoperative photograph of large inferior coloboma.
The patient was instructed to maintain head-down positioning for 12 hours. Follow-up assessment on the following day disclosed complete reabsorption of the subretinal fluid. Laser treatment was applied around the entire CC. The patient was then instructed to maintain lateral positioning on her right side as much as possible.
One week later, the retina remained attached and no new breaks were noted.
Three months later, visual acuity was 20/250 and fundus examination disclosed a completely attached retina (Fig. 3).
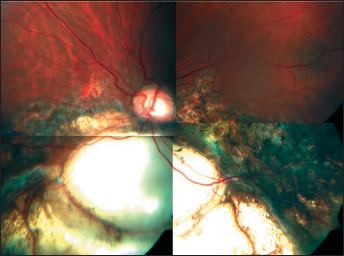
Photograph of fundus 3 months later showing completely attached retina with laser retinopexy around choroidal coloboma.
Discussion
Retinal detachments caused by coloboma of the fundus are relatively rare. Retinal detachment can occur in eyes with CC because of a retinal break outside the colobomatous area, at the margin of the coloboma, or over the coloboma. Clinical studies of CCs with RD have shown that the RDs etiologically related to the CCs have characteristic features (2). These features include a detachment of the intercalary membrane (ICM) along with breaks in the ICM and generally an absence of peripheral retinal breaks. The communication between ICM and RD is made possible if there is a dehiscence in the adhesion of the retinal pigment epithelium (RPE) to the neurosensory retina at the margin of the coloboma (locus minoris resistentiae [LMR]). However, the location of such a communication is often impossible to pinpoint clinically.
In our case the RD extended from the temporal margin of the CC to the superior quadrant of the retina. Since visible breaks/holes of the ICM had not been detected clinically, we assumed a causative relationship between the RD and the CC based on the absence of peripheral breaks of the retina and the presence of detachment of the ICM on the temporal side of the CC. All these features were suggestive of a hole in the ICM and LMR near the temporal margin of the CC.
Treatment of these patients with scleral buckling techniques is difficult as evidenced by the poor results reported and may be related to the difficulty in identifying and closing the causative retinal breaks (3). Pars plana vitrectomy with silicone oil tamponade has markedly improved the success rates (2, 4).
Compared with scleral buckling or vitrectomy, pneumatic retinopexy (PR) provides a less invasive and often better tolerated therapeutic alternative in selected cases. Several studies have demonstrated its comparative efficacy compared with scleral buckling in the treatment of primary rhegmatogenous RDs. Randomized trial criteria and practices of experienced vitreoretinal specialists have established the current standard of care for pneumatic retinopexy, which advocates the treatment of rhegmatogenous RDs when visible retinal breaks lie in the superior two-thirds of the retina.
Inferior retinal breaks and RDs without retinal breaks have generally been considered a contraindication for pneumatic retinopexy. However, in 2003 Chang et al (5) successfully used a modified pneumatic technique for treatment of inferior RDs.
In our case we decided to perform PR because of the ability of the young patient to maintain an inverted position and because the volume of the bubble injected could tamponade the temporal margin of the coloboma, the starting point of the RD.
However, pneumatic retinopexy may induce considerable increases in intraocular pressure potentially leading to ruptures of the thin sclera which typically forms the floor of the coloboma. Even without any increase in intraocular pressure some authors have described spontaneous rupture of the sclera in choroidal coloboma (6, 7). Rupture of the sclera may be a rare complication in equally rare choroidal colobomas; however, the patients should be informed about this real possibility. Unlike normal eyes undergoing retinal pneumopexy, thin sclera is typically part of the colobomatous malformation related to lack of choroidal and scleral induction by the missing RPE.
Our case demonstrates the feasibility of pneumatic retinopexy in selected cases of RD.