
Abstract
Purpose.
To compare the biomechanical properties of corneas in eyes of children with diabetes mellitus and in eyes of children without diabetes mellitus.
Methods.
In this prospective, comparative, and cross-sectional study, 46 patients with diabetes mellitus (study group) and 50 healthy individuals (control group) were enrolled. The corneal hysteresis (CH) and corneal resistance factor (CRF) were measured in children with and without diabetes using the Ocular Response Analyzer. Differences in the corneal biomechanical properties were determined using an independent-samples t test. Correlations between ocular and diabetic parameters were also evaluated.
Results.
Mean CH was 12.3±1.3 (SD) mmHg and 12.5±1.5 mmHg and the mean CRF was 12.4±1.7 mmHg and 11.9±1.5 mmHg in the diabetic and control groups, respectively (p>0.05). Corneal hysteresis and CRF were not correlated with fasting glucose level, HbA1c, age, or duration of diabetes.
Conclusions.
The findings indicate that diabetes mellitus does not affect corneal biomechanical parameters such as CH and CRF in children. In addition, CH and CRF are not affected by fasting glucose level, HbA1c, age, or duration of diabetes.
Introduction
Diabetes mellitus is a common disease associated with many ocular complications such as diabetic retinopathy, cataract, glaucoma, eyelid inflammatory disease, and palsy of the oculomotor nerve (1–4). Diabetes mellitus also has significant effects on the corneal epithelium, basement membrane, stroma, and endothelium (5–9). Corneal involvements include superficial punctate keratopathy, recurrent corneal erosion, persistent epithelial defect, and corneal endothelial damage (4).
The hyperglycemic state of patients with diabetes mellitus causes the nonenzymatic glycosylation of proteins, resulting in the formation of advanced glycosylation end products (AGEs). The presence of AGEs in tissue leads to an increase in collagen crosslinkage that results in several harmful reactions (10–12). Neuron-specific enolase (NSE) is a unique form of the glycolytic enzyme enolase, and also has a role in contribution of the neural crest cells to the development of the anterior ocular structures in the rat, similar to that in man (13). Corneal stromal changes include structural alterations produced by collagen cross-linking, which results in increased stiffness of the cornea, as reported in previous in vitro studies (14–16). This condition has been associated with overestimation of the true intraocular pressure (IOP) and the observation that diabetic corneas are less susceptible to the development and progression of keratoconus (17–19).
The alteration in the properties of corneal stroma occurs due to several factors such as aging, ocular pathology, and systemic diseases resulting in altered corneal biomechanical properties. The Ocular Response Analyzer (ORA) (Reichert Ophthalmic Instruments) allows us to perform in vivo evaluation of corneal biomechanical parameters such as corneal hysteresis (CH) and corneal resistance factor (CRF) using a noncontact rapid air pulse. Corneal hysteresis measures the viscous damping of the cornea, and CRF is most associated with the viscous and elastic resistance inherent to the cornea (20, 21). The ORA also allows assessment of IOP, described as Goldmann-correlated IOP (IOPg) and corneal-compensated IOP (IOPcc).
Several previous studies have reported altered corneal biomechanical parameters measured with ORA in older patients with type 2 diabetes mellitus (22–24). However, there have been no reports on corneal biomechanical properties in children with diabetes mellitus. The aim of this study was to evaluate the corneal biomechanical parameters in children with diabetes mellitus without diabetic retinopathy.
Materials and Methods
Study population and design
This prospective and observational study was performed at the Ophthalmology and Pediatric Departments of Istanbul Kanuni Sultan Suleyman Education and Research Hospital. The study followed the tenets of the Declaration of Helsinki and was approved by the local ethics committee. Parents provided written informed consent as the participants were under 18 years of age.
The patients were divided into 2 groups: normal cases (control group) and cases with diabetes mellitus (study group). The study group comprised patients with type 1 diabetes mellitus referred from the Department of Pediatrics. The age-matched control group comprised healthy children examined at the Department of Pediatrics and in whom diabetes mellitus or abnormal glucose levels were excluded.
The exclusion criteria included the following: a best-corrected visual acuity worse than 20/20, glaucomatous optic disc changes such as excavation, notching, or focal thinning of the neuroretinal rim, and peripapillary hemorrhage, glaucomatous visual field defects, IOP readings greater than 22 mmHg, a history of ocular trauma or ocular surgery, and a history of systemic disease except diabetes mellitus.
