
Abstract
Purpose
To evaluate the influence of socioeconomic factors on visual acuity before cataract surgery.
Methods
The medical case notes of 240 consecutive patients listed for cataract surgery from January 1, 2010, at Grampian University Hospital, Aberdeen, were reviewed retrospectively. Patients with ocular comorbidity were excluded. Demographics, postal codes, and visual acuity were recorded. Scottish Index of Multiple Deprivation was used to determine the deprivation rank. Home location was classified as urban or rural. The effect of these parameters on preoperative visual acuity was investigated using chi-square tests or Fisher exact test as appropriate.
Results
A total of 184 patients (mean 75 years) were included. A total of 127 (69%) patients had visual acuity of 6/12 or better. An association was found between affluence and preoperative visual acuity of 6/12 or better (χ2trend = 4.97, p = 0.03), with a significant rising trend across quintile of deprivation. There was no evidence to suggest association between geographical region and preoperative visual acuity (p = 0.63).
Conclusions
Affluence was associated with good visual acuity (6/12 or better) before cataract surgery. There was no difference in preoperative visual acuity between rural and urban populations.
Introduction
Cataract surgery is the most commonly performed elective surgical procedure in the United Kingdom. In England, the crude surgical rate in 1990 was around 2/1000 (1), by 1997 this had increased to 3/1000 (2), and by 2005 peaked at around 6/1000 (3), an increase of close to 300% over 16 years. In the National Health Service (NHS), thresholds for listing for cataract surgery have become increasingly lenient in visual acuity (VA) term; in 1990, under 9% of eyes for surgery had an acuity 6/12 or better (4); by 1997, this had risen to 31% (5), and the most recent data from 2001–2006 showed this had increased to 43% (6).
The issues of appropriateness and possible overutilization of cataract surgery have been raised by several investigators (7-9). In Vancouver, Wright et al (8) reported that 27% of patients’ visual functions were the same or worse after surgery. In the United Kingdom, Black et al (7) found that 25% of patients’ visual function scores were unchanged or deteriorated after cataract surgery. The risk-benefit ratio of early cataract surgery is still unclear. Malik at al (10) argued that cataract surgery for those with VA of 6/12 or better may only be effective at monocular level and shows no improvement in the quality of life.
In Scotland, more than 90% of land is classified as rural and approximately 1 of the 5.2 million people in Scotland live in rural areas. The average population density of rural Scotland is 21 persons per square kilometer. Hence, access to the remote areas can be difficult, and nearly half of the rural population has to drive about an hour to get to urban areas (11). National Health Service Grampian is based in Aberdeen City and serves a population of nearly 500,000. It covers an area of 6497 km2 (2508 square miles) in North East Scotland. Approximately half of the population lives in an urban area (Aberdeen City) and another half in rural areas (Aberdeenshire). Studies (12, 13) outside the United Kingdom showed that the rate of cataract surgery was lower in rural areas despite a higher prevalence of cataract. However, there was no report comparing preoperative VA between urban and rural areas.
Previous studies have investigated the association between socioeconomic status (SES) and prevalence of cataract (14, 15) and prevalence of cataract surgery (16, 17) but there are no studies on SES and preoperative VA. We therefore investigated whether cataract surgery indication—for example, VA—is different in patients with different socio-economic background. A second goal was to investigate the influence of home location (urban versus rural) in our area as rural populations might have more difficult access to health care service.
Methods
In Aberdeen, new cataract patients are referred from local optometrists. At the cataract clinic, VA, biometry, and complete microscopic examination are performed. The risks and benefits of cataract surgery are discussed at the clinic. Patients with relatively good VA (i.e., 6/5 or 6/6) and who are asymptomatic are not listed for surgery.
The medical notes of 240 consecutive patients who attended the preassessment clinic for cataract operation at Aberdeen Royal Infirmary from January 2010 to March 2010 were reviewed. Demographic data and VA of the operated and fellow eye were recorded. The VA was obtained using the Snellen chart with the patient's best-corrected refraction and converted to decimal values for statistical analysis. Patients with ocular comorbidity (i.e., diabetic retinopathy, glaucoma, maculopathy, retinal detachment [RD], age-related macular degeneration) were excluded from study.
