
Abstract
Purpose
To evaluate contrast sensitivity function (CSF) and color vision after implantation of either orange or yellow-tinted intraocular lenses (IOLs).
Methods
Fifty-six eyes of 28 cataract patients who had bilateral implantation of orange-tinted (PC440Y Orange, Ophtec), yellow-tinted (AcrySof Natural SN60AT, Alcon), or clear (AcrySof SA60AT, Alcon) IOLs were examined. Six months postoperatively, monocular CSF under photopic and mesopic (with and without glare) conditions were measured using the Functional Visual Analyzer. Color discrimination was determined with the Farnsworth-Munsell 100-Hue test.
Results
Patients implanted with orange-tinted, yellow-tinted, or clear IOLs displayed similar CSF values, with no statistically significant differences at any spatial frequency (p>0.05). There were no statistically significant differences in chromatic discrimination among the 3 groups of patients (p>0.05).
Conclusions
Orange or yellow blue-filtering IOL implantation is comparable to a clear IOL in terms of photopic and mesopic contrast sensitivity or color discrimination.
Introduction
The relationship between human eye tissues and light-wavelength blockage has been extensively studied (1-3). While the cornea mainly protects the retina from ultraviolet (UV) radiation shorter than 300 nm, the crystalline lens blocks wavelengths between 300 and 400 nm. The crystalline lens properties change with aging, and its yellowing results in a progressive increase in absorbance of short-wavelength light. In order to imitate the UV-filtering properties of the natural lens after cataract surgery, intraocular lenses (IOLs) with UV radiation–filtering chromophores have been used as standard since suggested by Mainster (4) and Lindstrom and Doddi (5) in 1986. More recently, IOLs that also attenuate visible short-wavelength blue light (from 400 to 500 nm) were introduced in an attempt to more closely approximate the protective properties of the natural lens (6, 7). A recent study by Sparrow et al (8) suggests that these blue-light absorbing IOLs protect lipofuscin-containing retinal pigment epithelial cells and thus help reduce the risk for macular degeneration or its progression. In this way, manufacturers have developed new IOLs with different color-filtering chromophores which differ in their transmittance properties.
Available IOLs range in color from fully transparent through light yellow up to orange. Particularly, the AcrySof Natural SN60AT IOL (Alcon) and the PC440Y Orange IOL (Ophtec) have been designed with a material that includes a blue light–absorbing chromophore (yellow and orange-colored chromophore, respectively) developed to mimic the light-transmittance characteristics of the natural lens at wavelengths below 500 nm. These IOLs not only filter UV radiation but also around 50% of the light between 380 and 500 nm (blue), theoretically providing the retina with better light protection (9).
It is important to answer the logical question of whether yellow and orange-tinted IOLs could modify visual performance due to the reduction in the visible spectrum of the blue band. Several studies assessing contrast sensitivity function (CSF) and color vision in patients implanted with blue-filtering IOLs yielded controversial results, some reporting no differences in photopic CSF and color discrimination (10-12), others showing changes in color perception (13, 14).
The purpose of the present study was to determine the photopic and mesopic CSF as well as color discrimination in patients implanted with 2 color-tinted IOL models, the orange-tinted PC440Y IOL and the yellow-tinted AcrySof Natural SN60AT IOL, and to compare them with a clear IOL, the AcrySof SA60AT. The CSF reports on visual performance in different spatial frequencies and contrast levels, which is particularly useful in patients undergoing cataract or refractive surgery (15-21). Color vision abnormalities could be discarded using the FM-100 Hue test, which is one of the most specific tests to assess chromatic discrimination in clinical practice.
Patients and Methods
Enrollment and baseline
This prospective consecutive nonrandomized interventional clinical study comprised patients having bilateral cataract surgery who were divided into 3 groups depending on the IOL implanted: the orange-tinted PC440Y IOL, the yellow-tinted AcrySof Natural SN60AT IOL, and the clear AcrySof SA60AT IOL. All the patients received the same model of IOL in both eyes. Written informed consent before surgery in accordance with the Declaration of Helsinki was provided, and institutional review board approval was obtained from the hospital ethics committee.
