
Abstract
Purpose
To identify complications associated with tumor-related lipid exudation (TRLE) after plaque radiotherapy of posterior uveal melanoma.
Methods
Comparative study including 294 patients with posterior uveal melanoma who developed TRLE after plaque radiotherapy (TRLE group) and 294 patients who did not develop TRLE (non-TRLE group). Patients in the TRLE group were matched with patients in the non-TRLE group for age, gender, and initial tumor thickness.
Results
The TRLE group was associated with significantly higher incidence of postradiation complications including early transient increase of serous retinal detachment (p<0.001), iris neovascularization (NVI) (p<0.001), neovascular glaucoma (NVG) (p<0.001), posterior synechia (p<0.001), vitreous hemorrhage (p<0.001), subretinal hemorrhage (p<0.001), and retinoschisis (p<0.001). A significant relationship was found between extent of TRLE and NVI (p<0.001), NVG (p<0.001), posterior synechia (p = 0.007), and retinoschisis over tumor (p = 0.010). Radiation-induced retinopathy, maculopathy, and papillopathy were not associated with presence or extent of TRLE. Tumor-related lipid exudation was also associated with worse final visual acuity (p = 0.011), higher rate of secondary enucleation (p<0.001), and lower rate of systemic metastasis (p = 0.006).
Conclusions
Tumor-related lipid exudation following plaque radiotherapy of posterior uveal melanoma is associated with major intraocular complications and portends poor prognosis for final visual acuity and eye retention. These findings provide evidence for the presence of 2 distinct pathogenic mechanisms, one radiation-induced and one tumor-related, in development of postradiation complications in eyes with posterior uveal melanoma.
Introduction
Radiation is a commonly used eye-conserving method for treatment of posterior uveal melanoma and is associated with various postradiation complications (1–15). Tumor-related lipid exudation (TRLE) is a known complication of radiotherapy of posterior uveal melanoma (11, 15). In a prior report, we described the risk factors predisposing to the development of TRLE following plaque radiotherapy of posterior uveal melanoma (15). In the current report, we describe the long-term complications associated with TRLE. We discuss the implications of our findings in regard to the pathogenic mechanisms underlying development of intraocular complications following radiotherapy of posterior uveal melanoma.
Materials and Methods
In this matched study, patients with posterior uveal melanoma who had developed TRLE after plaque radiotherapy (TRLE group) were compared with patients who had not developed TRLE after plaque radiotherapy (non-TRLE group). All included patients were managed at the Oncology Service, Wills Eye Institute, between 1978 and 2007 (Figs. 1, A and B, and 2, A, B, and D). The planned radiation dose to tumor apex was 8000 cGy in all cases. Eyes with serous retinal detachment (RD) without visible lipid exudation and eyes with lipid exudation that, on the basis of clinical or fluorescein angiographic findings, originated from abnormal retinal or optic disc vessels (radiation-induced retinopathy/maculopathy or papillopathy, respectively), and not from the treated melanoma, were excluded from the study. Patients in the 2 groups were matched for age (within 5 years), gender, and tumor thickness (within 1 millimeter). This report compares the TRLE group with the non-TRLE group for development of postradiation complications and is based on analysis of data from the same group of patients included in a previously published case-control study from our center focusing on risk factors predisposing to development of TRLE (15). Further details on the methods can be found in that publication (15). This study has been approved by the institutional review board of Wills Eye Institute.
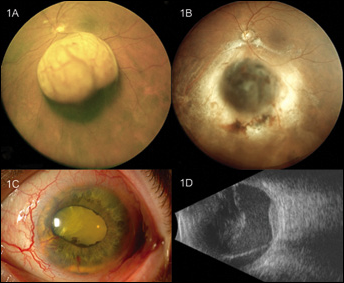
(A) Mushroom-shaped choroidal melanoma 8.6 mm in thickness in the left eye of a 60-year-old man complaining of decreased vision for 2 months prior to presentation; visual acuity is 20/40. (B) Seventeen months after I-125 plaque radiotherapy, the tumor has a regressed appearance with mild subretinal hemorrhage over and anterior to the tumor. Note the lipid exudation at the posterior margin, and to a lesser degree, at the temporal margin of the tumor outside the wide rim of radiation-induced chorioretinal atrophy. (C) Five and a half years after plaque radiotherapy, there is extensive neovascularization of the iris and the patient has developed mature cortical cataract precluding any view of the fundus. Visual acuity is no light perception. (D) B-scan ultrasound 5½ years after plaque radiotherapy reveals regressed tumor, diffuse vitreous echodensities, and linear echodensity inferiorly, consistent with retinal detachment.
