
Abstract
Purpose
To compare retinal nerve fiber layer thickness (RNFLT) of normotensive eyes with exfoliation syndrome (XFS) and healthy eyes.
Methods
Sixty-four consecutive individuals with XFS and normal office-time intraocular pressure (IOP) and 72 consecutive healthy controls were prospectively enrolled for a cross-sectional analysis in this hospital-based observational study. The GDx-VCC parameters (temporal-superior-nasal-inferior-temporal [TSNIT] average, superior average, inferior average, TSNIT standard deviation (SD), and nerve fiber indicator [NFI]) were compared between groups. Correlation between various clinical parameters and RNFLT parameters was investigated with Spearman coefficient.
Results
The NFI, although within normal limits for both groups, was significantly greater in the XFS group compared to controls: the respective median and interquartile range (IQR) values were 25.1 (22.0–29.0) vs 15.0 (12.0–20.0), p<0.001. In the XFS group, all RNFLT values were significantly lower compared to controls (p<0.001). However, they were all within the normal clinical ranges for both groups: TSNIT average median (IQR): 52.8 (49.7–55.7) vs 56.0 (53.0–59.3) μm; superior average mean (SD): 62.3 (6.7) vs 68.8 (8.2) μm; inferior average mean (SD): 58.0 (7.2) vs 64.8 (7.7) μm, respectively. TSNIT SD was significantly lower in the XFS group, median (IQR): 18.1 (15.4–20.4) vs 21.0 (18.4–23.8), p<0.001. There was no systematic relationship between RNFLT and visual acuity, cup-to-disc ratio, IOP, central corneal thickness, Humphrey mean deviation, and pattern standard deviation in either group.
Conclusions
Compared to control eyes, polarimetry-determined RNFLT was lower in XFS eyes with normal IOP. Therefore, close monitoring of RNFLT may facilitate early identification of those XFS eyes that convert to exfoliative glaucoma.
Keywords
Introduction
Exfoliation syndrome (XFS) is an age-related condition characterized by the gradual synthesis and accumulation of a fibrillar extracellular material in many ocular and extraocular tissues (1, 2). It is the most common identifiable cause of open-angle glaucoma worldwide, comprising the majority of glaucoma cases in several countries (3). Exfoliation syndrome and exfoliative glaucoma (XFG) currently affect 60–70 million people worldwide (1, 3). Eyes with XFS demonstrate more often increased intraocular pressure (IOP), greater IOP fluctuation, structural alterations of the optic nerve head, and a clinically significant cumulative risk of conversion to XFG (3–8). The cumulative risk of XFG in eyes with XFS and normal IOP is estimated to be approximately 30% in 10 years (9). It is well documented that the clinical course and prognosis of XFG is significantly worse than that of primary open-angle glaucoma (4, 10). Consequently, the earlier detection of those XFS eyes that will convert to XFG is clinically important and may facilitate long-term visual preservation.
Research data suggest that scanning laser polarimetry can detect early glaucomatous structural damage (11–13). Polarimetric retinal nerve fiber layer thickness (RNFLT) may already be reduced in perimetrically normal eyes with structural glaucomatous damage (14). In addition, scanning laser polarimetry provides useful information for the assessment of early glaucomatous damage (11–17). However, there is currently limited information on the development of RNFLT damage in eyes with XFS (18, 19). Therefore, the aim of the present investigation was to assess the clinical value of RNFLT measurement with scanning laser polarimetry in untreated XFS eyes with daytime IOP in the normal range.
Methods
Design
This controlled, hospital-based observational study took place from September 2007 until September 2011 in the Glaucoma Unit of 1st University Department of Ophthalmology, AHEPA Hospital, Thessaloniki, Greece. Prospectively recruited participants were analyzed in a cross-sectional fashion. The protocol adhered to the tenets of the Helsinki Declaration and was approved by the institutional review board of the Medical School of Aristotle University, Thessaloniki, Greece. All participants gave informed consent before entering the study. The investigation was registered with Clinicaltrials.gov (identifier: NCT01022281).
