
Abstract
Purpose.
To investigate visual function and ocular features in children with attention deficit hyperactivity disorder (ADHD).
Methods.
Fifty-one children underwent a detailed ophthalmologic evaluation. Thirty-two were diagnosed with ADHD, and 19 children with attention deficit disorder (ADD). The mean age was 9.9±3.1 years.
Results.
The average best-corrected visual acuity of the better-seeing eye was 1 (range 0.9-1.25) and 0.96 (range 0.5-1.25) for the fellow eye. Eighteen percent (10) had amblyopia in one or both eyes (3 had strabismic and 7 had ametropic amblyopia). Heterotropia was found in 5 (10%), and absent stereoacuity was found in 3 (6%). Subnormal convergence amplitude was noted in 2 patients (4%). The mean spherical equivalent (SE) of the eyes in this study was 0.17±1.73 (range −5.5 to +7). Twenty-two subjects (43%) had a myopia of −0.50 D or higher. Hyperopia higher than 3.5 D was seen in 10 cases (20%), and astigmatism larger or equal to 1.0 D was observed in 10 patients (20%). With-the-rule astigmatism was by far most common type in the 29 eyes with an astigmatic refractive error (59%). Significant ametropia was detected in 42 (83%) of the patients. In contrast to other studies, we did not find a higher rate of convergence insufficiency or heterotropia.
Conclusions.
Children diagnosed with either ADHD or ADD can present with significant ametropia but infrequent heterotropia.
Introduction
Attention deficit hyperactivity disorder (ADHD) is a prevalent neurodevelopmental disorder characterized by an increase in distractibility. Children being evaluated for attention deficit disorder with and without hyperactivity often have an eye examination as part of their complete physical and psychological workup. Several studies noted a higher rate of ocular abnormalities in this group of children (5, 6). These children would benefit from adequate diagnosis and treatment of any significant ocular pathology. We sought to report in a clinical setting the ocular findings associated with our group of patients with ADHD in comparison to other cited reports in the English medical literature.
Methods
Fifty-five children with the diagnosis of ADHD by the Test of Variables of Attention (TOVA) were seen in the private clinic of T.W.J. We excluded 3 patients with incomplete data and a child with pseudophakia due to traumatic cataract extraction. Data from the remaining 51 patients showed a mean age of 9.9±3.1 years (range 4.2-15.9 years). The group consisted of 31 boys and 20 girls. The children underwent a detailed ophthalmologic evaluation by T.W.J. The ocular examination included several tests. Visual acuity without correction and with correction in each eye was tested separately at a distance of 6 meters with a Snellen E chart or numbers and at near. Stereopsis was tested by using the Titmus test (VAO, Illinois, USA). The orthoptic evaluation was carried out by performing a distance and near target cover and alternate cover tests with and without correction. Convergence and convergence amplitudes were measured with prisms and not with an amblyoscope. Cycloplegic refraction of each eye was carried out with an autorefractometer (Nikon TL 100, Japan) after instilling 2 drops of cyclopentolate 1% 10 minutes apart and waiting for 50 minutes to achieve effective cycloplegia. The cycloplegic refraction by an autorefractometer was confirmed by a manual refraction.
Significant refractive errors were defined as a spherical equivalent (SE) of myopia of −0.50 D or higher, hyperopia equal or higher than 2 D, or astigmatism equal or larger than 1.0 D. Anisometropia was defined as a SE of 1 D or more. The definition of with-the-rule astigmatism was when the axis was between 0 and 30 or 150 and 180 degrees, against-the-rule astigmatism when the axis was between 60 and 120 degrees, and oblique astigmatism when axis was between 30 and 60 or 120 and 150 degrees. The posterior segment of the eye was examined by indirect ophthalmoscopy. Means, standard deviations (SDs), and ranges were calculated for descriptive purposes. Fisher exact text utilizing a 2-sided p value was performed using GraphPad InStat version 3.10 for Windows, GraphPad Software, San Diego California, USA (www.graphpad.com). The study and data collection conformed to all local laws and were compliant with the principles of the Declaration of Helsinki.
