
Abstract
Purpose
To describe the use of 3 prostaglandin/timolol fixed combinations (FCs) in UK primary care, to summarize characteristics of recipients, and to assess 12-month persistence.
Methods
This retrospective cohort study included first-time recipients of latanoprost/timolol FC, bimatoprost/timolol FC, or travoprost/timolol FC treated between April 1, 2007, and November 30, 2008, identified in The Health Improvement Network database, a large database of anonymized longitudinal electronic medical records of patients treated in UK primary care. Eligible patients were ≥18 years old at the index date (date of first prescription). Persistence, defined as a gap ≤60 days between consecutive prescriptions, was assessed through 12 months post-index for each cohort (Cox proportional hazards models).
Results
A total of 2,015 patients were included: latanoprost/timolol FC, n=898 (44.6%); bimatoprost/timolol FC, n=733 (36.4%); travoprost/timolol FC, n=384 (19.1%). The mean age was approximately 72 years across cohorts (p=0.792). Glaucoma was the diagnosis for >90% of patients in each cohort. Twelve-month persistence was similar across treatments: latanoprost/timolol FC: 38.2%; bimatoprost/timolol FC: 38.6%; travoprost/timolol FC: 38.3% (p=0.985). Mean time to therapy change for nonpersistent patients was also similar: 143.3±89.8, 151.0±87.9, and 151.8±87.7 days, respectively (p=0.095). Among persistent patients, additional therapy was prescribed for 36.2%, 41.7%, and 41.5% of patients, respectively. Among nonpersistent patients, 64.0%, 70.4%, and 69.2%, respectively, restarted the index therapy.
Conclusions
The largest proportion of first-time recipients of prostaglandin/beta-blocker FC products treated in UK primary care was prescribed latanoprost/timolol FC. Twelve-month persistence was similar (<40%) across the 3 FCs evaluated.
Introduction
Glaucoma, the second most common cause of blindness worldwide, will affect nearly 80 million people by 2020, with 59 million of those having open-angle glaucoma (1). Previous research (2-7) has demonstrated that use of topical ocular hypotensive agents to reduce intraocular pressure (IOP) levels can delay or stop both progression of ocular hypertension to glaucoma and progression of glaucomatous damage in those with the condition. Among patients who do not achieve their target IOP levels with monotherapy, the European Glaucoma Society recommends that a second medication from a different pharmacologic class be added to the original agent (European Glaucoma Society Terminology and Guidelines for Glaucoma [http://www.eugs.org/ebook.asp]). Use of multiple topical ocular hypotensive agents is common and 39.7% of medication participants in the Ocular Hypertension Treatment Study (4) were prescribed 2 or more such medications by month 60. In patients requiring multiple therapies, a fixed-combination (FC) formulation may be preferred in order to maximize patient adherence and quality of life (European Glaucoma Society Terminology and Guidelines for Glaucoma [http://www.eugs.org/ebook.asp]).
Persistence, prescriptions issued over time, is a prerequisite for adherence as patients must obtain a medication before it can be taken as directed. Although long-term persistence in individuals with ocular hypertension and glaucoma generally has been found to be poor, persistence estimates vary depending on the study design and the agents evaluated (8-16). Overall, persistence has been shown to be higher with prostaglandin analogues than with alternative agents (11, 13, 15), and within the prostaglandin class, several studies have found persistence to be higher with latanoprost compared with bimatoprost and travoprost (10, 12, 14, 16, 17).
Few studies (18, 19) have focused on persistence with FC ocular hypotensives and to our knowledge none have compared persistence across FCs of prostaglandin analogues and timolol. Three such formulations are approved in Europe: latanoprost/timolol FC (Xalacom®), bimatoprost/timolol FC (Ganfort®), and travoprost/timolol FC (DuoTrav®). The purposes of the present study were to describe the use of these agents in UK primary care, where chronic conditions such as glaucoma are generally managed, to summarize characteristics of recipients, and to assess and compare 12-month persistence with these FCs.
