
Abstract
Purpose
To assess the effects of corneal collagen crosslinking (CXL) on Scheimpflug imaging system parameters in patients with progressive keratoconus.
Methods
Forty-seven eyes of 47 patients who underwent CXL treatment (CXL group) for progressive keratoconus and 26 eyes of 26 nontreated patients with keratoconus (control group) were included in this retrospective controlled study. Changes in corrected distance visual acuity (CDVA, logMAR equivalent), maximum K (keratometry), corneal volume (CV), corneal thickness, and anterior chamber parameters including anterior chamber depth (ACD), anterior chamber volume (ACV), and anterior chamber angle (ACA) were analyzed at 6 months follow-up.
Results
The mean CDVA improved (p<0.001); maximum K, CV, and pachymetry measurements significantly decreased after CXL treatment in patients with progressive keratoconus (p = 0.001, p<0.001, respectively). However, in the control group, CDVA, maximum K, CV, and pachymetry measurements remained unchanged at 6 months follow-up (p>0.05). The anterior chamber parameters (ACD, ACV, and ACA) did not show significant changes between baseline and 6 months in CXL and control groups (p>0.05).
Conclusions
In patients with progressive keratoconus, CXL treatment is effective in improving visual acuity and maximum keratometry. Although the treatment might cause corneal thinning and volume loss, anterior chamber parameters seem not to be affected during the postoperative course.
Keywords
Introduction
Keratoconus is a noninflammatory progressive disease characterized by abnormal thinning and steepening of the cornea (1). Increased proteolytic enzyme activities, decreased concentration of protease inhibitors, and altered configuration of the stromal collagen lamellae play a role in the pathogenesis (2, 3). Wollensak et al (4) have introduced corneal collagen crosslinking (CXL) using riboflavin and ultraviolet A (UVA) as a new therapeutic option for keratoconus. Recent studies concluded that CXL enhances the biomechanical stability of the cornea and arrests the progression of keratoconus by inducing the formation of new covalent crosslinks between collagen fibrils (5-7). Visual and refractive improvements after CXL treatment have been demonstrated in many studies (8-10). However, to our knowledge, changes in anterior chamber measurements after CXL have not been reported.
Computer-assisted corneal topography devices are valuable for the diagnosis and follow-up of keratoconus. A recently introduced imaging device uses 360° rotating Scheimpflug camera and provides accurate measurements of anterior segment structures (11). In this retrospective controlled study, we aimed to assess the changes in anterior chamber parameters (anterior chamber depth, anterior chamber volume, and anterior chamber angle) and corneal parameters (maximum keratometry, corneal volume [CV], and corneal pachymetry) after CXL treatment in patients with keratoconus using Scheimpflug imaging system.
Methods
Forty-seven eyes of 47 patients who underwent CXL treatment for progressive keratoconus (CXL group) and 26 eyes of 26 age- and sex-matched nontreated patients with keratoconus (control group) were included in this retrospective study. In bilateral cases, eyes with more advanced stage of keratoconus were selected for statistical analysis. The study was performed in adherence to the tenets of the Declaration of Helsinki and the local ethics committee approved the methodology. Written informed consent was obtained. Patients were enrolled in the study according to the following criteria: corneal topography pattern consistent with keratoconus, at least 15 years of age, thinnest corneal pachymetry of ≥400 μm, and no history of corneal scarring or surgery. All patients underwent detailed ophthalmologic examinations included corrected (including contact lens) distance visual acuity (CDVA) measurement with Snellen charts, slit-lamp biomicroscopic examination, applanation tonometry, and dilated funduscopic examination using +90 D noncontact lens. Progressive keratoconus was defined as ≥1 D steepening of maximum keratometry or an increase of ≥1.00 D in manifest cylinder or an increase of ≥0.50 D in manifest refraction spherical equivalent in 2 years.