Results
Thirty-two children were diagnosed with ADHD, and 19 children with ADD. The average best-corrected visual acuity of the better-seeing eye was 1 (range 0.9-1.25) and 0.96 (range 0.5-1.25) for the fellow eye. Ten (18%) had amblyopia in one or both eyes (3 had strabismic and 7 had ametropic amblyopia). Forty-five children received methylphenidate (Ritalin, Concerta), while 6 subjects did not receive any medical treatment for ADHD. A vision-related condition was the cause for initial referral in 62% of children, and other reasons were responsible for 16% of the visits (Tab. I), but all children were referred at some point of time to assess vision or orthoptic problems, or any other ocular anomalies. Heterotropia was found in 4 (8%): 3 cases with esotropia and 1 revealed intermittent exotropia. Full stereopsis was detected in the majority of children, 34 (67%), absent stereo acuity was found in 2 (4%), while 17 (33%) patients were unable to perform this test. Subnormal convergence amplitude was noted in 2 patients (4%). The SE cycloplegic refraction of 36 eyes revealed emmetropia, while 25 eyes showed a myopic refractive error and 41 a hyperopic refraction. Twenty-nine eyes of 15 children had astigmatism. Anisometropia was revealed in 17 children. The mean SE of the eyes in this study was 0.17±1.73 (range −5.5 to +7). The mean SE of the myopic eyes in this study was −1.63±1.53 (range −0.25 to −5.5). The mean SE of the hyperopic eyes in this study was 1.48±1.53 (range 0.125-7) (Fig. 1). With-the-rule astigmatism was present in 20 (69%) eyes, against-the-rule astigmatism was prevalent in 7 (24%) eyes, and 2 (7%) of the patients had an oblique axis astigmatic refractive error with astigmatic errors of −0.5, −0.5, and −0.75. Two children presented with an anisometropia greater than 1 D (1.375 and 1.875). Forty eyes (39%) of 29 patients (57%) had significant ametropia in one or both eyes. Myopia of −0.50 D or higher was detected in 17 (17%) eyes of 12 (24%) children. Hyperopia of 2 D or higher was seen in 11 (11%) eyes of 7 (14%) subjects, and astigmatism larger or equal to 1.0 D was observed in 10 (10%) eyes of 7 (14%) patients (Fig. 2). No fundus abnormality was detected in any of the patients.
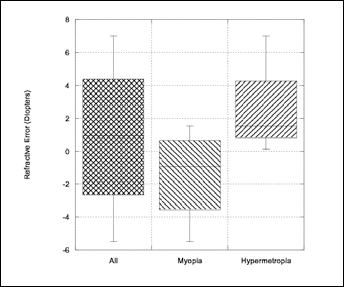
Refractive error characteristics of children in the study.
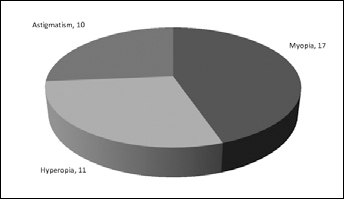
Children with attention deficit hyperactivity disorder with clinically significant refractive errors.
CAUSES FOR REFERRAL FOR EYE EXAMINATION a
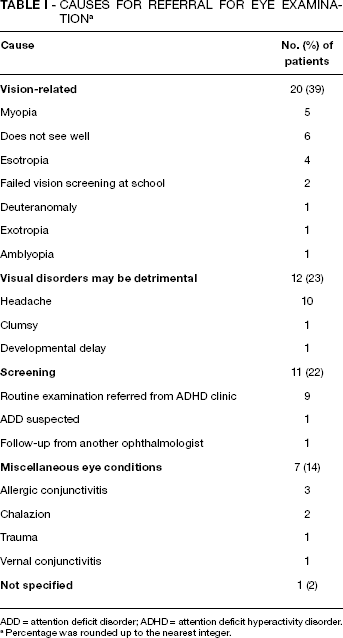
ADD = attention deficit disorder; ADHD = attention deficit hyperactivity disorder.
Percentage was rounded up to the nearest integer.
Discussion
Attention deficit hyperactivity disorder is estimated to reach an incidence of 7.5% by adolescence, and is 4-9 times more prevalent in males compared to females (5). This tendency was also observed in our study population and showed twice as many affected boys than girls. Attention deficit hyperactivity disorder is a heterogenic disorder probably involving several loci. The etiology, although unknown, has been associated with cortical inhibition and malfunction of the frontostriatal pathways, with reduction of blood flow in the domain of the orbitofrontal cortex and structural cortical abnormalities (1, 2). One hypothesis suggests that one locus for therapy may be the superior colliculus, a sensory structure associated with distractibility and production of head and eye movements (3).
Adults with ADHD were reported recently to have saccadic inhibition abnormalities, which could be due to a malfunction of prefrontal cortex–basal ganglia connections (4).
Previous studies demonstrated that ocular functions such as eye motility and fundus morphology reflecting prenatal defects of neural development might be associated with ADHD (5). Other ocular malformations were observed in children with ADHD: they had smaller optic disc areas and a smaller neuroretinal rim compared to controls, which was attributed to a reduction in the number of axons or a reduction in axonal volume of the optic nerve. Furthermore, vascular abnormalities of the fundus were observed, possibly reflecting an early malfunction in the formation of these structures.