Participants
All XFS participants were recruited consecutively from the Glaucoma Unit of the 1st University Department of Ophthalmology, AHEPA Hospital, and the diagnosis was confirmed by one of us (A.G.P.K.). The XFS group consisted of all newly diagnosed subjects with typical clinical evidence of exfoliation material upon the pupillary border or the anterior lens capsule after pupillary dilatation and normal office IOP. The control group comprised consecutive subjects attending the general outpatient service for a routine ophthalmic examination who did not demonstrate any ocular abnormality. After the initial evaluation at the outpatient service, all suitably qualified normal participants were invited to attend the Glaucoma Unit of the 1st University Ophthalmology Department of the AHEPA Hospital for further evaluation. The nature of the investigation was fully explained and their consent was obtained.
During the study visit, all participants underwent a comprehensive ophthalmic examination including best-corrected visual acuity (BCVA) testing, slit-lamp biomicroscopy, 3 Goldmann tonometry measurements (performed approximately every 2 hours between 9 am and 4 pm), gonioscopy, ultrasound pachymetry, standard automated perimetry with the Humphrey 24-2 SITA Standard program, dilated funduscopy with a 60-D hand-held lens, and scanning laser polarimetry with the GDx-VCC (Carl Zeiss Meditec, Dublin, CA, USA, software version 5.5.0). All GDx-VCC scans were performed by the same experienced investigator (A.T.D.). One randomly selected eye of each participant was analyzed if both eyes were eligible. Inclusion criteria were age between 55 and 75 years; a reliable normal visual field test (the first test was discarded and all cases had false-positive and false-negative responses lower than 33% and fixation losses lower than 20%); and at least 2 high-quality GDx-VCC scans (quality score ≥8). Exclusion criteria were history or signs of neurodegenerative or neurologic disease, any optic neuropathy, diabetes mellitus, systemic or topical therapy with corticosteroids, optic disc appearance compatible with glaucoma (i.e., neuroretinal rim thinning, optic disc hemorrhages, RNFLT defects, intereye asymmetry of cup-to-disc ratio >0.2), current or past use of glaucoma medications, IOP >20 mm Hg in any of 3 examinations at different times during office hours in any eye, visually significant cataract, visual acuity <0.5, ametropia higher than ±5 D, central corneal thickness (CCT) <500 μm or >600 μm, clinically significant ocular surface disease, corneal conditions preventing optimal image acquisition with GDx-VCC, previous ocular surgery, and presence of atypical polarization pattern with GDx-VCC. An atypical retardation image is characterized by irregular patches of elevated retardation values that do not match the expected retardation distribution based on the RNFL anatomy (20).
Statistical analysis
Normality of data was tested with the Kolmogorov-Smirnov test. The Student t test was employed if data were normally distributed, whereas the Mann-Whitney U test was used for non-normally distributed data. Results are reported as median and interquartile range (IQR) for the non-normally distributed parameters, and mean and SD for normally distributed parameters. The correlation between each of the GDx-VCC parameters and IOP, CCT, cup-to-disc ratio, Snellen BCVA, Humphrey mean deviation (MD), and pattern standard deviation (PSD) was examined with Spearman correlation coefficient (ρ). All reported p values were 2-tailed with p<0.01 considered as significant. The SPSS version 18.0 software package (SPSS, Inc., Chicago, IL, USA) was used for all statistical analyses.
Results
Sixty-four consecutive subjects with XFS (median age 69 years, 42% men) and 72 normal controls (median age 60 years, 37% men) were included in the current investigation (Tab. I). The characteristics of the participants are shown in Table I. The IOP was within the normal range in both groups, but it was higher in the XFS group: median (IQR) 19.0 (16.0–21.0) vs 16.0 (13.3–17.0) mm Hg; Mann-Whitney U test, p<0.001. There was no significant difference in CCT between the groups (542 [24] vs 550 [23] μm; Student t test, p = 0.049). The vertical cup-to-disc ratio was statistically greater in the XFS group compared to controls: median (IQR) 0.4 (0.3–0.5) vs 0.3 (0.2–0.4); Mann-Whitney U test, p = 0.001; however, the between-group difference was not clinically significant. For the XFS group, MD was significantly worse: median (IQR) −0.71 (–0.99 to −0.46) vs −0.29 (–0.66 to 0.23) dB; Mann-Whitney U test, p<0.001, and PSD was significantly more positive: median (IQR) 1.1 (0.8–1.5) vs 0.7 (0.4–1.1) dB; Mann-Whitney U test, p = 0.001, than for the control group. Nevertheless, these values were within the normal range for both groups.
