
Abstract
Purpose
TO determine ocular pulse volume values in patients with thyroid-associated ophthalmopathy with normal intraocular pressure, and to test the hypothesis that changes in orbital tissue that accompany thyroid-associated ophthalmopathy can in turn give changes in choroidal perfusion.
Methods
In a prospective study, we evaluated 30 eyes of 30 consecutive patients with TAO, and 30 eyes of 30 healthy subjects. Complete ophthalmologic examination including dynamic contour tonometry was done. Possible differences in ocular parameters between the tested groups were assessed.
Results
NO significant difference was found in ocular pulse volume values between the tested subjects (paired test p=0.23).
Conclusions
The orbit tissue changes that are involved in thyroid-associated ophthalmopathy do not have much implication on choroidal perfusion, at least when intraocular pressure values remain within the normal range.
Introduction
Intraocular pressure (IOP) elevation in thyroid-associated ophthalmopathy (TAO) can be a consequence of external ocular compression and increased episcleral venous pressure (resulting from the lymphocytic infiltration of the extraocular muscles and resultant proptosis and venous congestion), or restrictive fibrosis of the inferior rectus muscle (which causes mechanical compression in the primary position of gaze) and possible accumulation of mucopolysaccharides in trabeculum (1–3). Data regarding association of TAO with ocular hypertension and secondary open-angle glaucoma vary from 0.8% to 20% of cases (4–7). According to these data, a fair number of patients with TAO will not experience IOP elevation. Whether the changes in their orbital tissue result in consequent changes in choroidal perfusion is yet to be ascertained.
To our knowledge, none of the prior studies have investigated the ocular pulse amplitude (OPA) values in TAO using dynamic contour tonometry (DCT). The aims of this study were 1) to determine OPA values in patients with TAO with normal IOP and 2) to test the hypothesis that changes in orbital tissue which accompany TAO can in turn give changes in choroidal perfusion.
Materials and Methods
In a prospective, comparative study, we evaluated 30 consecutive patients with TAO and 30 healthy subjects, all examined at University Eye Hospital, Medical Faculty of Belgrade, between January 2011 and January 2012. The study was approved by the local ethics committee, and informed consent according to the Declaration of Helsinki was obtained from each tested subject.
The diagnosis of TAO was based on history; the presence of conventional symptoms; elevated levels of serum T3, free T3, T4, and free T4, and increased thyroidal 131J up-take; elevated titers of antithyroid stimulating antibody, antithyroglobulin antibody, and antithyroid peroxidase antibody; or the presence of ophthalmopathy (proptosis, extraocular muscle hypertrophy, orbital congestion, eyelid retraction, and orbital inflammation). Inclusion criteria for the study were consistent with TAO grading according to the NOSPECS classification (8). The diagnosis of TAO was confirmed by an expert oculoplastic specialist.
The control group was matched for age and gender distribution, and they had no history of ophthalmic disorders other than refractive error, dry eye syndrome, conjunctivitis, and eyelid problems.
Exclusion criteria included any ocular disorder precluding fundus examination or tonometry, history of orbital decompression surgery, and glaucoma.
All the TAO patients had been free of local or systemic medication for the treatment of ophthalmopathy (apart of artificial tears). One eye of each control subject and patient with TAO (if condition was bilateral) was randomly selected for the study. If TAO was unilaterally expressed, the affected eye was taken for the study. A complete ophthalmic examination, including applanation tonometry, DCT (Ziemer Ophthalmic System AG, Switzerland), pachymetry (Palm Scan AP 2000, Ophthalmic Ultrasound, 2007, Micro Medical Devices Inc., Calabasas, California, USA), autorefractometry, exophthalmometry (Hertel), color saturation tests, visual field testing (Humphrey Field Analyzer, Carl Zeiss Meditec, Dublin, California, USA, program 30-2), HRT II (HRT II, Heidelberg Retinal Tomography II, Heidelberg Engineering, Heidelberg, Germany) examination, indirect funduscopy (Volk, fundus lens 78 D), and measurement of eye movements, was performed by 2 experienced ophthalmologists (M.B. and M.K.) in all patients.
All patients had a 24-2 full threshold or Swedish interactive threshold algorithm (SITA) automated visual field. Only reliable fields with a fixation loss rate ≤33% and false-positive and false-negative rates ≤20% were included.