Corneal collagen crosslinking procedure was performed under sterile conditions using topical anesthesia as described by Wollensak et al (4). Central 9.0 mm corneal epithelium was removed by mechanical debridement. Riboflavin solution (0.1% in 20% dextran T500 solution, Medio Cross, Medio-Haus Medizinprodukte GmbH, Germany) was instilled every 2 minutes for 30 minutes. Riboflavin absorption was observed under biomicroscopic examination. Then the cornea was exposed to UVA irradiation at the wavelength of 365 nm and surface irradiance of 3 mW/cm2 (Opto XLink Corneal Cross-linking System 1.0, Opto Electronica S/A, SP Brazil). During the UVA exposure, isotonic riboflavin solution instillation was continued every 2 minutes for 30 minutes. Postoperatively, a soft contact lens was placed until corneal reepithelialization completed. Topical antibiotic and corticosteroid drops were administered after CXL treatment and continued 4 times daily for 1 week and 2 weeks, respectively. Scheimpflug ocular imaging (Oculus Pentacam, Oculus Optikgerate GmbH, Germany) was conducted with undilated pupils under scotopic conditions by a single experienced technician (SV). Scans were taken in automatic mode with proper quality. Anterior chamber depth (ACD, distance from the corneal endothelium to the anterior lens surface with undilated pupil along the optical axis), anterior chamber volume (ACV, calculated from the corneal endothelium to the anterior lens surface with undilated pupil in a 12-mm diameter around the corneal apex), anterior chamber angle (ACA), CV (calculated within diameter of 10 mm, centered on the corneal apex with the anterior and posterior cornea defining the boundaries), pupil center pachymetry, apical pachymetry, thinnest pachymetry, and maximum K values were obtained for each eye.
Visual acuity in Snellen format was converted to the logMAR equivalent and then mean visual acuity was calculated (12). The changes in mean CDVA, maximum K, and Scheimpflug imaging system measurements were evaluated in both groups at 6 months follow-up. Postoperative changes in the CXL group were compared with those of the nontreated controls at the same periods.
Statistical analysis was performed with the Statistical Package for Social Sciences software version 10.0.1 (SPSS Inc., Japan). Demographic and descriptive data were expressed as mean ± SD. Two related samples test (Wilcoxon signed ranks test) was used to analyze the changes in quantitative data (mean CDVA and Scheimpflug measurements) between baseline and 6 months. Comparison of the quantitative data (changes in mean CDVA and Scheimpflug measurements) between the CXL group and the control group was performed by Mann-Whitney U test. The χ 2 test was used to analyze differences in sex between groups. Spearman correlation coefficients were used to determine correlations among the changes in mean CDVA, maximum K, and Scheimpflug system parameters. At 95% confidence interval, a p value less than 0.05 was considered statistically significant.
Results
Forty-seven eyes of 47 patients had CXL treatment for progressive keratoconus (CXL group) and 26 eyes of 26 patients with keratoconus did not have any surgical treatment (control group). The CXL group consisted of 20 men and 27 women with a mean age of 28.7 ± 9.0 years and the control group comprised 15 men and 11 women with a mean age of 29.1 ± 6.9 years (p>0.05). All patients had at least 6 months follow-up.
The mean CDVA significantly improved and maximum K value significantly decreased after CXL treatment (p<0.001, p = 0.001, respectively) (Tab. I). However, in the control group, change in mean CDVA and maximum K was not statistically significant at 6 months control (p>0.05) (Tab. I). In the CXL group, improvements in CDVA and maximum K were statistically significant compared with those of the control group (p<0.001) (Tab. I).
Changes In Mean Cdva And Maximum Keratometry Over Time, And Comparison Of These Changes Between Groups
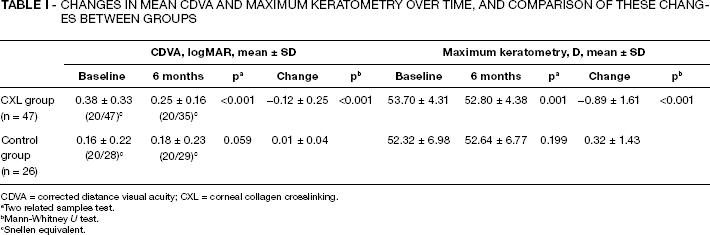
CDVA = corrected distance visual acuity; CXL = corneal collagen crosslinking.
Two related samples test.
Mann-Whitney U test.
Snellen equivalent.
The mean ACD, ACV, and ACA parameters did not change between baseline and 6 months in both CXL and control groups (p>0.05) (Tab. II). Furthermore, there were no significant differences between CXL and the control groups regarding the changes in anterior chamber measurements (p>0.05).
Changes In Anterior Chamber Parameters Between Baseline And 6 Months In The Cxl And Control Groups
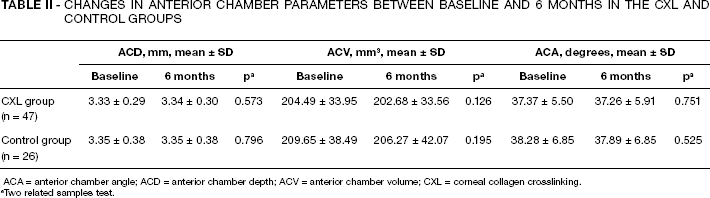
ACA = anterior chamber angle; ACD = anterior chamber depth; ACV = anterior chamber volume; CXL = corneal collagen crosslinking.
Two related samples test.