For our first goal, the Scottish Index of Multiple Deprivation (SIMD) was used to determine the SES. Patient's postal code was used to determine the SIMD deprivation rank. The SIMD is the Scottish government's official tool for identifying small area concentrations of deprivation across Scotland, thus enabling effective targeting of policies and funding. It uses 6505 data zones, which are population-based geographic areas with approximately 750 people living in each one. The SIMD ranks these areas from 1, the most deprived, to 6505, the least deprived, providing a ranking for every data zone in Scotland. The overall deprivation score is a weighted sum of 7 domain scores (current income, employment, health, education, geographic access, crime, and housing) derived from 37 different indicators. The SIMD index provides a relative ranking and not an absolute measure of deprivation.
The SIMD ranks were further divided into 5 quintiles; for example, patients in the first quintile rank from 1-1301, representing the 20% most deprived Scottish population. For our second goal, the cohort was divided into urban (Aberdeen City) and rural (Aberdeenshire). The VA was divided into above driving standard (6/12 or better) or below driving standard (worse than 6/12). The association of SIMD ranks on VA was investigated using the chi-square test for trend. Fisher exact test was used to examine the association of geographic variation on VA. Analyses were carried out using SPSS 18.0. All reported p values were based on 2-sided tests and use a significance level of 5%. Analyses were performed using SPSS version 18 (SPSS Inc., Chicago, Illinois, USA). This study was approved by the North of Scotland ethics committee and performed in accordance with the ethical standards of the Declaration of Helsinki.
Results
A total of 240 patients’ case notes were retrospectively reviewed. Fifty-six patients were excluded because of ocular comorbidity, leaving 184 patients for analysis. Of the 56 patients, 23 had glaucoma, 14 had macular degeneration, 12 had diabetic retinopathy, 5 had retina tear or detachment, and 5 had other retina diseases.
Demographics, VA, SIMD ranking quintiles, and geographic classification for those included and excluded are summarized in Table I. Both groups are similar in respect to age, SIMD quintiles distributions, VA, and geographic classification. Of the 184 patients, 72 (39%) had cataract operation on the fellow eye. Among the 127 patients with VA 6/12 or better, 2 (1%) had VA of 6/5, 12 (6.5%) had VA of 6/6, 74 (40%) had VA of 6/9, and 39 (21%) had VA of 6/12.
Demographics, Visual Acuity, Distribution Of Scottish Index Of Multiple Deprivation Scores, And Geographic Classification Of 184 Patients And Those Excluded From The Study (N = 56)
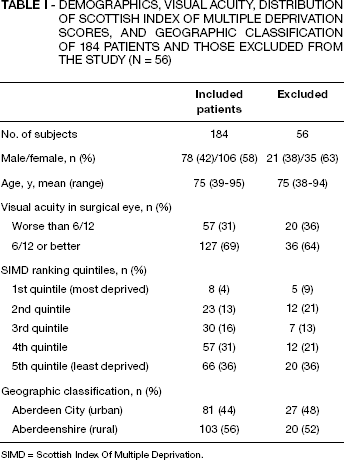
SIMD = Scottish Index Of Multiple Deprivation.
There was a statistically significant trend observed between affluence and VA (χ 2 trend = 4.97, p = 0.03, chi-square test for trend) (Fig. 1), showing more affluent groups tended to have better vision (6/12 or better) prior to cataract operation. Table II compares preoperative VA in urban and rural areas. There was no evidence that geographic region was associated with preoperative VA (p = 0.63, Fisher exact test).

Distribution of patients with visual acuity (VA) of 6/12 or better and worse than 6/12 across quintiles of deprivation. The affluence group tends to have better preoperative VA (χ 2 trend = 4.97, p = 0.03). Quintile of deprivation: 1 = most deprived quintile; 5 = least deprived quintile.