Examination protocol and measurements
Each clinical examination consisted of best-corrected visual acuity using a Snellen chart, IOP measurement using the Goldmann applanation tonometer, biomicroscopy of the anterior segment, dilated fundus examination, central corneal thickness (CCT) measurement with ultrasound pachymetry, and axial length (AL) measurements with the IOL Master (Carl Zeiss Meditech, AG, Jena, Germany).
The corneal biomechanical parameters were measured using Reichert Ocular Response Analyzer Software 3.01 by an experienced clinician while the patient was sitting comfortably in a chair located in a special room. Four good-quality measurements with minimal variability were obtained for each eye and the mean values of each parameter were used for statistical analysis. The clinician was masked in terms of study group.
Data analyses
All statistical tests were performed using SPSS (Statistical Package for the Social Sciences; SPSS Inc., Chicago, IL, USA) version 16. The normality of the data was confirmed using the Kolmogorov-Smirnov test (p>0.05). Independent Student t test was used to compare variables between groups. Pearson correlation was used to examine the relationships among the measured variables. A p value of <0.05 was considered significant.
Results
Demographic findings
This study included 50 healthy children and 46 children with diabetes mellitus. The characteristics of the 2 groups of subjects are shown in Table I. There were no statistically significant differences between the 2 groups with regard to age and gender distributions.
Demographic and Clinical Characteristics
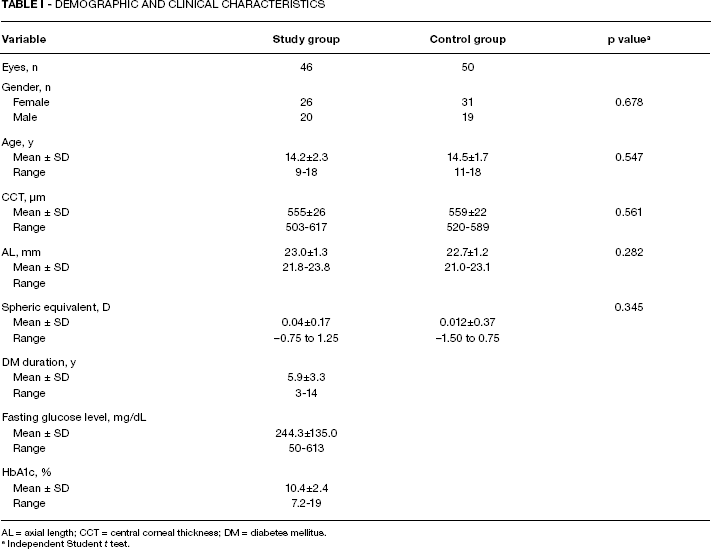
AL = axial length; CCT = central corneal thickness; DM = diabetes mellitus.
Independent Student t test.
Biomechanical parameters (CH and CRF)
Table II summarizes the comparison of mean ORA measurements in study and control groups. Mean CH and CRF values in eyes with diabetes were not significantly different from those in age-matched controls. The IOPg and IOPcc, which were measured with ORA, did not differ between the study and control groups.
Comparison of Mean ORA Measurements in Study and Control Groups
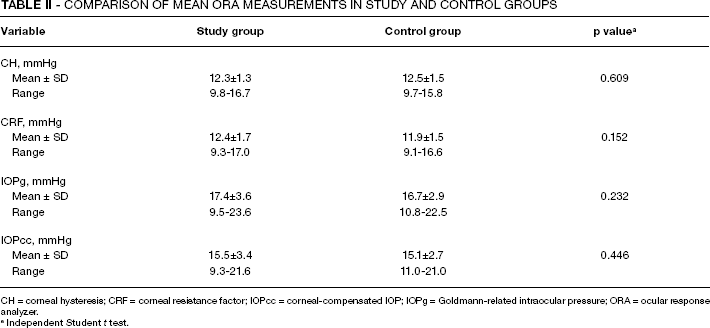
CH = corneal hysteresis; CRF = corneal resistance factor; IOPcc = corneal-compensated IOP; IOPg = Goldmann-related intraocular pressure; ORA = ocular response analyzer.
Independent Student t test.