Statistical methods
The number and percentage of patients with associated postradiation complications were compared between TRLE and non-TRLE groups using Cox regression analysis. The proportions of patients with these postradiation complications relative to extent of TRLE (≤1 quadrant, 2 quadrants, and ≥3 quadrants) were compared using log-rank test. The interval between plaque radiotherapy and various complications were compared between groups using Wilcoxon rank-sum test. The frequencies of complications based on the presence of Bruch membrane rupture by TRLE and non-TRLE groups were compared using log-rank test. In the TRLE group, the factors predictive of associated complications and enucleation were identified using Cox proportional hazard model. The factors found significant on univariable analysis at 5% level of significance were considered for multivariable analysis using the forward stepwise method. Kaplan-Meier analysis was performed to estimate the cumulative probability of outcome—TRLE, iris neovascularization (NVI), neovascular glaucoma (NVG), macular edema, vitreous hemorrhage, and enucleation—at 2, 5, 10, and 15 years.
Results
The demographic, ocular, and tumor features of the TRLE and the non-TRLE groups have been described previously (15). Overall, 294 patients in each group were analyzed for associated complications. The TRLE patients were first seen at the Oncology Service between March 1978 and July 2007 and non-TRLE patients between October 1979 and April 2006. The median patient age was 56 years (mean 55 years, range 15–83 years) in the TRLE group and 58 years (mean 58 years, range 26–92 years) in the non-TRLE group. The median tumor base and thickness were 12 mm (mean 11 mm, range 1–20 mm) and 6.4 mm (mean 6.4 mm, range 1.9–12.3 mm) in the TRLE group, respectively. In the non-TRLE group, the median tumor base was 12 mm (mean 12 mm, range 5–19 mm) and median tumor thickness was 6.3 mm (mean 6.4 mm, range 2.1–12 mm). The radioactive isotopes used in the TRLE group included iodine-125 (78%), cobalt-60 (17%), iridium-192 (4%), and ruthenium-106 (1%). In the non-TRLE group, the most commonly used isotope was iodine-125 (90%), followed by cobalt-60 (7%), iridium-192 (2%), and ruthenium-106 (1%). The median radiation dose to tumor base was 33,500 cGy (range 12,500–59,600 cGy) in the TRLE group and 30,600 (11,600–81,500 cGy) in the non-TRLE group. The duration of follow-up after plaque radiotherapy was a median of 64 months (mean 80 months) in the TRLE group and a median of 58 months (mean 71 months) in the non-TRLE group.
As shown in Table I, the TRLE group was associated with statistically significant higher frequency of certain postradiation complications including early transient increase of serous RD, NVI (Figs. 1C and 2C), NVG, posterior synechia (Figs. 1C and 2C), vitreous hemorrhage (Fig. 1D), subretinal hemorrhage over tumor (Figs. 1B and 2B), and retinoschisis over tumor (Fig. 2B). Our results also showed a significant relationship between extent of TRLE and these same complications except subretinal and vitreous hemorrhage (Tab. II). The TRLE group also had worse final visual acuity (≤20/200), higher rates of tumor recurrence and secondary enucleation (Fig. 2D), and lower rate of distant metastasis (Tab. I). As seen in Table III, there was no statistically significant difference between the TRLE and non-TRLE groups in regard to the interval between application of radioactive plaque and onset of complications. Table IV shows that, both in the TRLE and the non-TRLE groups, eyes containing posterior uveal melanomas with Bruch membrane rupture were associated with a significantly higher rate of postradiation complications including NVI, NVG, posterior synechia, cataract, vitreous hemorrhage, subretinal hemorrhage over tumor, and retinoschisis over tumor.
