
Abstract
Purpose
Charles Bonnet syndrome plus is an exceedingly rare variant of this disorder. The variant has been described in patients with sight impairment and severe hypoacusis, and is usually characterized by complex visual and auditory—musical—hallucinations that the patients recognize as unreal.
Methods
Case report.
Results
A 75-year-old woman diagnosed with Usher syndrome presented with visual acuity of light perception in both eyes, which did not improve with the use of a pinhole occluder. She also had coptosis in right ear and severe hypoacusis in left ear, confirmed through audiometry. Audiometric tests were normal once the implant and the hearing aid were connected. The patient was referred to the Neuro-Ophthalmology Unit after recounting experiencing complex visual hallucinations, as well as auditory (musical) ones at night after disconnecting the hearing aid. She described the latter as a nightly occurrence of hearing “cabaret music.” Nevertheless, she was aware of reality and of her sensory impairments. The patient was diagnosed at the interdisciplinary Neuro-Ophthalmology Unit, and began pharmacologic treatment with clear improvement.
Conclusions
Knowledge of Charles Bonnet syndrome and in particular of Charles Bonnet syndrome plus—due to its infrequency—on the part of ophthalmologists is fundamental to adequately diagnose and treat this rare disorder.
Introduction
Charles Bonnet syndrome (CBS) is characterized by complex stereotyped and elaborate visual hallucinations. These are usually recurrent, persistent, and appear unexpectedly. The patient does not present cognitive deficiencies, thus interpreting them as unreal. Hallucinations can be simple, such as basic geometric figures, or complex and structured (1). The great majority last less than 10 minutes and are usually repetitive in persistent fixed stereotypes. Ninety percent of hallucinations do not have any personal significance to the patient. The cause of these hallucinations is unknown; however, possible triggering factors include fatigue, stress, low room lighting, and blinding lights. Charles Bonnet syndrome has also been linked to social isolation, cognitive impairment, sensory privation, and low quality social interaction.
No co-existence of other types of sensory hallucinations is of great importance in CBS, since their presence would signify an evident psychiatric pathology. However, the exceedingly rare variant CBS-plus has been described in patients with vision impairment and severe hypoacusis; it is typically characterized by musical hallucinations unaccompanied by voices or strange noises (2, 3).
Case report
A 75-year-old woman, diagnosed 25 years ago with Usher syndrome, presented a visual acuity (VA) of light perception in both eyes, which did not improve with the use of a pinhole occluder. Intraocular pressure was normal in both eyes. Biomicroscopy revealed iridodonesis and aphakia in both eyes. Funduscopy revealed intraretinal bone-spicule pigmentation, as well as see-through of choroidal vessels (Fig. 1). The patient also presented coptosis in right ear and severe hypoacusis in left ear, which were confirmed through audiometry (Fig. 2). Audiometric tests were normal once both the implant and the hearing aid were connected (Fig. 3).
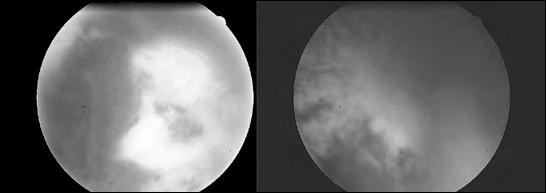
Funduscopy showing atrophy and spicules.
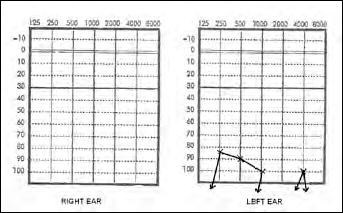
Audiometric results, both ears without implants. Observe the lack of response in the right ear and the severe hypoacusis in the left, with a hearing loss of 98 dB on conversational frequencies.
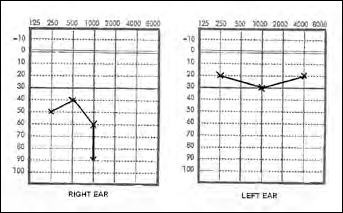
Audiometric results, both ears with implants. Normal results in both the right (implant connected) and the left (hearing aid connected) ears.
The patient was referred to the Neuro-Ophthalmology Unit after recounting complex visual hallucinations consisting of visions of unknown people wandering around her, but without interacting with her. She also explained that at night, after disconnecting the hearing aid, she would hear music that she described as “cabaret music,” this being an almost nightly occurrence. The patient was aware of the situation, recounting the facts in consciousness of her sensory impairments.
