
Abstract
Purpose
To evaluate visual performance and wavefront error after multifocal intraocular lens (MIOL) implant with or without capsular tension ring (CTR).
Methods
Sixty eyes of 60 candidates for phacoemulsification and MIOL implantation were included in the study and were randomly divided into 2 groups. Thirty eyes (group 1) were implanted with the AcrySof ReSTOR® SN60D3 MIOL and Corneal® ACPI 11 CTR and 30 eyes (group 2) received the same MIOL with no CTR.
Results
Twenty days and at 360 days after surgery, the uncorrected and corrected distance visual acuity at high and low contrast were not significantly different between the 2 groups. The root mean square (RMS) of ocular and internal wavefront error was significantly different in the 2 groups early after surgery and did not modify significantly over the 1-year follow-up period. The RMS of total and internal high-order aberrations and ocular and internal trefoil and coma aberrations were significantly lower in group 1 compared to group 2 (p<0.05). Ocular, corneal, internal modulation transfer function at high and low spatial frequencies and ocular, corneal, internal Strehl ratio were not significantly different between the groups. The IOL decentration and tilt were higher in group 1 compared to group 2.
Conclusions
ReSTOR MIOL was effective in improving visual performance and provided a good quality of vision due to a significant reduction of high-order spherical aberration. The implant of CTR additionally reduced the ocular wavefront error related to a reduction of third-order aberration related to better IOL position.
Introduction
Capsular tension rings (CTR) have been proven to be useful devices particularly in complicated cases of cataract surgery such as zonular weakness and dialysis mainly due to their capacity to maintain the capsule's circumference and to stretch the posterior capsule (1–4). Several studies report the use of CTR in normal cataract procedures in order to improve intraocular lens (IOL) centration by means of symmetrical stretch of the capsular bag.
Intraocular lens decentration is mainly caused by asymmetrical bag fixation (4, 5). Many IOL characteristics such as design, total length, and optic and haptic materials influence lens centration (6, 7). Moreover, capsular rings have been proven to reduce incidence of delayed IOL decentration occurring during time related to asymmetrical capsule contraction (3).
Intraoperative IOL malposition or changes in postoperative IOL position related to capsule opacification can cause decrement of quality of vision, particularly with aspheric IOLs and multifocal IOLs (MIOL) (8–13).
Several authors demonstrated that the impairment of visual performance in eyes with decentered or tilted IOLs is related to the increment of third-order aberrations (14, 15). Moreover, it has been shown that aspheric IOLs induce higher amount of third-order aberration compared to spherical IOLs (16, 17).
Recently, Aliò et al (18) showed good efficacy of the combined implant of CTR and an aspheric diffractive MIOL with asymmetrical light distribution in terms of reduced high-order aberrations and, consequently, improved of quality of vision.
In a previous study, we demonstrated that patients implanted with AcrySof ReSTOR® MIOL had a higher amount of coma aberration compared to the Tecnis ZM900 MIOL and a low amount of spherical aberrations similar to an aspheric IOL (19).
The aim of our study was to analyze wavefront error, visual performance, and IOL position after implant of AcrySof ReSTOR MIOL with or without CTR and evaluate the influence of the CTR in the optical performance of the implanted eyes.
Methods
Sixty consecutive eyes of 60 patients referred to the Ophthalmology Department of Chieti University from June 2011 to August 2011 for cataract surgery and MIOL implantation were enrolled in this comparative clinical trial.
Inclusion criteria were age between 50 and 75 years, axial length between 23.0 and 24.0 mm, and corneal preoperative astigmatism less than 1.00 D.
Exclusion criteria were anterior segment pathologic alterations, such as chronic uveitis, zonular dialysis, pseudoexfoliation syndrome, glaucoma, and diabetes; other ocular pathologies impairing visual function; previous anterior or posterior segment surgery; and intraoperative or postoperative complications.