Participant Characteristics
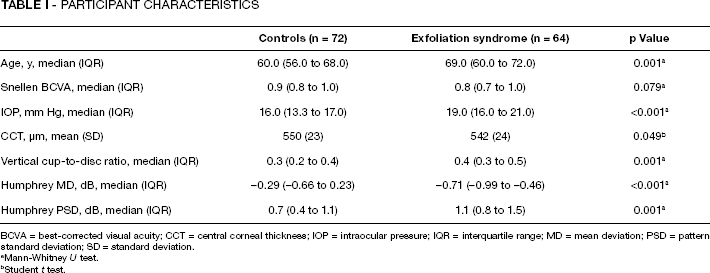
BCVA = best-corrected visual acuity; CCT = central corneal thickness; IOP = intraocular pressure; IQR = interquartile range; MD = mean deviation; PSD = pattern standard deviation; SD = standard deviation.
Mann-Whitney U test.
Student t test.
The 2 groups demonstrated statistically significant differences in all GDx-VCC parameters (Tab. II). Compared to the healthy controls, all RNFLT parameter values were significantly lower in the XFS group (p<0.001 for all comparisons). The RNFLT modulation parameter (TSNIT SD) was significantly lower in the XFS group (Mann-Whitney U test, p<0.001). The nerve fiber indicator (NFI) was significantly greater in the XFS subjects compared to normal controls: median (IQR) 25.0 (22.0–29.0) vs 15.0 (12.0–20.0); Mann-Whitney U test, p<0.001. There was no correlation between the measured RNFLT (TSNIT average, superior average, and inferior average) and age, vertical cup-to-disc ratio, CCT, and Snellen BCVA for either group (Tab. III).
Comparison Of The Most Important Retinal Nerve Fiber Layer Thickness Parameters Provided On The Gdx-Vcc Report
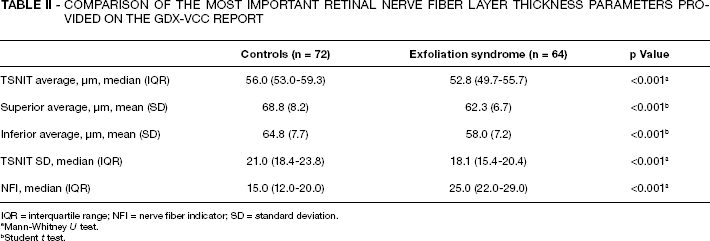
IQR = interquartile range; NFI = nerve fiber indicator; SD = standard deviation.
Mann-Whitney U test.
Student t test.
Correlation Between Gdx-Vcc Parameters And Clinical Parameters For The 2 Groups
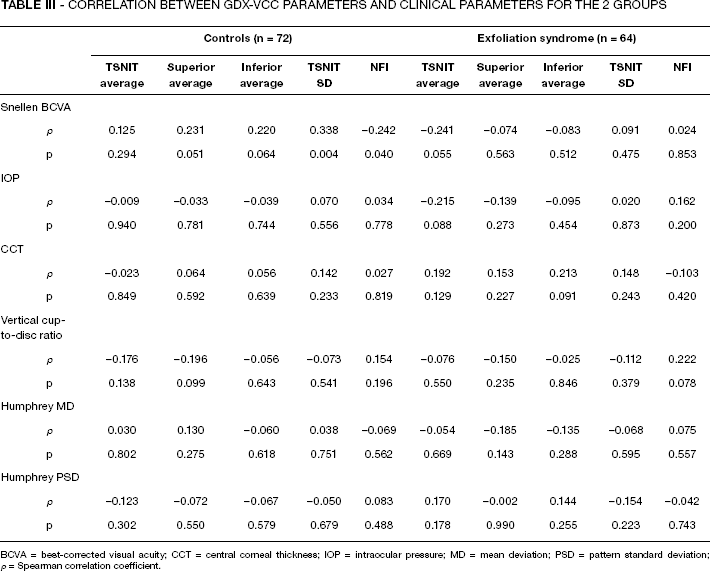
BCVA = best-corrected visual acuity; CCT = central corneal thickness; IOP = intraocular pressure; MD = mean deviation; PSD = pattern standard deviation; ρ = Spearman correlation coefficient.
