
Abstract
Purpose
To evaluate the use of a femtosecond laser combined with a microkeratome in the preparation of posterior corneal disks for Descemet stripping automated endothelial keratoplasty (DSAEK).
Methods
This experimental study involved ultrathin DSAEK tissue preparation of 22 donor corneas unsuitable for transplantation. The first cut was performed with an Intralase® FS60 laser and the second cut with a Moria CBm 300-μm microkeratome. The thickness of the first cut was modified for each cornea to obtain a final graft thickness of less than 110 μm. Precut and postcut central pachymetry were performed with an ultrasonic pachymeter. Central endothelial cell density (ECD) was calculated before and 24 hours after tissue preparation.
Results
Final graft thickness was 105.0 ± 26.1 (SD) μm (range 65–117). The mean microkeratome head cut thickness was 324.5 ± 10.9 μm (range 310–345). Precut and postcut ECDs averaged 2250 ± 222 and 2093 ± 286 cells/mm2, respectively, representing 6.9% of cell loss. No corneas were perforated.
Conclusions
Femtosecond FS60 lasers and Moria CBm 300-μm microkeratomes can be used sequentially to prepare consistently thin DSAEK grafts with no irregular cuts or cornea perforations.
Introduction
Descemet stripping automated endothelial keratoplasty (DSAEK) has become the standard of care for Fuchs dystrophy and other causes of endothelial dysfunction (1). DSAEK consists of stripping a patient's diseased endothelium and replacing it with the healthy endothelium, Descemet membrane, and a layer of stroma prepared from a donor cornea with an automated microkeratome (2, 3).
An important limitation of DSAEK is that some eyes do not achieve good visual acuity despite a clear cornea and minimal residual astigmatism (4–6). This may be caused by interface irregularity, the presence of donor posterior stroma, or a thick endothelial graft (7–9). The influence of endothelial graft thickness on visual acuity in DSAEK is controversial, with some authors reporting better results with thinner grafts and others finding no correlation (10–15). However, studies evaluating this subject have either focused on relatively thick grafts (160–170 μm) or on grafts prepared by manual dissection (11–15). When grafts having less than 130 μm are evaluated, a positive correlation between thickness and visual acuity is obtained (9, 10), suggesting that an effect may exist under a certain thickness. Obtaining thin grafts carries a higher risk of donor corneal perforation. Therefore, it is necessary to develop a technique to create thin posterior lamellar grafts without wasting donor corneas.
The present article presents a new technique that combines the sequential use of a femtosecond (FS) laser with a microkeratome to create posterior donor lenticules with a targeted thickness of less than 110 μm.
Methods
This study was an institutional experimental laboratory investigation consisting of DSAEK tissue preparation on 22 human donor corneas. The corneas were unsuitable for transplantation due to positive donor serology results. Donor age and preservation to lamellar dissection time (storage time; see Tab. I) were recorded. Tissue was preserved in Eusol-C® (Alchimia SRL, Padova, Italy) at a constant temperature of 4°C before use.
- Donor Tissue Demographics, Data Obtained During Each Cut, And Endothelial Cell Density Before And 24 Hours Postcut
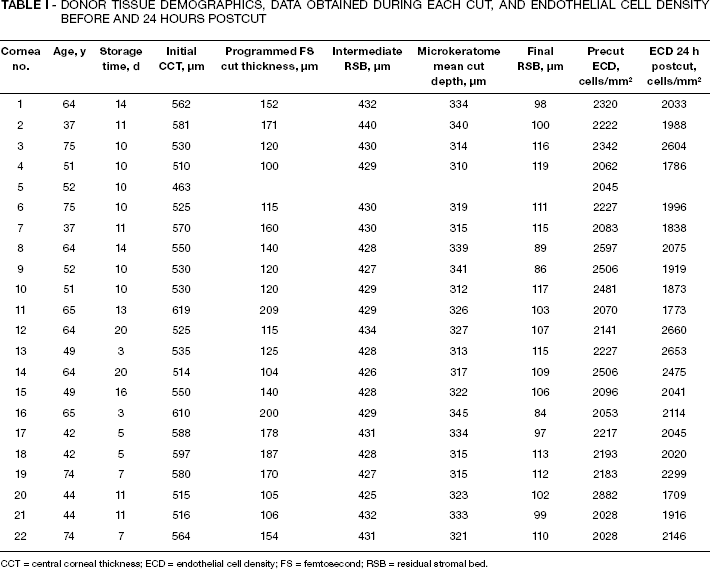
CCT = central corneal thickness; ECD = endothelial cell density; FS = femtosecond; RSB = residual stromal bed.