Readings were taken in the following order: DCT, Goldmann applanation tonometry (GAT), and pachymetry. After topical anesthesia of the cornea (tetracaine 1.0%), the DCT measurements were taken. The average recording time for all tested subjects was 8.6 seconds. We did not include measurements of unacceptable quality (Q3–Q5).
A slit lamp (Haag-Streit, Switzerland) with a calibrated Goldmann tonometer was used for GAT. Fluorescein sodium 2% strips were also used for the GAT measurements. Three measurements were taken and mean IOP value was recorded. The DCT and GAT were performed with the patient sitting in an upright position at the slit lamp. The DCT was not biased by the GAT as it was the first reading performed. The CCT was determined using ultrasound pachymetry. The pachymeter probe was placed on the center of the cornea (after topical anesthesia of the cornea with tetracaine 1.0%), over an undilated pupil, and the mean of 3 readings within a range of ±5 μm was calculated for each eye.
Systolic and diastolic blood pressure measurements were taken from each patient after 5 minutes of rest. Blood pressure measurements were taken 3 times, with a minimum 5-minute interval between readings (Omron M3 Intellisense, automated manometer, Omron Healthcare, Kyoto, Japan), and the mean blood pressure was noted.
The obtained results were processed by applying the method of descriptive statistics (arithmetical mean, standard deviation) and analytical statistics, for evaluation of statistical significance (χ2 test, Student t test). P less than 0.05 was considered statistically significant.
Results
A total of 30 eyes of 30 patients with TAO (mean age 54.45; range 19–72; 23 women) and 30 eyes of 30 healthy subjects (mean age 55.95; range 21–72; 21 women) in the control group were enrolled in this study. Table I shows the baseline clinical data of the tested groups. No statistically significant differences in age, sex, systolic or diastolic blood pressures, or heart rate were observed between the tested subjects.
- CHARACTERISTICS OF PATIENTS WITH TAO AND CONTROLS
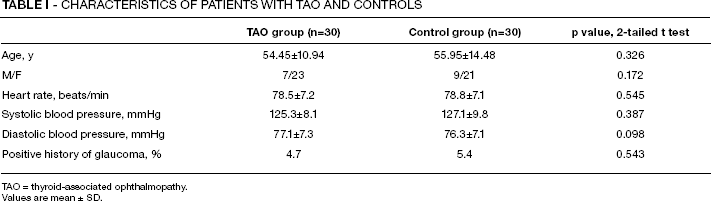
TAO = thyroid-associated ophthalmopathy.
Values are mean ± SD.
Positive history of glaucoma in close relatives was not significantly different in the TAO group (4.7%) and (5.4%) controls.
The results of IOP readings, HRT, and visual field testing were normal in both tested groups. None of the tested subjects were on any antiglaucoma medication. There were no significant differences in IOP measured by GAT and DCT between the tested groups (p=0.1 and 0.2, respectively) or in CCT values (p=0.19).
The mean OPA in the TAO group was 2.38±0.76 mmHg, and 2.21±0.7 mmHg in the control group, with no significant difference (p=0.23).
Measured ocular parameters (IOP, OPA, CCT) for all tested subjects are given in Table III.
None of our patients had central vision decrease or clinically apparent optic neuropathy caused by orbital involvement.
Exophthalmometric values (Hertel) were >20 mm in 76.67% of cases and <20 mm in 73.33% of controls (paired t test, p=0.001). Results are shown in Table II.
- EXOPHTHALMOMETRY IN TESTED SUBJECTS (HERTEL)
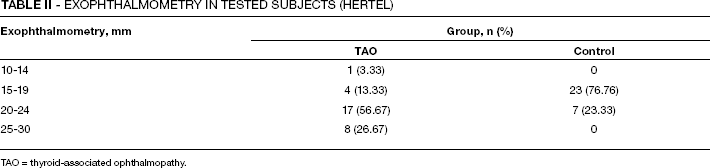
TAO = thyroid-associated ophthalmopathy.