Methods
Data source
The Health Improvement Network (THIN) is a large, longitudinal database of anonymized electronic medical records of patients treated in UK primary care. Practices that have agreed to contribute data to THIN use Vision practice management software and the data collection scheme was approved by the NHS South East Multicentre Research Ethics Committee (MREC reference number: 03/01/073) and registered on clinicaltrials.gov (NCT01206361). The THIN patient population is representative of the general UK patient population with respect to distributions of gender and age (internal data) and the prevalence of major diseases (20). Furthermore, THIN data have been found to be similar to data from practices using the Egton Medical Information Systems Ltd. (EMIS) general practice software, although patients in THIN are slightly more representative of more affluent social classes (21). The THIN uses Read codes for diagnoses and Multilex codes for drug prescriptions. When data for the present study were extracted, THIN included records from 464 general practices nationwide representing more than 8.7 million patients, of whom more than 3.3 million were actively registered during the study period. The population in THIN in 2007 covered 5.3% of the UK population (internal data).
Study design
The present retrospective cohort study included patients who received an index (first) prescription for latanoprost/timolol FC, bimatoprost/timolol FC, or travoprost/timolol FC between April 1, 2007, and November 30, 2008, were ≥18 years old at the index date (date of first prescription), and had ≥12 months quality-controlled data prior to the index date. Patients were followed up until the earliest of: 1) the date that the patient transferred out of the practice, 2) the date of the practice's last data collection, or 3) 12 months after the index date. The study was approved by the Cambridgeshire 4 Research Ethics Committee (REC reference number: 10/H0305/11).
Information concerning demographic characteristics, glaucoma or ocular hypertension diagnosis, comorbidities, ocular procedures, and prescriptions for ocular hypotensive therapy was collected from records dated prior to the index date (baseline data). The Townsend score (22), an index of the social and economic deprivation of a locality, was used to reflect patients’ socioeconomic status based on postal codes. Data concerning prescriptions for ocular hypotensive medications and ocular procedures were collected for up to 12 months following the index date.
Analyses
Baseline demographic and ocular characteristics and procedures, comorbidities, and time from glaucoma or ocular hypertension diagnosis to the index date were compared across the 3 FC treatment cohorts. The across-cohort differences were evaluated at a 5% significance level using analysis of variance (ANOVA) for continuous variables and chi-square tests for categorical variables.
Latanoprost/timolol FC and travoprost/timolol FC are packaged in 2.5 mL bottles and bimatoprost/timolol FC is packaged in a 3.0 mL bottle; bottles containing each formulation need to be used within 28 days after opening. Persistence with the index FC, defined as a gap ≤60 days between consecutive prescriptions, was assessed through 12 months post-index for each cohort. The 60-day threshold for discriminating between persistence and nonpersistence was chosen by investigating the interval between dates of consecutively issued prescriptions for study drugs. This approach was developed because limited information is available electronically on whether patients have been directed to apply ocular hypotensive therapy to one or both eyes or the number of drops, which makes it difficult to predict the volume of drug to be used. In determining the threshold, it was considered that patients could have received multiple prescriptions and/or prescriptions for multiple bottles (1 or 3 bottles) on the same date as aggregate time between consecutive prescription issue dates was evaluated. The exploratory study in THIN revealed a mean interval of approximately 35 days and a median of approximately 30 days between prescription dates (range of upper quartile: 35 to 49 days). The mean time interval before the next prescription was longer (approximately 40 to 60 days across the prescription issue intervals over time) among patients given 2 or more prescriptions on the same date. Based on these factors, the choice of a 60-day threshold was deemed reasonable. The fact that other studies of persistence also have used this threshold further supports this choice (23-27).
Persistent patients were those who were either prescribed only the index FC or who were prescribed a medication from a different therapeutic class (e.g., carbonic anhydrase inhibitors) in addition to the index FC, i.e. add-on therapy. The purpose of identifying add-on therapies was to evaluate how many persistent patients received a prescription for a non-index FC ocular hypotensive agent at any time during follow-up. The timing of the prescription for the additional therapy was not assessed and therefore the new agent could have been prescribed after the patient's last index FC. Nonpersistence was defined as a gap of >60 days between consecutive prescriptions for the index FC and may have reflected the following conditions: 1) restart: prescription for the index FC after a gap of >60 days and no prescription for an alternative ocular hypotensive therapy during the gap period; 2) switch: prescription for a study FC other than the index FC (e.g., if the index FC was travoprost/timolol FC and a subsequent prescription for bimatoprost/timolol FC was recorded); and 3) discontinuation: gap of >60 days between consecutive prescriptions and neither a restart of the index FC nor a switch to another study FC and a time gap between the last index FC and the end of the observation period of >60 days. In addition, a few patients were prescribed one of the study FC drugs other than the index FC before they restarted the index FC; these individuals were classified as other nonpersistent. In all analyses, only the first event was counted (e.g., if a patient restarted the index FC and later discontinued the agent, only the restart event was counted).