The mean duration of diabetes was 5.9±3.3 years (range 3–14) and the mean current HbA1c was 10.4±2.4 (range 7.2–19) (Tab. I). A correlation analysis was performed between current fasting glucose level, HbA1c, age, duration of disease, and CH-CRF values in the study group. The CH value was not associated with current fasting glucose level (r=-0.010, p=0.942), HbA1c (r=0.256, p=0.294), age (r=-0.267, p=0.205), or duration of disease (r=0.121, p=0.504). The CRF value was not associated with current fasting glucose level (r=0.178, p=0.465), HbA1c (r=0.392, p=0.219), age (r=-0.251, p=0.314), or duration of disease (r=0.461, p=0.092). The CCT was also not associated with current fasting glucose level (r=0.239, p=0.454), HbA1c (r=0.039, p=0.904), age (r=-0.397, p=0.201), or duration of disease (r=0.125, p=0.654).
Discussion
The corneal stroma is responsible for its mechanical and refractive properties (25). The changes in the properties of corneal stroma due to advancing age, corneal pathologies such as keratoconus, and systemic disease such as diabetes mellitus result in altered corneal biomechanical properties.
Diabetes mellitus has a significant effect on corneal stroma (26). Hyperglycemia causes the increased protein glycosylation, lysyl oxidase enzymatic activity, and the production of AGEs (27, 28). The production and accumulation of AGEs has been associated with increased collagen cross-linking in the corneas of diabetic patients. Higher CCT values have also been indicated in diabetic eyes compared with healthy control (29, 30). Both increased thickness of the cornea without edema and crosslinking of collagen fibers may eventually result in altered corneal biomechanical properties (16).
Several previous studies have investigated the corneal biomechanical properties in adult individuals with diabetes mellitus (22–24). Kotecha et al reported that eyes of diabetic patients indicated significantly higher CRF than eyes of nondiabetic patients (22). They also found that eyes of type 1 diabetes patients have significantly higher CH than eyes of type 2 diabetic patients and eyes of nondiabetic subjects. Goldich et al showed that the CCT, CH, and CRF of diabetic eyes were significantly higher than those of nondiabetic eyes (23). In contrast to both Kotecha and Goldich, Sahin et al determined that CH was significantly lower in diabetic patients, whereas CRF was not significantly different from that of control subjects (24). As mentioned above there have been controversial studies published on corneal biomechanical changes in adult diabetic patients; however, there have been no studies of corneal biomechanical parameters in children with diabetes. In our study, we investigated the corneal biomechanical parameters such as CH and CRF in diabetic children without diabetic retinopathy. Our data suggest that no differences exist in corneal biomechanical properties between diabetic and nondiabetic children. We also found that CRF and CH values were not associated with fasting glucose level, HbA1c, age, or duration of diabetes.
The literature contains fewer studies on the effects of diabetes on corneas in children than adults. Gestational diabetes has been shown to play an inhibitory role in the migration of the neural crest cells of the corneal endothelium, but diabetes mellitus itself does not affect the endothelial cell count in the pediatric population (31). Akinci et al reported that diabetic children have a significantly increased central corneal thickness compared with healthy controls (30). Moreover, they demonstrated that the HbA1C level was the only disease-related parameter that has an influence on central corneal thickness.
In contrast to previous studies that indicate altered corneal biomechanical parameters in eyes of diabetic adults, we found a lack of differences in corneal biomechanical parameters between the eyes of children with and without diabetes in our study. This may be explained in several ways. First, the mean duration of diabetes, 5.9 years in our study, might lead to these results. Because our study participants were under 18 years old, disease duration was low. Although Sahin et al (24) reported that disease duration (mean 13.5 years) had a statistically significant effect on CH and CRF, larger cohort studies are required to investigate the role of disease duration on corneal biomechanical properties. Secondly, the age of our participants (mean 14 years) might lead to these results. In the previous studies that reported altered corneal biomechanical parameters, the mean age of patients was over 50 years (22–24). It has been shown that an increased presence of AGEs in the cornea with advancing age results in altered corneal biomechanical properties (28, 32). Third, several studies found a positive significant correlation between the CCT and corneal biomechanical parameters (25, 33–35). Studies have also determined a positive significant association between the CCT and corneal biomechanical parameters in diabetic eyes (22, 24). In our study, we did not find any statistically significant differences between the children with and without diabetes.
In conclusion, the present study showed that the corneal biomechanical parameters of diabetic children such as CH and CRF are similar to those of healthy controls. Current fasting glucose level, HbA1c, duration of diabetes, and age do not seem to be associated with CH and CRF in children with diabetes. Further studies are required to establish the effects of diabetic disease severity and long-term poor glucose control on corneal biomechanical properties.