Geographic Location (Urban Versus Rural) And Preoperative Visual Acuity
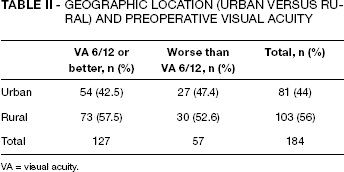
VA = visual acuity.
Discussion
Socioeconomic deprivation has been associated with late presentation and subsequent poor vision and blindness in several eye conditions such as glaucoma (18), amblyopia (19), and diabetic retinopathy (20). In this study, we found a significant association between affluence and good vision (6/12 or better) in the eye scheduled for cataract operation (p = 0.03).
Socioeconomic deprivation is well-known to be associated with higher prevalence of blindness (21), hence more deprived patients tend to present at a later stage of disease. There are several possible explanations for the association between affluence and good vision for cataract surgery observed in this study. First, more deprived groups accept a greater degree of ill health as normal, and are therefore less likely to consult a general practitioner (22) or optometrist. Conversely, people in the higher socioeconomic group consult earlier in their diseases (23). Secondly, the more advantaged groups are better educated and have the ability to articulate needs and possibly have more routine eye tests at community optometrists, where the cataract would have been detected.
Some population-based studies (14, 15) outside the United Kingdom found a “U-shaped” relationship between income and prevalence of cataract surgery, with higher prevalence in the lowest and highest income group. The higher prevalence in the deprived groups was explained by the evidence that low SES is associated with cataract (16, 17). However, high SES was not associated with increased prevalence or progression of cataract. This supports the notion that there was some degree of overutilization of cataract surgery, especially in the high SES groups. This may explain why we found an association between affluence and good vision before cataract surgery. The fact that affluence was associated with good vision in the eye scheduled for surgery is particularly worrisome as the benefit-risk ratio in early cataract surgery remains unknown. Malik et al (10) reported 40% of the patients with VA 6/12 or better listed for cataract surgery had only mild vision-related quality of life impairment and were not dissatisfied with their overall level of vision. Black et al (7) undertook a study to measure the impact of surgery on a representative sample of patients to determine whether or not overutilization of surgery is occurring. They found that 30% of operations would be deemed inappropriate if based on patients’ reported visual function (VF-14) score of just 5.5 higher after surgery. As far as the risk is concerned, the incidence of RD after phacoemulsification ranged from 0.9% to 1.2% (24-26), which is almost 9 times higher than expected in eyes that do not undergo cataract surgery. Interestingly, a population-based study (27) in Scotland found 23% of those with RD had undergone cataract surgery in the past and RD is strongly associated with affluence. Since affluence is associated with both RD (27) and early cataract surgery (in this study), one may speculate that affluent patients may expose themselves to unnecessary risk. However, it is beyond the scope of our study to prove this.
There are several potential limitations in this study. First, SIMD ranks are based on postcode areas rather than on the individual, so the results may be affected by the “ecological fallacy” in which some patients in the affluent areas may actually be of lower SES and vice versa. Secondly, patients from areas of greater deprivation may have poorer access to health care services and were excluded from the study. Third, these data were based on routine NHS hospital statistics. Private cataract surgery data were therefore not included. Furthermore, the grading and types of cataract were not included in the study.
This study did not show an association between geographic location and preoperative VA (p = 0.63), suggesting ophthalmic services are not compromised in rural areas in North East Scotland. This was not consistent with Finnish (12) and Western Australia (13) reports, possibly because of the differences in health care systems. For other specialties, remoteness remains a challenging issue in providing health care. For example, Campbell et al (28) reported that rural residents in Northern Scotland presented with more advanced stage of lung and colorectal cancer. Mackenzie et al (29) found that patients from rural areas had higher rate of symptomatic carotid artery disease but this was not met by increased rate of carotid endarterectomy.
In conclusion, this study showed that affluent patients were more likely to have better VA prior to their cataract operation than those from more deprived postcode areas.