Differences in persistence among cohorts were evaluated using chi-square tests. Cox proportional hazards models were used to evaluate at a 5% significance level whether persistence differed between cohorts once baseline covariates (chosen a priori) were adjusted for, along with differences in the time that patients could potentially have changed therapy and loss to follow-up. Time to discontinuation was defined as the time between the index date and the date of the last index drug prescription plus the estimated duration of that final prescription. Time to switch was calculated as the time between the index date and the date of the first prescription of the new study drug. Time to restart was defined as the time between the index date and the date of the next prescription for the index FC after a gap of >60 days. For those who were “other nonpersistent”, time to change was the time between the index date and the date of the first prescription of the new, non-index study drug. Kaplan-Meier survival plots graphically represented proportions of persistent patients throughout the follow-up period for each cohort.
Results
A total of 2,015 patients were included with 898 (44.6%) prescribed latanoprost/timolol FC, 733 (36.4%) prescribed bimatoprost/timolol FC, and 384 (19.1%) prescribed travoprost/timolol FC (Tab. I). Across cohorts, about half of patients were male (p=0.435), the mean age was approximately 72 years (p=0.792), and glaucoma was the diagnosis for >90% of the 1,768 patients for whom a diagnosis was recorded (p=0.557). Within each cohort, larger proportions of patients came from more affluent areas, with approximately 30% living in Townsend score 1 areas (most affluent), which was slightly higher than the overall THIN population (approximately 25%) (28). There was no evidence that the proportions varied across cohorts (p=0.332). Prior to the index date, hypertension was the most prevalent comorbidity in each cohort (approximately 50% of patients had a record of hypertension), followed by diabetes, renal failure, cardiovascular disease, and asthma (Tab. I). There was no evidence of any differences in distributions of comorbidities among the cohorts (p>0.15 for each comorbidity). At baseline, fewer than 10% of patients in any cohort had undergone a glaucoma-related laser or other glaucoma-related ocular procedure (p=0.160); however, other ocular glaucoma-related procedures were more common among those treated with bimatoprost/timolol FC (p=0.017).
Baseline Demographic and Medical Characteristics a
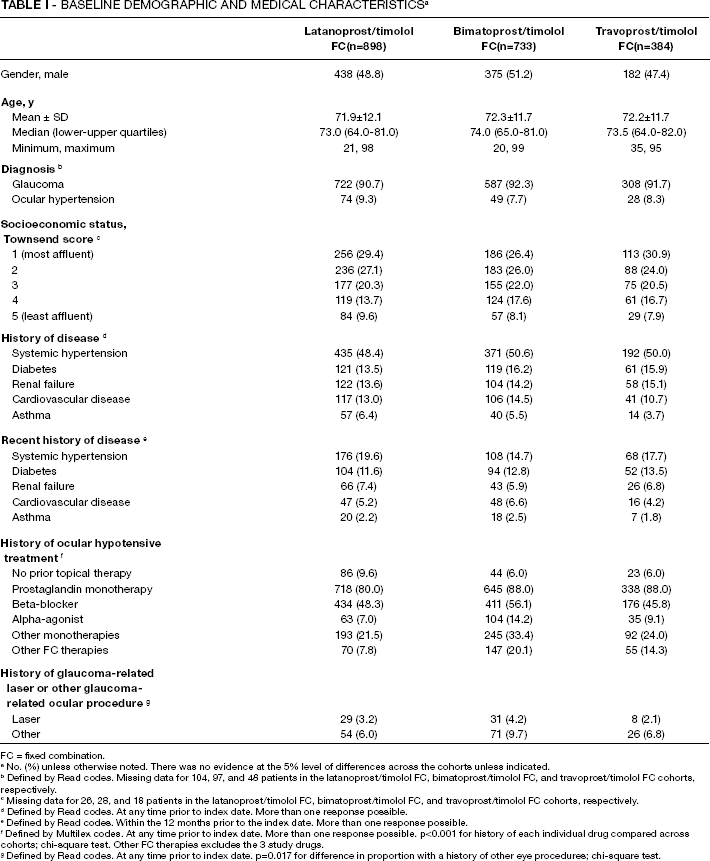
FC = fixed combination.