Discussion
Exfoliation syndrome is a common condition worldwide (21–23) and eyes with exfoliation may convert to XFG at a rate of approximately 30% per decade (9). Exfoliative glaucoma is the most common cause of secondary open-angle glaucoma, and is characterized by rapid and serious progression (24–27). Still, little attention has been paid to the detection of those XFS eyes that are at risk for conversion to XFG. Early initiation of treatment in these cases may prevent the development of clinically significant glaucomatous damage and avert long-term loss of vision. Although diurnal IOP monitoring may detect some XFS patients with abnormal fluctuation of IOP (10, 18), this procedure is not feasible for most individuals at risk in routine clinical practice. Therefore, diagnostic methods that do not require hospitalization but provide clinically useful information on early glaucomatous damage in XFS may gain an important role in detection of conversion from XFS to XFG.
In this cross-sectional study with prospectively enrolled participants, we employed GDx-VCC for the comparison of RNFLT of healthy controls and individuals with XFS and normal daytime IOP. We observed that XFS eyes exhibited significantly thinner RNFLT compared to healthy control eyes. Indeed, all RNFLT parameters with major clinical importance (TSNIT average, superior average, inferior average) showed similar differences between the 2 groups, suggesting that thinning of RNFLT was diffuse in patients with XFS. Though our XFS patients were somewhat older than the control subjects, we do not think that this was the reason for the between-group RNFLT difference. Aging causes a mild age-related RNFLT reduction. The calculated figures for healthy subjects are 0.08, 0.16, and 0.12 μm per year for GDx-VCC TSNIT average, superior average, and inferior average, respectively (28). In our study, considering the 9-year median age difference between the groups, age-related RNFLT reduction would only be responsible for a loss of approximately 0.72 μm, 1.44 μm, and 1.08 μm for TSNIT average, superior average, and inferior average, respectively. These figures are much smaller than those found by us. Thus, age cannot account for the differences observed in the 2 groups of our study. This and the significant between-group difference in visual field MD and PSD (which are age-corrected, thus age-independent parameters) show that our groups did differ in RNFLT independently from their age difference. In addition, the significant between-group difference of TSNIT SD (a modulation parameter which describes the difference between the superior/inferior and temporal/nasal sectors) also suggests that the differences we observed in the RNFLT parameters were not the result of an age-related RNFL thinning. Since BCVA did not differ between the groups, the potential influence of cataract on the signal-to-noise ratio (which may cause virtual thinning of the measured RNFLT) can be excluded for the XFS group. Therefore, we think that the between-group differences were caused by RNFLT loss predominantly at the superior and inferior sectors, which is typical for early glaucoma (29, 30). Thus, our findings show that the RNFLT reduction in these normotensive XFS eyes was predominantly caused by early glaucomatous structural damage, which became detectable prior to the development of meaningful visual field loss. Furthermore, NFI, a composite index of probability of glaucomatous damage, was significantly higher in the XFS eyes. However, it should be noted that the XFS group also demonstrated higher mean IOP (within the normal range), higher visual field MD and PSD, and greater vertical cup-to disc ratio, which were statistically (but not clinically) significantly worse than the control group.
Our results support recently published data on the value of scanning laser polarimetry in evaluating conversion from XFS to XFG. In the first study on the subject, Gumus et al (18) employed an early version of the GDx platform with a fixed corneal compensator. These authors reported that subjects with XFS and high diurnal IOP fluctuation (>5 mm Hg) demonstrated thinner RNFL compared to normal controls. On the contrary, eyes with XFS and diurnal IOP fluctuation ≤5 mm Hg had RNFL thickness similar to controls. However, perhaps due to the limited statistical power of the study, no real difference was detected when polarimetric RNFLT values of the XFS group with higher IOP fluctuation were compared to those of the XFS eyes with lower IOP fluctuation. In a subsequent study by Kozobolis et al (19), participants with XFS and normal office-hour IOP had thinner RNFL compared to age-matched controls. Our current results support these findings in a larger cohort of patients and suggest that scanning laser polarimetry may help clinicians to detect XFS eyes at risk for conversion. In our study, all parameters in eyes with XFS were labeled as “within normal limits” by the software of the instrument. Accordingly, software-provided automatic identification of XFS eyes at risk for conversion to XFG was not feasible. However, when the clinician focuses on the individual superior and inferior RNFLT values and the value of TSNIT SD, eyes with thinner superior and inferior RNFLT can be identified even if all RNFLT parameters are within the statistically normal range. Based on published results (18), such XFS eyes are at a significant risk for conversion to XFG; thus the clinician can consider in each case if initiation of therapy is warranted. Interestingly, we found practically no correlation between RNFLT and BCVA, IOP, cup-to-disc ratio, CCT, MD, or PSD, which indicates that none of these clinical parameters can directly substitute quantitative RNFLT measurement in XFS.