Inclusion criteria were cataract causing a significant reduction in visual quality and potential visual acuity determined by dilated near-pinhole test of 0.3 logMAR or better in both eyes. Exclusion criteria were ocular disease other than cataract, including uveitis, amblyopia, glaucoma, retinal detachment, diabetic retinopathy, macular degeneration, corneal opacities, previous corneal refractive surgery, and neuro-ophthalmic disease.
Preoperatively, all patients had a full ophthalmologic examination including refractive status, slit-lamp evaluation, tonometry, and funduscopy. The corrected distance visual acuity (CDVA) at 6 m was assessed using a calibrated Snellen chart. Corneal refractive power was measured with an automated keratorefractometer (KR-7000, Topcon), and axial length (AL) was measured using noncontact optical biometry (IOLMaster, Carl Zeiss Meditec AG). The power of the IOL was selected for a target of emmetropia applying the SRK/T formula for eyes with an AL of more than 22.0 mm and the Hoffer-Q formula for eyes with an AL less than 22.0 mm.
Intraocular lens characteristics
The IOLs involved in the present study are shown in Figure 1. The orange-tinted PC440Y Orange IOL is a biconvex 3-piece silicone IOL made with clear polysiloxane elastomer with covalently bound orange chromophore and UV absorber. The IOL has a 12.5 mm overall length, a 5.8 mm square edge optic, and brown PMMA haptics with C-fit loop and 10° angulation.
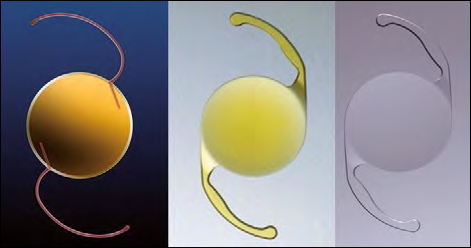
The 3 intraocular lenses (IOLs) involved in the present study: the PC440Y Orange IOL (left), the AcrySof Natural SN60AT IOL (center), and the AcrySof SA60AT IOL (right).
The yellow-tinted AcrySof Natural SN60AT IOL and the clear AcrySof SA60AT are biconvex monoblock hydrophobic C-loop designed acrylic IOLs, with a 13.0 mm overall length and a 6.0 mm optic. They are optically and structurally identical except for the presence of the yellow blue-light filter in the former.
Surgical technique
Two surgeons (G.M. and A.F.-P.) performed all operations; the second eye surgery was performed within 1 week of the first. The technique included phacoemulsification through a 2.75-mm clear corneal incision placed on the steepest meridian, a 5.0-mm capsulorhexis, and symmetric implantation of the IOL in the capsular bag.
Postoperative topical therapy included diclofenac 0.1% (Dicloabak) and tobramycin 0.3%–dexamethasone 0.1% (TobraDex) for 3 weeks.
Postoperative assessments
Evaluations were performed 1 day, 1 week, and 1 and 6 months after the second eye surgery and included refractive status, slit-lamp evaluation, tonometry, and fundoscopy. Contrast sensitivity and color vision were tested at 6 months of follow-up by the same ophthalmic technician masked as to the IOL type.
Contrast sensitivity was tested monocularly using best correction for distance under photopic conditions (85 cd/m2) and under mesopic conditions (3 cd/m2) with and without glare, using the Optec® 6500 tester with the functional acuity contrast test (Stereo Optical Co., Inc.). This test allows the presentation of sine-wave gratings at different spatial frequencies (1.5, 3, 6, 12, and 18 cycles per degree [cpd]), with increasing contrast values. Absolute values of log10 contrast sensitivity were obtained for each combination of eye and spatial frequency, and means and standard deviations (SD) were calculated. Patients remained 10 minutes inside the testing room under mesopic conditions for an appropriate adaptation before mesopic contrast sensitivity was measured.