Patients were randomized to receive a multifocal diffractive IOL with or without CTR. Group 1 consisted of 30 patients implanted with AcrySof ReSTOR SN60D3 IOL and Corneal® ACPI 11 CTR and group 2 of 30 patients with ReSTOR MIOL with no CTR. A computer-generated randomization list of 60 patients was prepared. Patients were assigned to one of the two treatments with the probability of 0.5 for each group. The next randomization number was assigned to a patient if he or she fulfilled the inclusion and exclusion criteria.
The AcrySof ReSTOR IOL (Alcon Laboratories Inc., Fort Worth, Texas, USA) has a single-piece 6-mm biconvex optic of hydrophobic flexible acrylic material with a central 3.6-mm apodized diffractive design and a peripheral refractive area. Apodization allows a gradual tapering of the diffractive steps from the center to the outside edge of the lens to create a smooth transition of light between the distance, intermediate, and near focal points. This is obtained by means of a precise reduction in step heights from 1.3 to 0.2 μm. The outer ring of the AcrySof ReSTOR IOL that surrounds the apodized diffractive region is dedicated to focusing light for distance vision. The CTR ACPi 11 (Corneal Laboratories, Paris, France) is a polymethylmethacrylate injectable capsular ring with 11-mm diameter.
A complete ophthalmologic examination, including medical and ophthalmologic history, was performed and patients were informed about the surgery and all signed an informed consent form. Ethical committee approval was obtained for the study.
In group 1, a standardized uneventful small-incision phacoemulsification with IOL implantation was performed by a single surgeon (L.M.). After a 3.2-mm near clear corneal tunnel was made, a curvilinear capsulorhexis was created. Phacofracture in the capsular bag was followed by automated irrigation/aspiration of the cortical remnants. The IOL was implanted in the capsular bag. The incision was not sutured.
In group 2, the same procedure was adopted except for the implantation of the CTR in the capsular bag preceding the MIOL implant.
In all cases, postoperative therapy consisted of ofloxacin 0.3% and dexamethasone 0.2% eyedrops 4 times daily for 3 weeks.
Patients were examined 20 days and 360 days after surgery.
The main outcome measures were spherical equivalent (SE) cycloplegic subjective refraction, uncorrected distance visual acuity (VA) at high and low contrast (HUDVA and LUDVA, respectively), corrected distance VA at high and low contrast (HCDVA and LCDVA, respectively), distance-corrected near VA (DCNVA), and corrected near VA (CNVA).
Ocular, corneal, and internal root mean square (RMS) of high-order aberrations (HOA) and ocular, corneal, and internal Zernike coefficients of second-, third-, and fourth-order aberrations at 4, 5, and 6 mm of analysis and ocular, corneal, and internal modulation transfer function (MTF) and Strehl ratio were calculated at the same diameters for all patients.
In addition, IOL decentration in x-axis and y-axis were evaluated in both groups.
Moreover, the anterior and posterior capsule were examined after dilating the pupil to establish the presence of anterior and posterior capsule opacification (ACO and PCO, respectively).
High- and low-contrast visual acuity evaluation
High-contrast logMAR (log [minimum angle of resolution]) VA with or without best spectacle correction and low (10% of maximal contrast) contrast logMAR VA with or without best refraction in place were measured using the ZyQV kit (Zyoptix™ Quality of Vision, Technolas Bausch & Lomb, Rochester, New York, USA). Each patient was invited to read the chart until 4 letters were missed in the smallest line. The final VA was calculated by multiplying the logMAR value of each letter (0.02) by the number of misread letters and adding this value to the lowest line read.
Wavefront aberration analysis
The HOA was measured using OPD-Scan II and OPD-Station software (Nidek Co. Ltd., Aichi, Japan) based on retinoscopic principles using infrared light, as already described (20).
The OPD-Scan II measures the corneal topography and ocular wavefront, enabling the determination of the corneal and internal aberration of the eye. It defines and calculates ocular, corneal, and internal aberrations in terms of Zernike polynomials up to the sixth order. The first (Z11, Z1−1), second (Z20, Z22, Z2−2), third (Z31, Z3−1, Z33, Z3−3), fourth (Z40, Z42, Z4−2, Z44, Z4−4), fifth (Z51, Z5−1, Z53, Z5−3 Z55, Z5−5), and sixth (Z60, Z62, Z6−2, Z64, Z6−4, Z66, Z6−6) order aberrations expressed as Zernike coefficients values were measured in μm.