The patient was assessed and treated at the interdisciplinary CBS unit, formed by the Departments of Ophthalmology, Neurology, and Psychiatry at Hospital Clínico San Carlos. Initial assessment ruled out other pathologies through clinical examination, extensive blood testing, and imaging testing, in order to justify the diagnosis. Thus, the patient was put under treatment with haloperidol, 10 drops per day, together with quetiapine, 300 mg per day. After 3 months, the patient did not present any clear improvement, so the treatment was suspended and instead she was prescribed donepezil 5 mg a day, which has so far resulted in a clear improvement in the symptoms.
Discussion
Estimated prevalence of simple visual hallucinations in patients with ocular pathologies is between 41% and 59%, decreasing to between 11% and 15% for complex visual hallucinations. However, case studies show a prevalence of between 1.84% and 3.15% due to ignorance on the part of the doctor, and to fear of being catalogued as mentally ill on the part of the patient (2, 3). The majority of the cases described correlate with populations between 75 and 84 years of age, with a slight predominance in women. Most cases are associated with loss of vision. Development can be episodic, cyclic, or chronic. Duration is usually under 18 months, though cases have been described with several or more years of evolution.
Pathologies most commonly associated with the condition are macular degeneration associated with age, cataracts, corneal opacity, glaucoma, retinal damage, enucleation, optic neuritis, and pigmentary retinosis, among others (4). Nevertheless, it has also been described in patients with good vision and glaucoma, possibly linked to deafferentation of the injured fibers despite preservation of central vision. Some authors describe the appearance of CBS as a process towards dementia. Contributing factors could include appearance of cognitive deterioration, alterations in the sleep-wake cycle, depression, and duration of the symptoms. However, other authors have not found this relationship.
Various theories have been put forward to explain the origin of hallucinations in CBS. With a manifest decrease in visual acuity—a necessary condition for diagnosis of CBS—stimulation of the visual cortex from the retina diminishes, though neural activity does not completely disappear, unlike in blindness. It is then that the so-called process of deafferentation takes place, the consequence of which is hyperexcitability of a specific cortical area in an attempt to compensate on the part of the neuron, through various mechanisms, thus bringing about anatomic and physiologic compensatory changes in the latter. In the presynaptic neuron, the following increase: the size of the terminal buttons, the total number of vesicles in each, the active zone surface, the amount of neurotransmitter released, and the probability of neurotransmitter release. In the postsynaptic neuron, the number of receptors increases, thus allowing a heightened response to any stimulus (4). This increase in the number of receptors occurs primarily for dopamine and serotonin, consequently causing regulation in acetylcholine levels. This is translated in lower levels of the latter in the thalamus, thus causing an indiscriminate and unfiltered perception of the majority of visual stimuli in the retina, since this neurotransmitter intervenes in their selection process (4).
At the same time, response of glutamate N-methyl-D-aspartate (NMDA) receptors increases, while gamma-aminobutyric acid (GABA) decreases, which cause the neurons to be even more excitable.
Charles Bonnet syndrome–plus is an extremely infrequent diagnosis, and only 4 cases have been described, 2 of which were in the article “Charles Bonnet syndrome and musical hallucination” by Aziz et al, where one of the patients describes having auditory hallucinations of ecclesiastic music, while the other reports hearing opera music (5). In the article “Charles Bonnet syndrome with auditory hallucinations: a diagnostic dilemma” by Hori et al, both patients referred to hearing “whistling and applauding” (6).
For adequate treatment of this disorder, accurate diagnosis is essential, which implies ruling out neurologic and psychiatric pathologies. Psychoeducation for patients and their families is fundamental since this is not a mental disorder, and psychotropic drugs should only be used when all previous interventions prove to be ineffective (7). Improvement in the social factors associated with this disorder such as isolation, deprivation, or deterioration of social interaction also aids in the control, and even disappearance, of the symptoms. There is no standardized pharmacologic treatment for CBS, and response is patient specific. Among drugs used in neurology and psychiatry, the following stand out: antipsychotics such as olanzapine, risperidone, and haloperidol; anticonvulsants such as valproate and carbamazepine; or serotonin antagonists such as mirtazapine and cisapride.
Prognosis varies according to the nature and location of the visual damage, and in the majority of cases, the hallucinations disappear spontaneously. On occasion, paradoxically, they cease as the patient progresses towards complete blindness.
Knowledge of CBS and in particular of CBS-plus—due to its infrequency—on the part of ophthalmologists is fundamental to adequately diagnose and treat this rare disorder, and hence to improve patients’ quality of life (1).