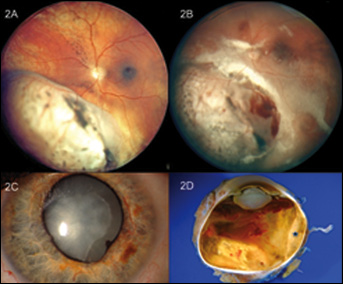
(A) Amelanotic choroidal melanoma with a thickness of 9.6 mm in the left eye of a 27-year-old man with visual acuity of 20/40 4 months after I-125 plaque radiotherapy; note focal retinoschisis over the apex of the tumor. (B) There is extensive tumor-related lipid exudation 19 months after plaque radiotherapy and visual acuity has decreased to 20/400; note persistent retinoschisis with overlying hemorrhage. (C) Thirty-three months after plaque radiotherapy, there is extensive iris neovascularization, focal posterior synechia, and mature cataract. Visual acuity is light perception and intraocular pressure is 35 mm Hg. (D) Over the ensuing 7 months, vision drops to no light perception, intraocular pressure increases to 56 mm Hg, and the eye undergoes enucleation. The gross cut section of the globe shows mature cataract, vitreous hemorrhage, shallow retinal detachment, regressed amelanotic melanoma (asterisk), and extensive lipid exudation (histopathology picture courtesy of Ralph C. Eagle, Jr., MD).
- TUMOR-RELATED LIPID EXUDATION FOLLOWING PLAQUE RADIOTHERAPY OF POSTERIOR UVEAL MELANOMA: ASSOCIATED POSTRADIATION COMPLICATIONS
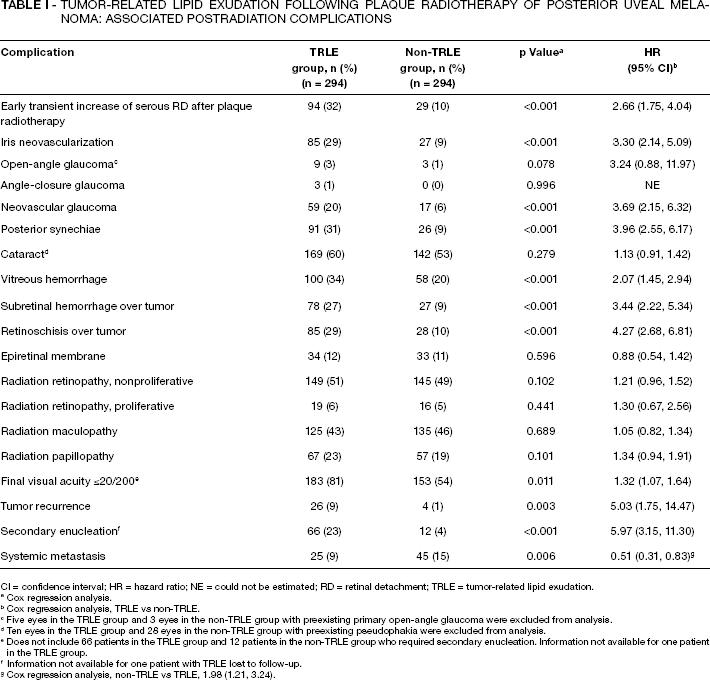
CI = confidence interval; HR = hazard ratio; NE = could not be estimated; RD = retinal detachment; TRLE = tumor-related lipid exudation.
Cox regression analysis.
Cox regression analysis, TRLE vs non-TRLE.
Five eyes in the TRLE group and 3 eyes in the non-TRLE group with preexisting primary open-angle glaucoma were excluded from analysis.
Ten eyes in the TRLE group and 28 eyes in the non-TRLE group with preexisting pseudophakia were excluded from analysis.
Does not include 66 patients in the TRLE group and 12 patients in the non-TRLE group who required secondary enucleation. Information not available for one patient in the TRLE group.
Information not available for one patient with TRLE lost to follow-up.
Cox regression analysis, non-TRLE vs TRLE, 1.98 (1.21, 3.24).