Color vision was evaluated monocularly with distance correction using the Farnsworth-Munsell (FM) 100-Hue Test under photopic conditions (22). An HD 9221 photometer (Delta OHM S.r.L.) was used to measure the lighting conditions in the room in which Farnsworth-Munsell was performed to ensure equal lighting levels for all patients at all testing sessions. Under photopic conditions, luminance was 90 cd/m2 and illumination was 450 lux. The FM 100-Hue Test has not been previously validated for use under mesopic conditions (13, 23). This color test contains 85 colored caps organized in 4 boxes of 20 to 22 caps. The first and the latest of these caps are fixed in each box, being the color reference caps, whereas the other caps are loose and can be removed by the examiner. According to the color test instructions, patients should place the colored caps in the correct order to obtain a gradual progression sequence of hue. When the 4 boxes were completed, the examiner wrote the results without disclosing them to the patients. The FM error scores were calculated as described by Kinnear (24). The error score for each cap was calculated by adding the difference between the cap's number and the number of the caps the subject placed on both sides of it. Therefore, the score for a cap correctly placed would be 2.
Data management and statistical analysis
Visual acuity values were converted to logMAR notation for statistical purposes.
The revised abbreviations for reporting visual acuity values proposed by Kohnen were used (25). Statistical analysis was performed using SPSS for Windows software (version 11.5, SPSS, Inc.). The Kruskal-Wallis test was used to compare results between the 3 groups. Results are presented as the mean ± SD; a p value of 0.05 was considered statistically significant.
Results
All patients completed the 6-month follow-up and data were collected from 56 eyes of 28 patients (13 men, 15 women) with a mean age of 68.3±0.4 years (SD). The mean pupil size was 3.6±1.1 mm under photopic conditions and 5.8±1.0 mm under mesopic conditions. There were no intraoperative complications. There were no cases of iris trauma, posterior capsule opacification, or IOL decentration or tilt.
The 3 groups of treatment were comparable before surgery (Tab. I) with no statistically significant differences regarding age, axial length, keratometry, preoperative CDVA, or preoperative spherical equivalent (SE). Moreover, cataract surgery with the 3 different IOL models yielded similar refractive outcomes with no statistically significant differences with regards to postoperative CDVA or residual SE.
Preoperative and Postoperative Data of Patients Implanted with Orange-Tinted, Yellow-Tinted, and Clear IOLS
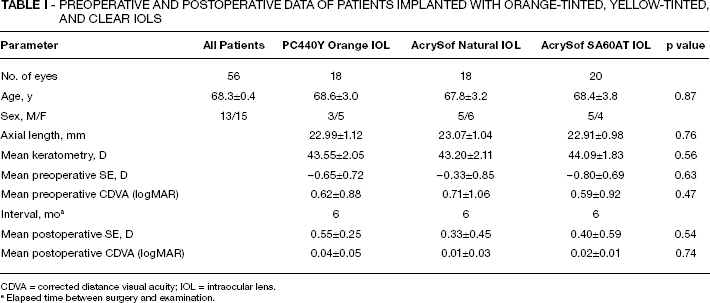
CDVA = corrected distance visual acuity; IOL = intraocular lens.
Elapsed time between surgery and examination.
Contrast sensitivity
Photopic distance CSF was similar for the 3 IOLs (Fig. 2) with no statistically significant differences at any tested frequency (1.5 cpd, p=0.49; 3 cpd, p=0.72; 6 cpd, p=0.87; 12 cpd, p=0.23; 18 cpd, p=0.11).
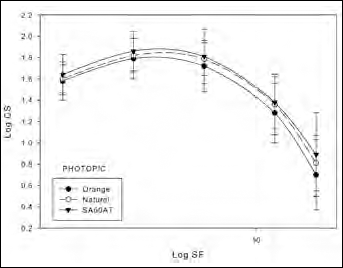
Logarithmic contrast sensitivity (CS) values under photopic conditions with the PC440Y Orange, the AcrySof Natural SN60AT, and the AcrySof SA60AT intraocular lenses.