Each donor cornea had a 5-mm scleral rim and was mounted on an artificial anterior chamber (ALTK, Moria SA, Antony, France) filled with balanced salt solution (BSS®, Alcon Laboratories, Fort Worth, Texas, USA). The BSS® bottle was elevated to 220 cm and the tubing was clamped at 60 cm from the anterior chamber, to ensure a high and stable anterior chamber pressure.
In order to obtain the initial central corneal thickness (CCT), precut central pachymetry was performed with an ultrasonic pachymeter (Corneo Gage Plus® 50 MHz; Sonogage, Cleveland, Ohio, USA) after removal of the cornea epithelium. The first cut of the double-pass technique was performed with an Intralase® FS60 FS laser (Abbott Medical Optics, Santa Ana, California, USA), and the second cut with the Moria® CBm microkeratome 300 μm cutting head (Moria SA, Antony, France) (Fig. 1). The programmed FS cut thickness of the first cut was calculated as follows:
Programmed FS cut thickness = initial CCT - (theoretical microkeratome cut thickness + desired final graft thickness) The theoretical microkeratome cut thickness was considered to be 300 μm and the desired final graft thickness was 110 μm.
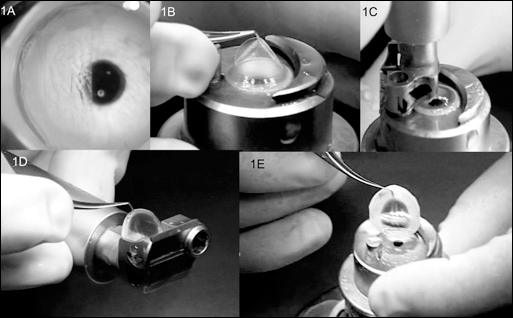
Donor cornea is assembled in an artificial anterior chamber and a first cut is performed with the femtosecond laser (A). The thickness of this cut is chosen in order to leave approximately 410–430 μm of intermediate residual stromal bed. The tissue is easily removed (B). The second cut is performed with a 300-μm microkeratome head (C, D) leaving a thin and smooth final residual stromal bed. The cornea is removed from the anterior chamber (E).
By replacing these values, this formula can be simplified as follows:
Programmed FS cut thickness = initial CCT − 410 μm.
Care was taken when positioning the donor tissue on the anterior chamber so that there was a regular ring of sclera appearing around the cornea. The FS cut was centered, having as reference the hole inside the anterior chamber, visible on the screen of the Intralase® (Fig. 1A). No suction ring was used and docking was straightforward. The FS settings were full lamellar cut with a diameter of 9.5 mm, raster energy 1.5 μJ, and anterior side cut at 90° with 2.7 μJ. A new applanation cone was used for each cornea. After laser passage, the disc of tissue was removed and central pachymetry was evaluated to obtain intermediate residual stromal bed thickness (Tab. I). The second cut was performed immediately afterward with the 300 μm microkeratome head, keeping the manual rotation speed constant and with total duration of approximately 3–5 seconds. Central pachymetry was again repeated to obtain final residual stromal bed thickness. The tubing was unclamped with the BSS bottle at 150 cm to avoid turbulence inside the anterior chamber. Donor tissue was removed by gently pulling the scleral rim from the top of the anterior chamber and then immersed in the storage medium. Endothelial cell density was calculated before and 24 hours after the cuts, using a noncontact specular microscope (SP4000 noncontact specular microscope; Konan Medical Corp., Fair Lawn, New Jersey, USA). A technician marked the center of at least 50 endothelial cells and the computer software estimated the area and the cell density of the entire cornea.