- TUMOR-RELATED LIPID EXUDATION FOLLOWING PLAQUE RADIOTHERAPY OF POSTERIOR UVEAL MELANOMA: FREQUENCY OF POSTRADIATION COMPLICATIONS RELATIVE TO EXTENT OF TUMOR-RELATED LIPID EXUDATION (IN THE TRLE GROUP) a
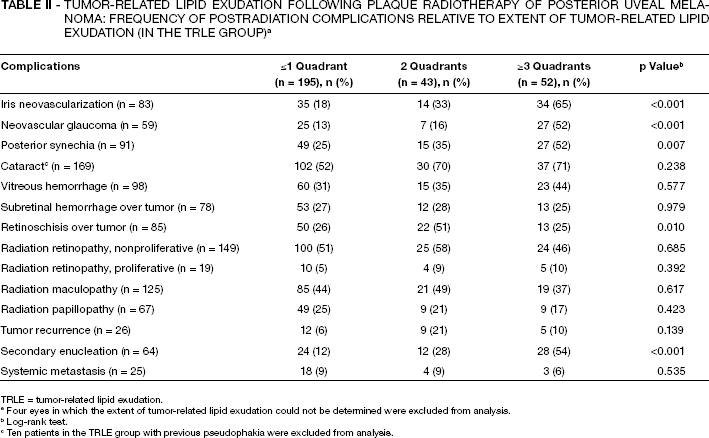
TRLE = tumor-related lipid exudation.
Four eyes in which the extent of tumor-related lipid exudation could not be determined were excluded from analysis.
Log-rank test.
Ten patients in the TRLE group with previous pseudophakia were excluded from analysis.
- TUMOR-RELATED LIPID EXUDATION FOLLOWING PLAQUE RADIOTHERAPY OF POSTERIOR UVEAL MELANOMA: INTERVAL BETWEEN APPLICATION OF RADIOACTIVE PLAQUE AND ONSET OF COMPLICATIONS
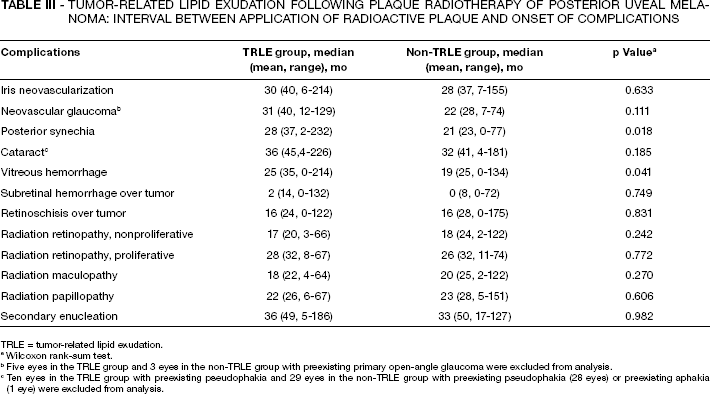
TRLE = tumor-related lipid exudation.
Wilcoxon rank-sum test.
Five eyes in the TRLE group and 3 eyes in the non-TRLE group with preexisting primary open-angle glaucoma were excluded from analysis.
Ten eyes in the TRLE group with preexisting pseudophakia and 29 eyes in the non-TRLE group with preexisting pseudophakia (28 eyes) or preexisting aphakia (1 eye) were excluded from analysis.
- TUMOR-RELATED LIPID EXUDATION FOLLOWING PLAQUE RADIOTHERAPY OF POSTERIOR UVEAL MELANOMA: FREQUENCY OF COMPLICATIONS BASED ON THE PRESENCE OF BRUCH MEMBRANE RUPTURE IN THE TRLE AND NON-TRLE GROUPS

TRLE = tumor-related lipid exudation.
Log-rank test.
Five eyes in the TRLE group and 3 eyes in the non-TRLE group with preexisting primary open-angle glaucoma were excluded from analysis.
Ten eyes in the TRLE group with preexisting pseudophakia and 29 eyes in the non-TRLE group with preexisting pseudophakia (28 eyes) or preexisting aphakia (1 eye) were excluded from analysis.
Information not available for one patient in the TRLE group lost to follow-up.