A study by Grönlund et al (5) found that 76% of the examinees had ophthalmic findings including reduced visual acuity, strabismus, subnormal stereoacuity, convergence abnormalities, refractive errors, small optic discs, and cognitive visual problems (5). Visual acuity performance in this group greatly improved when treatment included stimulants, although a training effect may also be considered as part of the improvement. Less ametropia, heterotropia, and no ocular structural abnormalities were present in the current study compared to the study of Grönlund et al (Tab. II). Grönlund et al performed a very similar study to the present one with fewer subjects; nevertheless, the ophthalmic abnormalities in their group were much more prevalent than in the present group. Visual acuity was better than 0.8 in 83% of the subjects. In comparison, visual acuity of 1.0 in the better-seeing eye was present in 100% of the patients in our study. They found heterotropia in 29% while we found heterotopias in only 8% of the examinees. In addition, subnormal stereoacuity was found in 26% of their patients, while in ours only 4% did not possess stereoacuity. Twenty-four percent of the patients had convergence abnormalities in the Grönlund et al group, but only in 4% in our group. Significant myopia, hypermetropia, and astigmatism were detected in 19%, 24%, and 24% of their patients, respectively. In contrast, the current study revealed myopia, hypermetropia, and astigmatism in 24%, 14%, and 14%, respectively. Finally, structural abnormalities including smaller optic nerve discs were found in 21% of their patients and decreased vascular tortuosity was documented in 18% of the patients, while in our group these findings were not detected in any of the subjects. The abnormalities in the 2 groups were similar but much less common in our study. This may be because our patients were from a private clinic while theirs were recruited from a tertiary academic center and may reflect the problems in a group of children with more difficult symptoms and a more severe spectrum of ADHD. Both studies suggest that there is a higher rate of ophthalmic abnormalities associated with children with ADHD. Parents of children with ADHD may wish to minimize visits to doctors given the difficulty in examining these patients. If there is no obvious ophthalmic problem, then there is less chance that they will make an appointment to see an ophthalmologist. If there is an obvious issue, such as a heterotropia, then they are much more likely to take their child for an eye examination. This observation might pose a greater selection bias in our study where 20% of the children were examined as part of a routine workup for detection of ADHD, while in the other study all the patients had already been diagnosed with ADHD and hence all of them were routinely seen in the eye clinic. Another cause for the higher rate of retinal abnormalities might be the fact that the fundus findings in Grönlund et al's study were analyzed by a computer digital mapping system rather than ophthalmoscopy, a modality that might have superior sensitivity to detect subtle structural changes. Granet et al (6) reported a much higher incidence of convergence insufficiency in children with ADHD. Patients with convergence insufficiency often present with poor school performance and poor reading skills. They postulated that treatment of the underlying convergence insufficiency could improve the function of children diagnosed with ADHD (6). The near point of convergence was abnormal or absent and improved with stimulants. In our group, we did not find such a large group of children with convergence abnormalities; again, this may reflect the fact that more cases that are difficult are sent to clinics in the hospital. Another study reported better visual acuity and visual field function when children with ADHD were on stimulants. This improvement was not seen in the control group (7). This difference could be attributed to inattentiveness and not to a true visual field defect or reduced visual acuity.
COMPARISON OF OCULAR FUNCTION AND STRUCTURE a
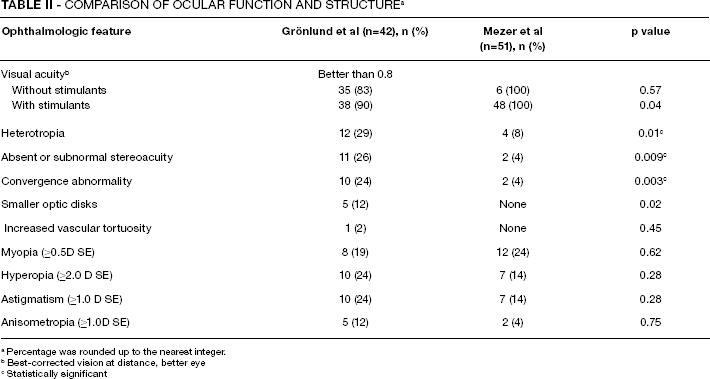
Percentage was rounded up to the nearest integer.
Best-corrected vision at distance, better eye
Statistically significant
In the present study, significant ametropia was detected in 39% of the patients. In contrast to other studies, we did not find a higher rate of convergence insufficiency ametropia or heterotropia. No subtle morphologic changes of the optic nerve and retinal vasculature were detected in the current group, and no other abnormal anatomic ophthalmic findings were observed.
In summary, ametropia was observed in as much as a third of children diagnosed with ADHD in our study although we observed substantially less other ocular abnormalities. Although the range and spectrum of ocular abnormalities varied substantially between our study and other studies, their existence together with other behavioral and neurologic abnormalities can hamper the overall development of children with ADHD or ADD. As ametropia and heterotropia can be readily treated and potentially improve the function of these children, it is advisable to perform an ophthalmic examination as part of routine evaluation.