No. (%) unless otherwise noted. There was no evidence at the 5% level of differences across the cohorts unless indicated.
Defined by Read codes. Missing data for 104, 97, and 48 patients in the latanoprost/timolol FC, bimatoprost/timolol FC, and travoprost/timolol FC cohorts, respectively.
Missing data for 26, 28, and 18 patients in the latanoprost/timolol FC, bimatoprost/timolol FC, and travoprost/timolol FC cohorts, respectively.
Defined by Read codes. At any time prior to index date. More than one response possible.
Defined by Read codes. Within the 12 months prior to the index date. More than one response possible.
Defined by Multilex codes. At any time prior to index date. More than one response possible. p<0.001 for history of each individual drug compared across cohorts; chi-square test. Other FC therapies excludes the 3 study drugs.
Defined by Read codes. At any time prior to index date. p=0.017 for difference in proportion with a history of other eye procedures; chi-square test.
Mean time from the initial glaucoma or ocular hypertension diagnosis recorded in the database to the index date was 6.3±6.4 years for latanoprost/timolol FC, 7.1±6.3 years for bimatoprost/timolol FC, and 6.1±6.8 years for travoprost/timolol FC (p<0.001). Overall, 153 patients, 7.6% of the total study cohort, had not been treated previously with a topical ocular hypotensive agent (Tab. I). More than 80% in each cohort had a history of treatment with prostaglandin monotherapy. Relatively more patients prescribed bimatoprost/timolol FC had a history of treatment with a beta-blocker, an alpha-agonist, prostaglandin monotherapy (although similar to the travoprost/timolol FC cohort), other monotherapies, or other FCs (p<0.001 for each 3-way comparison of individual agents).
Nearly all patients (1,862/2,015 [92.4%]) had 365 days of follow-up after the index date. Mean duration of follow-up was comparable across cohorts ranging from 350.5±57.3 days for those treated with travoprost/timolol FC to 357.0±44.1 days in the latanoprost/timolol FC cohort. During follow-up, ≥92% of patients in each cohort received at least one more index prescription after the index date. Half (50.2%) of all patients did not receive any topical treatment other than the index FC (Tab. II). Prostaglandin monotherapies and other monotherapies (other than beta-blockers and alpha-agonists) were prescribed for approximately 20% to 30% of those in each study cohort during follow-up. Proportions of patients receiving other topical treatments were similar except that more of those initially prescribed bimatoprost/timolol FC were prescribed other monotherapies during follow-up (p=0.001). During the follow-up period, fewer than 1% of patients in any cohort underwent laser procedures (p=0.421), and 2% to 3% of patients in any cohort underwent other eye procedures (p=0.154).
Topical Ocular Hypotensive Prescriptions During Follow-up (Including Index Date), n (%)
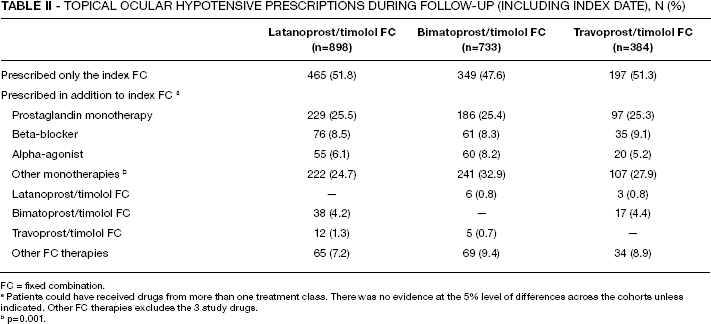
FC = fixed combination.
Patients could have received drugs from more than one treatment class. There was no evidence at the 5% level of differences across the cohorts unless indicated. Other FC therapies excludes the 3 study drugs.
p=0.001.
As shown in Figure 1, 12-month persistence was similar across treatments: latanoprost/timolol FC, 38.2% (343/898); bimatoprost/timolol FC, 38.6% (283/733); travoprost/timolol FC, 38.3% (147/384; p=0.985 for 3-way comparison). Among persistent patients, statistically similar proportions of patients in each cohort received only the index FC (p=0.599). Among nonpersistent patients, there was some evidence (p=0.013) of a difference across cohorts in the proportions of changes in therapy (restart, switch, discontinue, other), with slightly more of those receiving bimatoprost/timolol FC restarting index therapy following a gap. Approximately 80% of patients in each FC cohort continued the index FC therapy during follow-up, i.e., either persisted with or restarted the index FC (p=0.098).