The ocular, corneal, and internal total (from first to sixth) and high-order wavefront error (from third to sixth) expressed in RMS represent the average of the square root of the wavefront errors, measured in μm.
Aberration measurements were measured 20 days after surgery after pupil dilatation with phenylephrine. For each patient, 4.0-, 5.0-, and 6.0-mm pupil diameters were chosen as reference pupil diameters in order to obtain comparable data.
The ocular, corneal, and internal RMS of total HOA were calculated for each patient examination as the mean value of 3 reliable consecutive measurements.
In addition, the absolute value of Zernike coefficient of astigmatism (Z22, Z2−2), third-order coma (Z31, Z3−1), third-order trefoil (Z33, Z3−3), and fourth-order spherical (Z40) aberration were calculated for each patient.
The ocular, corneal, and internal MTF curves from 0 to 60 cycles per degree (cpd) obtained from aberrations and the ocular, corneal, and internal Strehl ratio for total high-order aberration were used as metric of vision quality.
Intraocular lens position
To assess IOL decentration and tilt, single best images obtained for 0°-180° and 90°-270° meridians by means of Pentacam Scheimpflug System (Oculus Inc., Berlin, Germany) at 20 and 360 days were collected for each patient. The images were blinded for patient information and randomized. A single reader (L.T.) then evaluated the decentration and tilt with an in-house closed-source software developed in MatLab 2009b® (see www.ophthalmology.unich.it for further details). The reproducibility of the 3 measurements was evaluated with intraclass correlation coefficient (ICC). In case of low reproducibility, the 3 measurements were repeated.
Capsule fibrosis assessment
Anterior capsule fibrosis was assessed with focal and retroillumination photographs obtained with maximum pupil dilation using a Tomey video slit-lamp.
The ACO was subjectively graded as 0 = none, 1 = moderate: mild opacification not involving the whole capsulorhexis, 2 = severe: complete whitening of the capsule over the IOL optic.
Statistical analysis
In all patients, the postoperative follow-up of the parameters evaluated in the study was set 20 days after surgery.
The main parameters evaluated included the visual parameters (SE, HUDVA, HCDVA, LUDVA, LCDVA, DCNVA), the ocular, corneal, and internal aberration parameters (HOA RMS and Zernike coefficient of astigmatism, coma, trefoil, and spherical aberrations), the metrics of vision quality (MTF and Strehl ratio) at 4, 5, and 6 mm of analysis, analysis of IOL position (decentration in X and Y axis, tilt around X axis and Y axis), and capsule fibrosis assessment (ACO, PCO). All parameters evaluated at 20 days and 360 days after surgery were summarized as median and range. The results are reported separately for each lens.
All statistical analysis was performed using nonparametric tests. The comparison between lenses in visual aberrometric and decentration parameters was performed using Mann-Whitney U test; the Wilcoxon U test was applied to evaluate the difference between 20 and 360 days postoperatively. The chi-square test or Fisher exact test, where appropriate, were performed to evaluate the difference between groups in ACO and PCO.
All statistical tests were evaluated at an α level of 0.05. Statistical analysis was performed using SPSS® Advanced Statistical 11.0 software (SPSS Inc., Chicago, Illinois, USA).
Results
Visual outcome
Twenty days after surgery, the HUDVA was 0.20 (0.00 to 0.30) logMAR and 0.10 (0.00 to 0.40) logMAR and the HCDVA was −0.00 (−0.10 to 0.00) logMAR and 0.00 (−0.10 to 0.10) logMAR in group 1 and group 2, respectively (p = NS). The LUDVA was 0.40 (0.30 to 0.50) logMAR and 0.45 (0.20 to 0.70) logMAR and the LCDVA was 0.30 (0.20 to 0.40) logMAR and 0.40 (0.20 to 0.50) logMAR, respectively (p = NS). The UDVA and CDVA at high and low contrast did not modify significantly at 1 year (Tab. I). The DCNVA was 1.50 (1.00 to 4.00) J in the first group and 1.50 (1.00 to 5.00) J in the second group (p = NS) at 20 days and 1.25 (1.00 to 5.00) and 1.25 (1.00 to 3.00) respectively at 1 year. The CNVA was 1.00 J in 100% of cases in both groups.