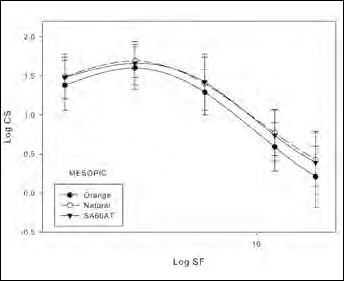
Figure 3 and 4 plot the CSF under mesopic conditions with and without glare, respectively, showing no statistically significant differences between the 3 IOLs. As expected, CSF under mesopic conditions showed lower values than those obtained under photopic conditions for all range of spatial frequencies, particularly for high frequencies and with glare.
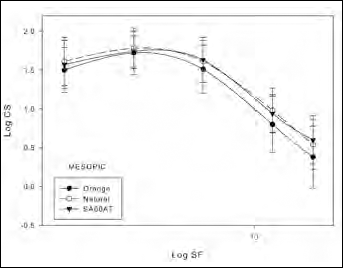
Contrast sensitivity (CS) function under mesopic conditions without glare with the PC440Y Orange, AcrySof Natural SN60AT, and AcrySof SA60AT intraocular lenses.
Contrast sensitivity (CS) function under mesopic conditions in the presence of a glare source with the PC440Y Orange, AcrySof Natural SN60AT, and AcrySof SA60AT IOLs.
Color vision
Table II shows that there were no statistically significant differences between orange-tinted, yellow-tinted, and clear IOLs in color perception under photopic conditions (p=0.56). However, the total error score obtained with orange-filtering IOL was higher than with the other 2 IOL models.
Error Scores for the Farnsworth-Munsell 100-hue Test with the Orange-Tinted, Yellow-Tinted, and Clear Iols
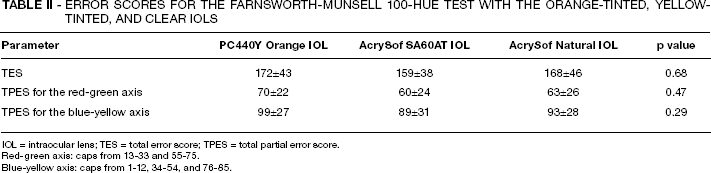
IOL = intraocular lens; TES = total error score; TPES = total partial error score.
Red-green axis: caps from 13-33 and 55-75.
Blue-yellow axis: caps from 1-12, 34-54, and 76-85.
Discussion
The main theoretical benefit of blue-filtering IOLs is retinal protection from blue light by partially absorbing the short wavelength range of the visible spectrum. Blue-filtering IOLs are intended to mimic the natural transmittance characteristics of the adult human crystalline lens protecting an aging retina from visible blue light. However, these IOL should not interfere with natural vision. Previous studies suggest that yellow filters may even improve visual parameters such as visual clarity, visual performance under glare conditions, and CSF for medium spatial frequencies under photopic and mesopic conditions (26, 27).
The present study compares the CSF and chromatic discrimination provided by 2 blue-filtering IOL models: the orange-tinted PC440Y Orange IOL and the yellow-tinted AcrySof Natural SN60AT IOL, with the CSF and color vision provided by the clear AcrySof SA60AT IOL. There are no previous reports about the CSF or chromatic discrimination of patients implanted with an orange-tinted IOL. According to our results, CSF values for the 3 IOL models at 2 luminance levels and for all spatial frequencies were similar, suggesting that visual performance under photopic and mesopic conditions (with or without glare) is not impaired after color-filtering IOL implantation.