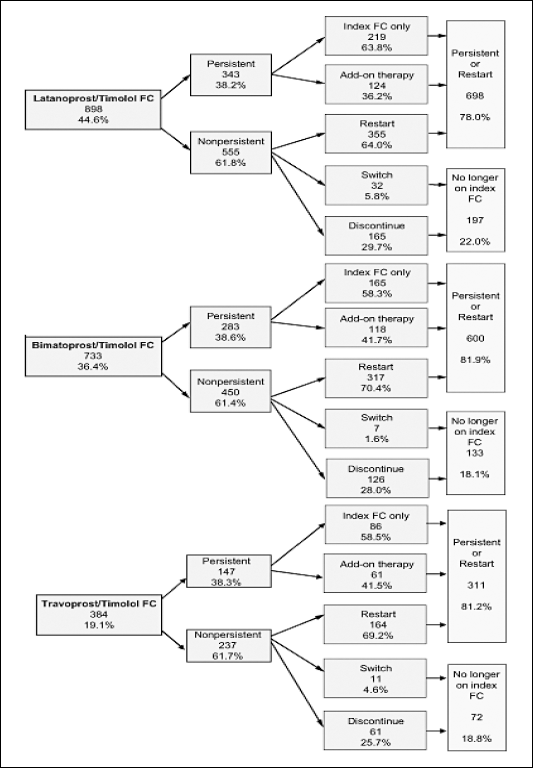
Continuation of fixed combination (FC) therapy over 12 months. Nonpersistence categories exclude 3 patients in the latanoprost/timolol FC cohort and 1 in the travoprost/timolol FC cohort who received a study drug other than the index drug before restarting the index drug; these patients could not be classified as restarting or switching according to study definitions (other nonpersistent).
Mean time to therapy change among nonpersistent patients was similar across cohorts: latanoprost timolol FC, 143.3±89.8 days; bimatoprost/timolol FC, 151.0±87.9 days; travoprost/timolol FC, 151.8±87.7 days (p=0.095; Fig. 2). Once time to change was accounted for, along with the baseline covariates of interest, there was no evidence that the likelihood of persistence changed according to cohort. However, there was evidence that the likelihood of persistence changed according to age (p<0.0001) and history of treatment with a prostaglandin monotherapy (p=0.005, Tab. III). For each 1-year increase in age there was a 1% reduction in the likelihood of changing therapy (hazard ratio 0.99; 95% confidence interval [CI] 0.98-0.99) and patients who had been prescribed prostaglandin monotherapies prior to index were 19% less likely to change therapy than those who had not been prescribed prostaglandin monotherapies prior to the index date (hazard ratio 0.81; 95% CI 0.69-0.94) adjusted for the other baseline covariates. The Townsend score was included in a separate analysis as missing data for this variable reduced the sample size to 1,943 patients. Adjusting for Townsend score did not alter the results and the score was not associated with the likelihood of changing therapy. Among nonpersistent patients who restarted the index agent, the time between the last index FC prescription and the restart date was similar across the drug cohorts with means ranging from 86.1±38.2 day in the latanoprost/timolol FC cohort to 88.9±34.3 days among those prescribed bimatoprost/timolol FC (p=0.224).
− Hazard Ratios for Nonpersistence with Index FC, N=2,015 a
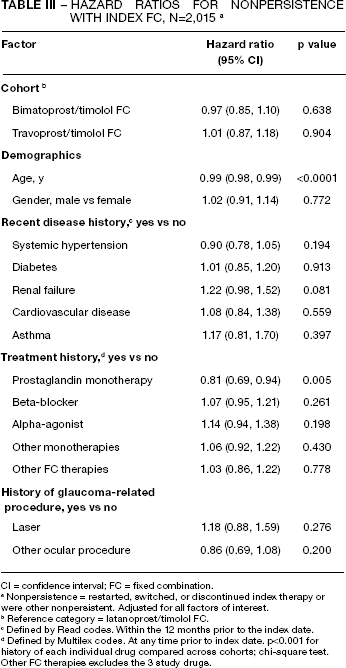
CI = confidence interval; FC = fixed combination.