Results of multivariate analysis for preradiation tumor features predictive of development of postradiation complications in the TRLE group are shown in Table V. The NVI was related to greater tumor thickness, retinal invasion by tumor, and greater extent of TRLE. Features predictive of NVG were greater tumor thickness, mushroom tumor shape, and greater extent of TRLE. Lesser tumor distance to optic disc and presence of retinal invasion by tumor were predictive of development of vitreous hemorrhage. Features predictive of secondary enucleation included greater tumor thickness, retinal invasion by tumor, and greater extent of TRLE (Tab. V). Table VI shows the cumulative incidence of TRLE and its associated complications in the TRLE group at 2, 5, 10, and 15 years after plaque radiotherapy.
- TUMOR-RELATED LIPID EXUDATION FOLLOWING PLAQUE RADIOTHERAPY OF POSTERIOR UVEAL MELANOMA: FEATURES PREDICTIVE OF ASSOCIATED COMPLICATIONS AND ENUCLEATION (IN THE TRLE GROUP)
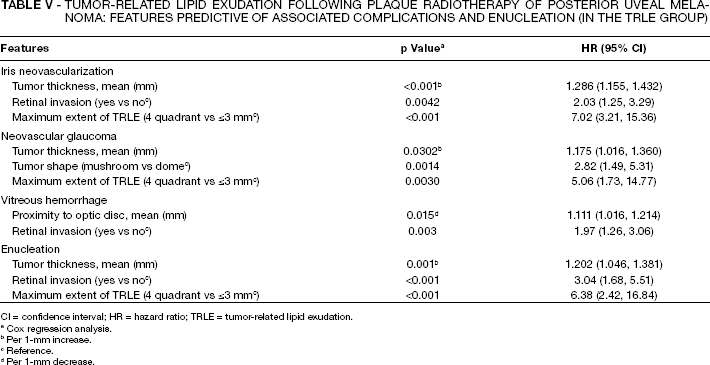
CI = confidence interval; HR = hazard ratio; TRLE = tumor-related lipid exudation.
Cox regression analysis.
Per 1-mm increase.
Reference.
Per 1-mm decrease.
- TUMOR-RELATED LIPID EXUDATION FOLLOWING PLAQUE RADIOTHERAPY OF POSTERIOR UVEAL MELANOMA: CUMULATIVE INCIDENCE OF OUTCOMES USING KAPLAN-MEIER ESTIMATES (IN THE TRLE GROUP)
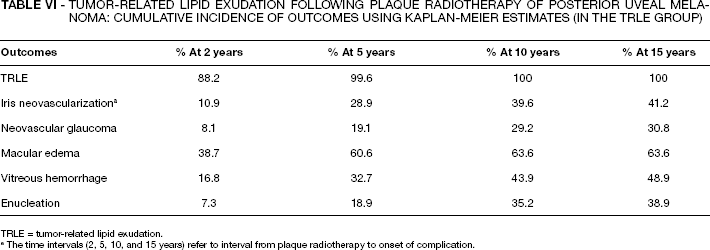
TRLE = tumor-related lipid exudation.
The time intervals (2, 5, 10, and 15 years) refer to interval from plaque radiotherapy to onset of complication.
Discussion
Previous studies have shown residual postradiation tumor tissue to be the source of lipid exudation following plaque radiotherapy of posterior uveal melanoma (11, 15). This condition, referred to as postradiation TRLE, is strongly related to tumor features such as presence of Bruch membrane rupture (15), larger tumor size (11, 15), and lack of application of transpupillary thermotherapy to the tumor (15). The current study, in turn, shows a strong association between presence (Tab. I) and extent (Tab. II) of TRLE and development of certain postradiation complications (NVI, NVG, posterior synechia, vitreous hemorrhage, subretinal hemorrhage over tumor, and retinoschisis over tumor) in eyes with posterior uveal melanoma. We argue that the association between TRLE (itself a tumor-related complication originating from the residual irradiated tumor) and these other postradiation complications provides strong evidence for the role of tumor-related factors in the pathogenesis of some of the important intraocular complications encountered after plaque radiotherapy of posterior uveal melanoma.