Previous studies (26-28) report that the use of yellow filters by healthy phakic patients improved the image contrast and consequently their CSF. This improvement may be attributed to a decrease in the effects of chromatic aberrations (29, 30), a brightness increment (31), scattering reduction (32), or a decrease in lenticular fluorescence (33). The effects of chromatic aberration are more noticeable in high spatial resolution–demanding tasks. Considering that visual acuity, one of the tasks most sensitive to the presence of these aberrations, is not improved with the use of tinted lenses, the effect of the reduction in chromatic aberrations due to the filter would probably not improve the patients’ performance in contrast discrimination tasks (29, 30). Kinney et al (28) suggest that the origin of this enhancement is the response increment of the opponent chromatic mechanisms due to the removal of the negative contribution of short wavelengths. Also, the decrease of blue light reduces the scattering effects, which would justify the poor performance of these filters under glare and poor atmospheric conditions (32). It has been found that the short wavelengths removed by the cutoff filters produce fluorescence effects in the chromophore-containing proteins present in the crystalline lens of the human eye (33). Taking this into account, it is reasonable to believe that the different contributions of the phenomena discussed above result in an increase in CSF. In this way, de Fez et al (14) have shown that yellow filters enhance low achromatic contrast for middle and high spatial frequencies.
It is important to insist on the effect of color filter on contrast sensitivity. It depends on spectral transmittance. In a recent study, Artigas et al (9) compare the spectral transmission of different IOLs with UV or blue-light filters under artificial illumination and sunlight. They show that all the IOLs provide good UVC (200-280 nm) and UVB (280-315 nm) protection, being in the UVA (315-380 nm) range where the different IOLs manifest different degrees of absorption, with the orange and yellow filters providing greater UV photoprotection. The filters that favor better reception of visible light (380-780 nm) are those that transmit this radiation close to 100%. A possible balance between photoprotection and photoreception could be an IOL with a sharp cutoff filter near 400 nm and a maximum transmittance around 100% (9). The PC440Y Orange IOL filters around 50% of the light that reaches between 380 and 500 nm (blue) transmitting only 10% at 427 nm. Similarly, AcrySof Natural SN60AT IOL filters blue radiation with low transmittance, about 30% at 430 nm. The present results do not reveal any significant difference among the 3 IOL models in CSF under any lighting condition or with glare for any spatial frequency. Therefore, the main reason to explain the differences found in and between previous studies may be related to the different spectral transmittance of each filter.
In relation to color vision assessment, some studies evaluating yellow filters found a decrease in color perception. The common factor has been light-transmission cutoff at wavelengths greater than the 500 nm range, particularly using darker filter colors such as orange, brown, or darker yellow, which have been associated with decreased color sensitivity and tritan color defects (13, 14, 31, 34, 35). The present study shows a higher total error score after orange-filtering IOL implantation than with the other 2 IOL models, but not reaching statistical significance. These outcomes agree with reports from Rodríguez-Galietero et al (10) that revealed no color discrimination alterations in eyes implanted with the AcrySof Natural IOL and comparable results between eyes implanted with yellow and clear IOLs. Kinnear and Sahraie (36) found similar results for a population without chromatic discrimination alterations. In contrast to this, De Fez et al (14) reported that yellow filters cause a tritan-like defect with discrimination loss in the yellow-purplish region. As previously discussed, differences in spectral transmittance might be the reason for the differences between the results found in the present study and those reported in previous literature (14). The differences in transmittance of the PC440Y Orange IOL, AcrySof Natural SN60AT IOL, and the AcrySof SA60AT IOL are not enough to induce divergence in color vision between patients implanted with the different IOLs. Thus, the implantation of these blue light–filtering IOLs does not adversely affect color vision.
In conclusion, the present study shows no significant worsening of visual function after blue light–filtering IOL implantation. The PC440Y Orange IOL is comparable in terms of visual performance with the AcrySof Natural SN60AT IOL. No statistically significant differences in CSF under any lighting condition or color vision were found between them and the clear AcrySof SA60AT IOL after 6 months of follow-up. Orange and yellow IOL filters may be best suited for cases requiring special retinal protection. Color-tinted IOLs may be recommended for eyes at high risk of developing macular degeneration. The limited number of patients and the interindividual design should be considered as potential limitations of the study, and further investigation with larger samples and intraindividual design would be desirable for stronger conclusions. The controversial results in visual performance between the present and previous studies promote further debate about the use, advantages, and drawbacks of blue light–filtering IOLs.