Nonpersistence = restarted, switched, or discontinued index therapy or were other nonpersistent. Adjusted for all factors of interest.
Reference category = latanoprost/timolol FC.
Defined by Read codes. Within the 12 months prior to the index date.
Defined by Multilex codes. At any time prior to index date. p<0.001 for history of each individual drug compared across cohorts; chi-square test. Other FC therapies excludes the 3 study drugs.
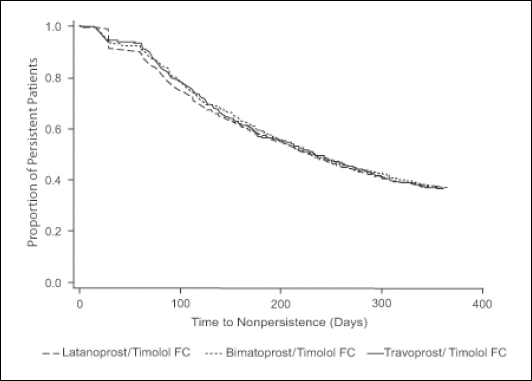
Kaplan-Meier curve for time to nonpersistence with index fixed combination (FC). Nonpersistence = restarted, switched, or discontinued index therapy or were other nonpersistent.
Discussion
In this evaluation of information from the THIN database, persistence across the latanoprost/timolol FC, bimatoprost/timolol FC, and travoprost/timolol FC cohorts was approximately 38%. In general, these results confirm those of previous studies of ocular hypotensive monotherapies demonstrating that uninterrupted use by glaucoma patients is relatively poor (8-16, 29).
In the present study, there was no evidence from the unadjusted or adjusted analyses that persistence differed between cohorts. Persistence with each of the 3 evaluated prostaglandin FCs was higher than the persistence reported in the Glaucoma Adherence and Persistence Study (GAPS) for latanoprost, bimatoprost, and travoprost monotherapies (10, 16). In GAPS, 11%, 9%, and 5% of patients were persistent over 12 months with latanoprost, bimatoprost, and travoprost, respectively, compared with 38% to 39% of those in each FC cohort evaluated herein. As in GAPS, the present study also analyzed persistence accounting for restarts, a critical consideration when evaluating long-term glaucoma treatment (20, 30). Among patients prescribed latanoprost, bimatoprost, and travoprost monotherapies, 68%, 61%, and 58%, respectively, were either persistent or restarted the index medication after 12 months (10, 16). These proportions of persistent patients were substantially lower than reported in this study whereby approximately 80% in each FC cohort continued the index medication at least intermittently or in combination with another medication after 12 months. A prospective, noninterventional study (18) of patients switched to latanoprost/timolol FC for medical reasons reported that 97% of patients remained on therapy throughout the 6-month follow-up period; however, differences in methodologies and duration of follow-up limit the ability to make direct comparisons with the current findings. While several studies (10, 12, 14, 16, 17) found persistence to be higher with latanoprost than with travoprost or bimatoprost, the present study found that persistence was similar across the 3 prostaglandin FCs. This difference is difficult to explain but may reflect differences in study designs and population characteristics. Few studies (18, 19) have focused on persistence with FCs and none, to our knowledge, has compared persistence across prostaglandin FCs. Patients prescribed FCs may exhibit greater persistence than those prescribed either monotherapies or unfixed combination therapies for reasons including convenience owing to simplicity of dosing (19) (European Glaucoma Society Terminology and Guidelines for Glaucoma, 2nd ed. Savona, Italy: DOGMA, 2008. Available at: http://www.eugs.org/ebook.asp. Accessed July 28, 2009) and heightened concern about vision loss (30). Recent research (19) compared persistence among patients prescribed dorzolamide/timolol FC versus 2 or 3 separate topical medications using a retail pharmacy claims database (n=37,979). There was evidence that a greater proportion of patients prescribed the FC completed 1 year of treatment without discontinuing than patients in the cohorts prescribed either 2 or 3 separate agents (35.3% vs 27.2% vs 23.9%, respectively; p<0.0001 for comparisons with the FC). The authors conclude that fixed combinations can “positively contribute to patient persistence” by simplifying dosing regimens. Moreover, the need for multiple ocular hypotensive agents suggests the presence of disease that is difficult to control. Patients with more advanced disease may be more concerned about potential vision loss from glaucoma and thus are more motivated to persist with the medication regimen. Poorer adherence (lower ratio of days of supply of medication dispensed divided by the days between pharmacy fulfillments) has been reported among glaucoma patients who did not believe that nonadherence increased their risk for reduced vision (30).