- Visual Parameters for the Control Group and Study Group at 20 and 360 Days After Surgery, Median (Range) a
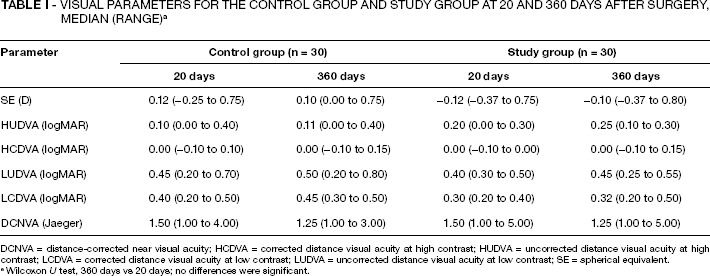
DCNVA = distance-corrected near visual acuity; HCDVA = corrected distance visual acuity at high contrast; HUDVA = uncorrected distance visual acuity at high contrast; LCDVA = corrected distance visual acuity at low contrast; LUDVA = uncorrected distance visual acuity at low contrast; SE = spherical equivalent.
Wilcoxon U test, 360 days vs 20 days; no differences were significant.
Refractive outcome
The median (range) SE was −0.12 (−0.37 to 0.75) D in group 1 and 0.12 (−0.25 to 0.75) D in group 2 (p = NS) at 20 days and −0.10 (−0.37 to 0.80) D and 0.10 (0.00 to 0.75) D respectively at 360 days (p = NS) (Tab. I).
Postoperatively, the RMS of ocular and internal total HOA and absolute value of ocular and internal Zernike coefficient of coma and trefoil aberrations were significantly different in the 2 groups. At 20 and 360 days, ocular RMS HOA was significantly lower in group 1 compared to group 2 at 4 and 5 mm of analysis (p<0.05). Internal RMS HOA was significantly lower in group 1 compared to group 2 at 4 mm of analysis (p<0.05). Ocular and internal Z33 and Z31 at 5 mm were significantly lower in the study group compared to the control group (p<0.05) (Tab. I).
Corneal Z40 was also significantly different in the 2 groups at 5 and 6 mm of analysis (Tab. I).
Ocular, corneal, internal MTF at high and low spatial frequencies and ocular, corneal, and internal Strehl ratios were not significantly different between the groups.
Lens decentration and tilt
Intraocular lens decentration in x-axis at 20 days was −0.08 ± 0.58 and 0.13 ± 0.44 in group 1 and group 2; decentration in y-axis was −0.10 ± 0.03 and 0.02 ± 0.15, respectively (Tab. III).
Intraocular lens tilt around x-axis was 4.59 ± 7.19 degrees in the control group and 2.34 ± 8.45 degrees in the study group and IOL tilt around y-axis was 9.19 ± 7.34 and 2.28 ± 9.16 degrees, respectively (Figs 1, 2).
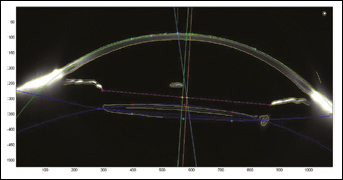
Image at 0°-180° meridian by means of Pentacam Scheimpflug System (Oculus Inc., Berlin, Germany) 20 days after surgery showing intraocular lens (IOL) decentration as the distance between pupillary axis (orange line) and IOL axis (green line) and IOL tilting as the angle between pupillary axis (orange line) and IOL axis (green line) in a patient implanted with a multifocal IOL without capsular tension ring.
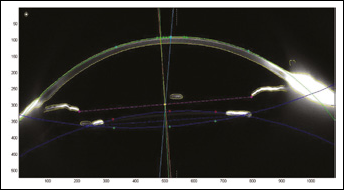
Image at 0°-180° meridian by means of Pentacam Scheimpflug System (Oculus Inc., Berlin, Germany) 20 days after surgery showing intraocular lens (IOL) decentration as the distance between pupillary axis (orange line) and IOL axis (green line) and IOL tilting as the angle between pupillary axis orange line) and IOL axis (green line) in a patient implanted with a multifocal IOL and capsular tension ring.