- IOP MEASURED BY GAT AND DCT, OPA, AND CCT IN TESTED SUBJECTS
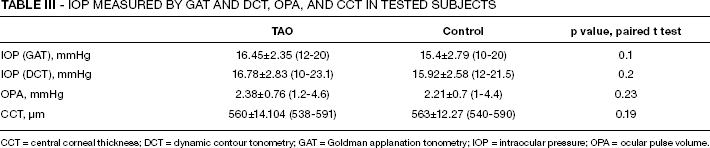
CCT = central corneal thickness; DCT = dynamic contour tonometry; GAT = Goldman applanation tonometry; IOP = intraocular pressure; OPA = ocular pulse volume.
No significant difference was found in OPA values between the tested subjects (paired t test, p=0.23).
Discussion
It is possible that the changes in the orbit associated with TAO are involved in the development of open-angle glaucoma, including normal-tension glaucoma. Wessely in 1918 was the first to describe increased IOP on upgaze in patients with TAO (11). The proposed mechanism of the increased IOP on upgaze was inelasticity of the inferior rectus muscle as a result of fibrosis and consequent incapacity to relax, which causes compression on the globe when the antagonist pulls the eye upwards (12). Later studies revealed other possible mechanisms underlying this complication: increased episcleral venous pressure, changes in trabeculum (1–3).
We focused our study on detecting the possible changes in ocular perfusion in patients with TAO. Previous studies that were addressing this problem were performed on commonly used devices, such as pulsatile ocular blood flow tonometer. Nowadays, the range of technical possibilities of getting an insight on ocular perfusion is widened, and indirectly, DCT is one of them. Besides tonometry values, DCT gives us a value that represents the difference between systolic and diastolic pressure, the OPA (9, 10). This index is thought to be an indirect indicator of the choroidal perfusion that reflects the ocular blood flow corresponding to the heart pulse as a function of time (9). Among glaucomatologists, the common belief is that the optic nerve head vessels represent the most relevant vascular bed for glaucoma pathogenesis (13). When weighing the validity of a parameter such as OPA, we have to bear in mind that its values are affected by the IOP values. The OPA was found to increase with the IOP values in different glaucoma groups, being the highest in ocular hypertension and the lowest in healthy subjects (14). We tested the hypothesis that the occurrences in orbital tissue in TAO can have some consequence on ocular perfusion, and OPA values.
No significant difference in OPA values among patients with TAO and healthy controls was found in our study (paired t test, p=0.23). Several studies concluded that the OPA measurements can potentially be an important milestone in the detection and follow-up of glaucoma, but only when IOP is above the normal values (13). All enrolled subjects in our study had IOP within the normal range, and there was no significant difference in IOP between the tested groups, either when measured with GAT or DCT (paired t test, p=0.1 and p=0.2). Here we have to point out the importance of IOP measurement in TAO in primary, up, and downgaze, as pointed out by Kalmann and Mourits (5). Unfortunately, DCT measurements are practically impossible to take in gaze directions other than primary, so our study lacks data on IOP and OPA values in different gaze directions.
Alimgil et al (15) showed that OPA in patients with TAO with pronounced orbital involvement is significantly lower compared to patients with TAO with no ocular involvement. According to Alimgil et al, reduced OPA could be due to orbital edema and swelling, which can cause a relative decrease of arterial filling facility of the choroid, or the increase of intraorbital pressure may prevent the eye from pulsating mechanically. The results of this study implicated that the measurement of OPA could be a useful parameter for discrimination and classification of orbital involvement in patients with TAO.
Unlike the results of our study, Tsai et al (16) observed a significant decrease in pulse amplitude, pulse volume, and pulsatile ocular blood flow in patients with TAO. The difference in results could partially be due to a different technique used for assessing ocular blood flow, but is more likely a consequence of the fact that there was a significant difference in IOP between the tested groups in 2 studies by Tsai et al. Selected patients with pronounced ophthalmopathy in the Tsai et al study had significantly lower pulse amplitude, pulse volume, and pulse ocular blood flow, but also higher IOP values. Nevertheless, the difference was not noted when they compared patients without ophthalmopathy and healthy controls. This is in agreement with the results of our study, since we could not detect a significant difference between the OPA values in healthy subjects and subjects with TAO who had IOP within the statistically normal range. This can lead us to conclude that drastic disturbances have to take place in the orbit of the patient with TAO to initiate a cascade of changes in ocular perfusion.
Despite the controversial statistics on probability of getting glaucoma associated with TAO obtained so far, and the results of our study, which show no direct changes in OPA values in TAO, we stress the need for carefully monitoring IOP in all patients with TAO.