Two other findings of our study lend support to the above conclusion. First, as seen in Table IV, the postradiation complications associated with TRLE were more common in eyes containing posterior uveal melanomas with Bruch membrane rupture (a tumor-related feature) compared to those without Bruch membrane rupture. Second, on multivariate analysis, postradiation complications associated with TRLE were mostly predicted by preradiation tumor features, and not by radiation parameters (Tab. V).
Other researchers have shown similar relationships between tumor features and certain postradiation complications in eyes harboring posterior uveal melanoma. Namely, NVG has been related to greater tumor thickness (3, 10, 16, 17), largest tumor basal diameter (6), and increased internal tumor vascularity (10). Cataract has been associated with greater tumor size (6, 7, 17–20) and vitreous hemorrhage with greater tumor size (6, 7) and with Bruch membrane rupture (7, 17). Intraocular inflammation after proton beam radiation has been shown to correlate with initial tumor height (9).
Other arguments have been used by several other investigators to support a possible role for tumor-related factors in development of some postradiation complications. One such argument used by Detorakis et al (10) and Kim et al (21) has been based on the observed relationship between NVG and tumor features such as larger tumor size (height) (10, 21) and greater tumor vascularity (10). A different but related argument by Desjardins and coworkers (22) has been based on their finding that reduction in tumor thickness induced by transpupillary thermotherapy is associated with a decrease in the incidence, severity, and duration of postradiation glaucoma following proton beam radiotherapy of large uveal melanoma. A third line of reasoning has emphasized the observation that even low doses of helium ion radiation (50 GyE) are associated with posterior pole complications outside the radiation field in eyes with thick peripheral melanomas (16, 23). Finally, presence of retinal/optic disc neovascularization (24–26), intraocular inflammation (27), NVI/NVG (28), cystoid macular edema (24), and other photographic and angiographic posterior pole abnormalities (14) in eyes with unradiated uveal melanomas have been ascribed to the effects of the intraocular tumor. Damato (29) has attributed development of exudative RD and NVG after radiation of uveal melanoma to the residual irradiated tumor and has reported regression of these complications following transscleral local resection of the irradiated tumor.
We previously suggested (15) that postradiation vascular changes in the residual necrotic melanoma (30–35) and possibly in the surrounding choroid or retina may play a role in development of tumor-related lipid exudation following plaque radiotherapy of choroidal melanoma. A similar pathogenic mechanism, augmented by postradiation tumor necrosis and resultant inflammation (9), may account for the high incidence of postradiation complications in eyes with TRLE, as seen in the current study. These postradiation vascular changes are important from 2 perspectives. First, vascular changes in the residual necrotic tumor (or the surrounding choroid and retina) can be the direct source of subretinal or vitreous hemorrhage in eyes with irradiated posterior uveal melanoma (6, 7, 17, 36). The higher incidence of subretinal and vitreous hemorrhage in eyes with TRLE (Tab. I) can be, at least partially, explained by the high rate of Bruch membrane rupture in these eyes (15), allowing the extravasated blood in the irradiated residual tumor to extend into the subretinal and vitreous spaces. Second, the radiation-induced vascular alterations in the residual tumor tissue (or the surrounding choroid and retina) may contribute to the elevated levels of vascular endothelial growth factor (VEGF) in eyes with irradiated uveal melanoma, as shown by Missotten and coworkers (37). Vascular endothelial growth factor may, in turn, underlie development of NVI and NVG after radiotherapy of uveal melanoma, a conclusion that is supported by reports of successful treatment of this condition with anti-VEGF agents (38, 39).
The lack of association between TRLE and radiation retinopathy (nonproliferative and proliferative), maculopathy, and papillopathy in our study is noteworthy and confirms that these complications are not tumor-related and result from direct radiation damage to the retinal and optic disc microvasculature, as already believed (14, 40–43). Supporting this distinction between postradiation tumor-related complications and direct radiation-induced side effects, we did not find any relationship between diabetes mellitus and development of TRLE or its associated complications (15). In contrast, radiation maculopathy, papillopathy, and retinopathy have been shown to be more common or severe in patients (1, 8, 14, 43–47) and experimental animals (41) with diabetes mellitus.