The reliability of the methods was evaluated for decentration in the x-axis (ICC 0.984) and y-axis (ICC 0.933) and for tilt in the x-axis (ICC 0.843) and y-axis (ICC 0.982). The variation between 20 and 360 days postoperatively for decentration and tilt was not statistically significant (Tab. II).
- Aberration Parameters for the Control Group and Study Group at 20 and 360 Days after Surgery, Median (Range) a
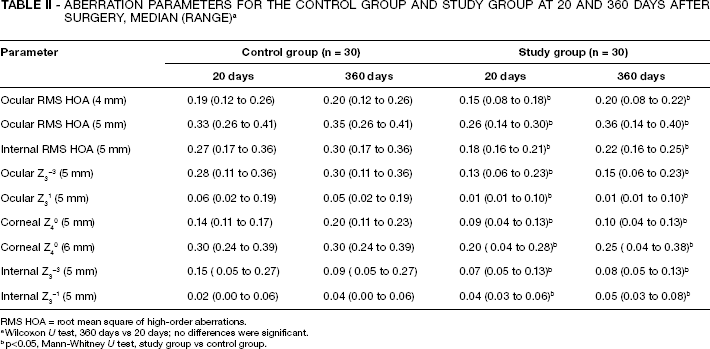
RMS HOA = root mean square of high-order aberrations.
Wilcoxon U test, 360 days vs 20 days; no differences were significant.
p<0.05, Mann-Whitney U test, study group vs control group.
- Mean ± Standard Deviation of Tilt and Decentration Values
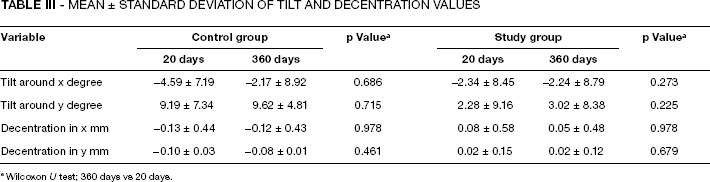
Wilcoxon U test; 360 days vs 20 days.
Capsular biocompatibility
In all patients, rhexis overlaid the anterior optic surface for 360°.
At 20 days, the percentage of patients with ACO was 0% in both groups, at 360 days 33% of patients in group 1 and 30% of patients in group 2 had a grade 1 ACO, and 12% and 10%, respectively, had a grade 2 ACO.
Discussion
Modern IOL implantation is a safe and efficacious surgical procedure which usually yields good VA with either monofocal or multifocal IOLs. Nevertheless, several studies demonstrated problems in vision quality such as reduced contrast sensitivity and visual symptoms such as haloes, glare, and blurred night vision, particularly with conventional spherical monofocal IOLs and MIOL (21, 22).
Recently, some technical innovations have been introduced in IOL manufacturing to improve the visual performance of postcataract patients.
It has been demonstrated that the spherical design of the conventional IOLs may induce disturbing visual symptoms associated with the increase of positive spherical aberration that can lead to decreased quality of the optical system.
Intraocular lenses of aspheric design have been manufactured either with monofocal or multifocal optics to induce a negative spherical aberration and to reduce the overall amount of ocular spherical aberration. Several authors demonstrated a better visual performance, particularly a higher contrast sensitivity in patients implanted with aspheric IOLs compared to conventional IOLs (23–26).
Recently, new attempts to optimize quality of vision promoted the manufacture of customized IOLs to correct preoperative HOAs (27).
Nevertheless, IOL implantation—spherical, aspherical, or customized—has an important limitation: the precision of lens positioning (6–15).