The higher persistence rate demonstrated with the prostaglandin FC compared with the prostaglandin monotherapies may also be reflected in the increased IOP-lowering effect of the prostaglandin FC compared to the prostaglandin monotherapies. Meta-analyses and various efficacy studies of individual monotherapies and their corresponding prostaglandin FCs have consistently demonstrated that the prostaglandin FC will result in increased IOP lowering compared to the monotherapies (31-36).
In the present study's relatively older population (mean age, approximately 72 years), multivariable analyses demonstrated that the likelihood of persistence increased with patient age. This finding is comparable to findings of a study by Nordstrom et al (11) in which those 40 to 49 years were found to be at higher risk of discontinuation than those in older age groups. In the current study, those previously treated with a prostaglandin monotherapy were more likely than those without this therapeutic history to persist with the index FC. All 3 FCs have been shown to be effective and well-tolerated (37-42). The fact that physicians prescribed one of the study FCs for patients with a history of prostaglandin use suggests that, while additional IOP lowering was desirable, tolerability with prostaglandin therapy was at least satisfactory. After the need for increased IOP lowering, adverse events have been found to be the most common reason given by physicians for switching ocular hypotensive therapies (43% and 19%, respectively) (16).
Improving the relatively low rate of persistence documented herein and by previous researchers remains challenging. Regularly assessing the medication regimen, ensuring that the patient knows how to correctly instill drops and minimize wastage, and being attuned to cost issues have been suggested as ways to improve patient persistence with ocular hypotensive therapies (43). A recent Cochrane review (44) of 8 randomized studies of interventions to improve adherence to ocular therapy concluded that simplified dosing regimens, reminder devices, education, and individualized care planning resulted in improved adherence rates; these same approaches might also improve persistence rates.
This study has several potential limitations. The THIN database did not contain information on whether one or both eyes were treated for individual patients or on the number of drops needed per eye. As a result, some patients falling into the restart category may have been persistent and therefore persistence may have been underestimated, a limitation that applied equally across treatment cohorts. The longer mean time from diagnosis to the index date and the greater number of eye procedures among those in the bimatoprost/timolol FC cohort suggests that these patients may, on average, have had glaucoma longer before being initiated on the FC than those in the other cohorts—a difference that may have affected persistence. As the relative timing of add-on therapy was not evaluated, any interpretation from these findings should be made with caution. Moreover, data in THIN reflect issued, not redeemed, prescriptions; however, it is likely that the majority of patients with chronic conditions such as glaucoma filled their prescriptions. Finally, patients could have received their first glaucoma diagnosis outside of primary care. Therefore, the time since first diagnosis may have been underestimated; however, there is no reason to expect that this potential bias would have been unequally distributed across treatment cohorts.
A strength of the study is its observational design and large patient population. Moreover, the findings should be generalizable to the UK population because the THIN database has been shown to be representative of recipients of treatment in UK primary care (20). Future research could evaluate the effect of persistence on glaucoma-related treatment outcomes such as IOP or eye surgery.
Conclusions
The largest proportion of first-time recipients of prostaglandin/beta-blocker FC products treated in UK primary care was prescribed latanoprost/timolol FC. Twelve-month persistence was similar across the 3 fixed prostaglandin/beta-blocker combinations evaluated. However, fewer than 40% of patients in any cohort were persistent, suggesting that long-term use of ocular hypotensive therapy remains a problem for many patients. The study had several limitations, including the possibility that some patients included in the restart category may in fact have been persistent. The extent to which this resulted in an underestimation of persistence is unknown; however, the limitation applied equally across cohorts. Nevertheless, it seems reasonable to conclude that persistence with ocular hypotensive medication remains suboptimal and that it is important for clinicians to identify patients who are not continually persistent, to prescribe therapies that encourage persistence, and to educate patients on the importance of long-term medication use.
Footnotes
ACKNOWLEDGEMENTS
Editorial support, including contributing to the first draft of the manuscript, revising the paper based on author feedback, and styling the paper for journal submission, was provided by Jane G. Murphy, PhD, of Zola Associates, and was funded by Pfizer Ltd, UK.