The results of this study suggest that 2 distinct pathogenic mechanisms are responsible for development of postradiation intraocular complications in eyes with posterior uveal melanoma. One mechanism is direct radiation damage to nontumoral intraocular tissues and is responsible for radiation-induced retinopathy/maculopathy (40) and papillopathy (direct radiation-induced complications). These complications, as expected, are associated with greater radiation dose to the macula (1, 43, 48, 49) and optic disc (2, 8, 43, 50, 51) or tumor proximity to the fovea (6, 8, 17, 52) or optic disc (6, 7, 48, 51), higher radiation dose per fraction (45, 53) or higher radiation dose rate (7, 8), and host factors such as younger age (51, 52), diabetes (1, 8, 14, 41, 43–47), and systemic chemotherapy (45, 54). The other pathogenic mechanism results from radiation-induced changes in the irradiated residual tumor tissue and, as shown in our study, is strongly associated with tumor features such as size (11, 15), and Bruch membrane rupture (15). Tumor-related complications can manifest locally in the vicinity of the treated tumor (tumor-related lipid exudation, overlying retinoschisis, subretinal hemorrhage, vitreous hemorrhage) or can affect distant intraocular tissues through the action of chemical mediators such as VEGF (37) (posterior synechia, NVI/NVG, and possibly some cases of macular edema and cataract).
The main limitations of this study arise from its retrospective and nonrandomized nature. Practical limitations prevented us from matching the TRLE and non-TRLE groups for more than a few features and it is possible that some known or unknown differences between these 2 groups may be partly responsible for the observed outcomes. Moreover, despite our attempts to exclude such cases, it is possible that the lipid exudation seen in some of the eyes included in the study actually arose from radiation-damaged microvasculature of the optic disc or retina and not from the irradiated tumor itself.
In conclusion, our study revealed a strong association between TRLE after plaque radiotherapy for posterior uveal melanoma and certain postradiation ocular complications including early and transient increase of serous RD, NVI/NVG, posterior synechia, subretinal/vitreous hemorrhage, and retinoschisis over tumor. Eyes with postradiation TRLE, especially if extensive, had a poor visual outcome and were more likely to require secondary enucleation. In contrast, TRLE was not associated with proliferative and nonproliferative radiation retinopathy, maculopathy, or papillopathy. These findings strongly suggest that 2 distinct pathogenic mechanisms, one resulting from direct radiation damage to nontumoral intraocular tissues and the other originating in the irradiated residual tumor tissue, act separately or in concert to produce the postradiation complications encountered in eyes with posterior uveal melanoma. It logically follows that different approaches, depending on the underlying pathogenic mechanisms, are required to prevent development of these vision- or eye-threatening complications. Prevention of direct radiation-induced complications can be achieved by decreasing radiation dose to the macula and optic disc (23, 50, 55–58), by hyperfractionation (59), or by increasing tissue resistance to the damaging effects of ionizing radiation (60). Prevention or treatment of tumor-related complications, on the other hand, can be achieved by surgical (61–64) or laser (21, 29, 61) techniques aimed at removal or destruction of the irradiated residual tumor tissue or by pharmacologic methods directed against chemical mediators released from the irradiated tumor (38, 39, 65). Future research should be conducted to identify these chemical mediators and to elucidate the pathogenic pathways involved in their deleterious effects on intraocular tissues.
Footnotes
ACKNOWLEDGMENT
Arman Mashayekhi, MD, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Rishita Nutheti, PhD, Hyderabad, India, provided statistical analysis.
Support provided by a donation from Michael, Bruce, and Ellen Ratner, New York, NY (J.A.S., C.L.S.), the Paul Kayser International Award of Merit in Retina Research, Houston, TX (J.A.S.), Mellon Charitable Giving from the Martha W. Rogers Charitable Trust, Philadelphia, PA (C.L.S.), the Eye Tumor Research Foundation, Philadelphia, PA (C.L.S., J.A.S.), and the Scientific and Technical Research Council of the Turkish Republic, Tubitak, Ankara, Turkey (S.T.).