Results
Donor age was 56.1 ± 12.7 years (mean ± SD) and preservation to lamellar dissection time was 10.5 ± 4.6 days. Death to preservation time was less than 12 hours in all cases. Initial CCT after epithelial debridement was 548.4 ± 37.8 μm (range 463–619 μm; Tab. I). Cornea no. 5 (Tab. I) had an initial thickness of 463 μm, which would require a FS cut of 43 μm. This value is below the limit of the Intralase® depth range, which precluded cutting this cornea. The disc of tissue from the FS cut was easily removed in all cases.
Intermediate residual stromal bed was 429.7 ± 3.2 μm. The microkeratome mean cut depth was 324.5 ± 10.9 μm (range 310–345 μm; Tab. I). Final residual stromal bed was 105.1 ± 10.2 μm (range 84–119 μm). Average precut endothelial cell density was 2250 ± 222 cells/mm2 and postcut was 2093 ± 286 cells/mm2, representing 6.97% cell loss. No corneas were lost due to perforation, irregular cuts, or buttonholes.
Discussion
Despite excellent postoperative results, best-corrected visual acuity after DSAEK is sometimes less than that obtained with penetrating keratoplasty (16, 17). Several studies report that better results might be achieved with a smoother interface and thinner grafts (2, 9, 10). Neff and colleagues (10) reported that grafts ≤131 μm provided a statistically significant improvement in best-corrected visual acuity compared with thicker grafts. Several attempts have been made to develop a technique to create very thin DSAEK grafts, without wasting donor tissue (18–21).
A FS laser, without a microkeratome, was previously used for this purpose. However, the resulting surface was not as smooth as from a microkeratome and concentric folds would form due to compression or irregularity of the posterior stroma (22, 23). In addition, interface scatter may later appear (21).
The method we describe here, the double-pass technique, combines the sequential use of a FS laser and a microkeratome. The first pass is performed with the laser to avoid the variability of the microkeratome, but for the second cut the latter is used to obtain a smooth stromal bed (24). Posterior donor lenticules with a mean thickness of 105 μm were obtained and no cornea was perforated. An important aspect of this technique is that the thinner cut is done first, leaving a strong and thick cornea for the microkeratome. Because the anterior stroma is the strongest (25), this approach avoids irregular cuts and buttonholes during the microkeratome cut.
The desired final graft thickness can be obtained by changing the parameters of the laser, which can be programmed to cut at a customized depth for each cornea, according to the initial pachymetry. This avoids using nomograms and allows having only one microkeratome head available, in this case a 300 μm, but other heads would probably work as well. It also has the advantage of using equipment already available in most cornea centers. The target thickness of 110 μm was chosen essentially for safety reasons. This way, at least 410 μm of corneal tissue are cut with a 300 μm microkeratome head, minimizing the risk of perforation. Since the microkeratome we use usually cuts more than 300 μm (26), we found that aiming for a final thickness of 110 μm would actually result in thinner grafts (than 110 μm) without perforating. Because the microkeratome cut depth depends on several factors, such as intrachamber pressure, tissue thickness, and manual rotation speed, these factors are kept constant (tubing clamped at 60 cm when bottle is raised at 220 cm, FS cut first, 3–5 seconds manual rotation speed) in order to reduce variability.
In terms of endothelial cell loss, the cut performed by the FS is superficial, similar to the flaps produced in laser-assisted in situ keratomileusis (LASIK). Therefore, this cut should not induce any more cell loss than a regular LASIK flap. The second cut is performed immediately after the first to avoid further manipulation of the donor cornea. In the present study, mean endothelial cell loss from precut to 24 hours postcut was 6.9%, which is higher than the 3%–4% reported by other authors (22, 26, 27). However, the time interval between cutting the cornea and counting the cells is likely to be important when evaluating cell death, with longer intervals (as was the case in this study) being associated with lower final cell densities (28).
In conclusion, the technique described in this study combines the sequential use of a FS laser and a microkeratome to obtain posterior lamellar grafts with a mean thickness of 105 μm. More research is needed to determine the visual outcomes of this approach and to clarify whether there is an ideal graft thickness both in terms of visual recovery and endothelial cell loss.
Footnotes
Acknowledgment
The authors thank Robert Van Velze for help in setting the parameters of this study.