In addition, our results substantiate previous observations suggesting a clinically demonstrable thinning of the neuroretinal rim in eyes with XFS (7). The precise explanation for these findings, however, remains unclear. One potential mechanism that could partly account for these data is the notion that XFS is associated with ocular or systemic hemodynamic dysregulation. Because exfoliation material has been found in numerous organs including extraocular blood vessels, XFS can be viewed as a multisystem fibrillopathy (4). Although not supported by all existing literature (31–33), circulatory defects and vascular disorders in persons with XFS have been reported. For example, circulatory impairment at the central retinal artery, the ophthalmic artery, and the posterior ciliary arteries have been described in eyes with XFS (34, 35). In addition, extraocular capillary and large-vessel dysfunction, as well as cardiovagal dysregulation, have been reported in persons with XFS (36–39). Therefore, at least in principle, vascular insufficiency of the optic nerve could result in thinning of the RNFL in some eyes with XFS. Even in this case, however, it remains unknown if XFS patients with circulatory compromise would be at risk for conversion to XFG.
A second, more plausible explanation for our findings may be the potentially worse 24-hour IOP characteristics of our XFS group. Our inclusion criteria required 3 office-hour Goldmann IOP readings <21 mm Hg for all participants. Although both the XFS and the control groups did have mean IOP well below 21 mm Hg, the XFS group had higher mean IOP within the normal range compared to controls. The IOP findings are in agreement with population-based studies showing that eyes with XFS have statistically greater IOP within the normal range than eyes without XFS (40, 41). This view is supported by Gumus et al, who reported greater diurnal IOP fluctuation in XFS eyes associated with RNFL thinning (18). Because 24-hour IOP monitoring was not performed in our study (as it is not performed in routine clinical care), it is feasible that the worse mean, fluctuation, or peak 24-hour IOP in the XFS group of our study directly resulted in RNFL damage (42). This may be a fruitful line of future investigations. It is relevant that Puska and Harju observed with confocal scanning laser ophthalmoscopy no visible optic disc damage in those XFS subjects with normal IOP and low IOP fluctuation (43). These authors concluded that XFS per se might not constitute a risk factor for optic disc damage in normotensive XFS with small diurnal IOP fluctuation (43).
In our study, the XFS group had statistically significantly worse cup-to-disc ratio and perimetry indices (MD and PSD) compared to the control group. These differences in retinal sensitivity and the clinical appearance of the optic disc may indicate that in our sample, some eyes with XFS already had early structural alterations accompanied by subtle functional deficits. Therefore, it is conceivable that some normotensive XFS eyes in our study may have entered the process of conversion to early XFG.
Our study has some limitations. As discussed above, the study groups were not age matched. Another limitation of the study is that circadian IOP measurements were not performed in our study group and consequently, adverse IOP characteristics such as spikes above 22 mm Hg may have occurred and remained undetected. It should also be noted that our investigation employed a cross-sectional design. Therefore, our results do not necessarily indicate that our participants with XFS will unavoidably convert to XFG, because a prospective cohort design would be needed to investigate this possibility.
Our data indicate that otherwise healthy eyes with XFS can have RNFL thinning. These observations support the notion that the presence of exfoliation material in otherwise healthy eyes with apparently normal office-time IOP may be a risk factor for structural damage and progression to glaucoma. These results also highlight the need for clinical vigilance, patient counseling, and appropriate follow-up in XFS. Scanning laser polarimetry represents an easy to use, quantitative clinical tool that may identify XFS eyes at risk for conversion to XFG. However, long-term, prospective research on larger patient cohorts is needed in order to set cutoff values for polarimetric RNFLT parameters that can indicate with certainty early structural damage in XFS. In the future, refining the ability of scanning laser polarimetry to more accurately identify eyes with XFS at risk for conversion to XFG will be desirable. To this end, different imaging technologies and larger prospective studies are needed to confirm our findings and better delineate XFS eyes at risk for conversion.
Footnotes
Acknowledgment
The authors thank Anna-Bettina Haidich, MD, PhD, Department of Hygiene, Aristotle University, Thessaloniki, Greece, for assistance with the statistical analysis.