Several studies described the decrement of vision quality when there is a tilt or decentration of the optic, related particularly to the increment of HOAs of third order (8, 10, 14). Intraocular lens decentration is mainly caused by asymmetric bag fixation (4, 5). Many IOL characteristics such as design, total length, and optic and haptic materials influence lens centration (6, 7). Moreover, IOL decentration is associated with asymmetric contraction of a fibrotic capsule because of unequal shrinkage of the lens capsule (28–30).
Several studies report the use of CTRs to improve intraoperative IOL centration of uncomplicated cataract surgery by means of symmetrical stretching of the capsular bag and to reduce delayed IOL decentration related to asymmetric capsule contraction by means of inhibition of myofibroblastic lens epithelial cells (LEC) metaplasia and migration. The CTR helps to keep the anterior capsule distant from the anterior optic surface, thus reducing ACO, and creates a discontinuous capsular bend, reducing the incidence of PCO (3).
Some studies demonstrated the use of CTR to improve IOL centration and tilt (18, 31).
Aliò et al (18) demonstrated that the combined implant of Acri.lisa 366 D multifocal diffractive IOL and CTR improves the optical performance of the eye with better postoperative refraction, significant reduction of HOA, and significant increase of modulation transfer function and Strehel ratio, probably related to better IOL centration.
In our study, we compared patients implanted with the AcrySof ReSTOR IOL with or without a CTR by evaluating the visual performance and wavefront error.
At early and long term after surgery, the 2 groups did not show statistically significant differences in excellent distance VA at high and low contrast and good near VA.
However, the RMS of ocular and internal total HOAs were significantly lower in the group with CTR than in the group with only MIOL implanted at 4 and 5 mm of analysis. Analyzing the difference of the absolute values of Zernike coefficients, a significantly lower amount of ocular and internal coma and trefoil aberrations were found. Ocular Z33 at 5 mm was 0.13 μm in the study group and 0.28 μm in the control group (p = 0.045) and internal Z33 was 0.07 μm and 0.15 μm, respectively (p = 0.045). Ocular Z31 at 5 mm was 0.01 μm in group 1 and 0.06 μm (p = 0.045) in group 2 and internal Z31 was 0.02 μm and 0.04 μm (p = 0.045). Wavefront error did not change significantly at 360 days after surgery compared to the previous time point.
In a previous study, we demonstrated that ReSTOR IOL induce a lower amount of spherical aberration compared to spherical monofocal and MIOL, probably related to central apodization of the optics (19). Several studies demonstrated a higher amount of third-order aberrations when aspheric IOL are decentered compared to spherical IOLs, demonstrating the limitation of correcting spherical aberration with aspheric IOLs when correct positioning of the IOL is not obtained because of decentration and/or tilt (16, 17).
In our patients, the lower value of third-order aberrations in the group with CTR is probably related to a lower value of decentration and tilt of the MIOL.
The better centration and positioning of the MIOL at 20 days after surgery is probably related to the symmetrical stretch of the CTR on the capsule that allowed better positioning of the lens in the capsular bag.
We did not observe delayed decentration after 1 year, which has been found to be associated with asymmetric contraction of a fibrotic capsule (29, 30).
Anterior capsule fibrosis is based on the fibrous metaplasia of residual LEC attached to the inner surface of the anterior capsule when they come into contact with the IOL, and usually occurs in the first months after surgery (31).
In our cases, we found in both groups a low incidence of ACO without significant differences between the 2 groups, probably related to IOL material and design characteristics of the AcrySof IOLs and particularly to the tacky nature of the AcrySof material allowing tenacious adherence of the anterior capsule to the lens optic with reduction of capsule opacification phenomena.
The better centration of the patients with MIOL and CTR was not correlated with a greater quality of vision evaluated with MTF curves at all analyzed spatial frequencies and Strehel ratio.
Some authors stated that when decentration of MIOL is equal to or higher than 0.7 mm or higher than 1.0 mm, visual performance significantly decreases (32, 33).
The good visual performance in patients with MIOL without CTR not significantly different from the group implanted with CTR due to the low amount of decentration in x- and y-axis, demonstrating the good stability of the AcrySof ReSTOR in the capsular bag. Nevertheless, combined implant of CTR and AcrySof ReSTOR improved optical performance by means of reduction of third-order aberrations.