In the CXL group, the mean CV was significantly decreased from 56.84 ± 3.95 mm3 baseline to 55.79 ± 3.78 mm3 at 6 months (mean change 1.05 ± 1.59 mm3, p<0.001). Moreover, pupil center pachymetry, apical pachymetry, and thinnest pachymetry values significantly decreased between baseline and 6 months after CXL (p<0.001) (Tab. III). However, the changes in pachymetry measurements from baseline were not statistically significant in the control group (p>0.05) (Tab. III). The decreases in CV and all pachymetric measurements in the CXL group were significant compared with those of the control group (p = 0.010, p<0.001, respectively). Correlation analyses were performed to determine the relations between the Scheimpflug system parameters and clinical outcomes of the CXL treatment. In the CXL group, we found significant positive correlations between the changes in corneal thicknesses (pupil center, apex, and thinnest pachymetry) and the change in maximum K value (r = 0.462, p = 0.001; r = 0.535, p<0.001; r = 0.445, p = 0.002, respectively), although correlations between the changes in corneal thicknesses and the change in CDVA were not statistically significant (p>0.05). Moreover, anterior chamber parameters and CV did not show significant correlations with the improvements in CDVA and maximum K value (p>0.05).
Changes In Pachymetry Measurements Between Baseline And 6 Months In The Cxl And Control Groups
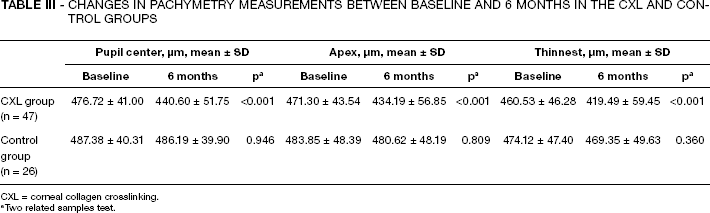
CXL = corneal collagen crosslinking.
Two related samples test.
Anterior segment slit-lamp biomicroscopy findings were unremarkable during the 6 months follow-up except for CXL-related corneal haze in all treated patients that resolved about 3 months after treatment.
Discussion
Corneal collagen crosslinking is a new procedure that was shown to arrest progression of keratoconus due to change in biomechanical strength of the cornea (4-7). Visual and refractive improvements reveal the efficacy of CXL treatment (8–10, 13). In this retrospective controlled study, we assessed changes in Scheimpflug anterior chamber parameters (ACD, ACV, and ACA) and corneal parameters (maximum K, CV, and corneal pachymetry) after 6 months from CXL treatment in patients with progressive keratoconus. To our knowledge, effects of CXL treatment on anterior chamber parameters have not been reported previously. In the current study, mean ACD, ACV, and ACA values did not show significant change from baseline at 6 months after CXL treatment. This finding may indicate stability of the anterior chamber parameters after CXL treatment, whereas this idea needs to be supported with long-term studies. Corneal collagen crosslinking induces a structural remodeling process that leads to pachymetric and volumetric alterations in the cornea (14-16). In this study, mean CV and corneal thickness were found significantly decreased between baseline and 6 months after CXL, although there were no significant changes in terms of CV and corneal thickness in the control group. Similarly, Vinciguerra et al reported a significant decrease in CV and pupil center pachymetry in keratoconus patients and a significant decrease in CV, pupil center pachymetry, and thinnest pachymetry in eyes with corneal ectasia at 1 year from CXL (16, 17).
In a prospective study, Greenstein et al (18) found all pachymetry measurements significantly thinned at 1 month and 3 months, although only thinnest pachymetry remained thinner than preoperatively at 1 year after CXL treatment. They also suggested that CXL-associated corneal haze density was significantly decreased between 3 months and 12 months, which was parallel with the time course of corneal thinning and rethickening (18, 19). In our study, all CXL-treated eyes developed anterior stromal corneal haze. Although corneal haze resolved about 3 months postoperatively, the cornea was still thinner from baseline at 6 months. Change in corneal transparency and enhanced density of stromal fibers after CXL treatment could interfere with light and cause an artificial wrong measurement of corneal thickness with Scheimpflug method. However, previous studies showed that Scheimpflug pachymetry measurements were reliable, repeatable, and comparable to ultrasonic pachymetry in keratoconic corneas (20, 21). Moreover, pachymetry measurements obtained from Scheimpflug system were found to be similar with ultrasonic pachymetry measurements in eyes with corneal haze after myopic photorefractive keratectomy (22).
Corneal thinning and rethickening process after CXL treatment was also demonstrated in the study of Arbelaez et al (23). In contrast to our study, Grewal et al (24) and Coskunseven et al (25) found no significant change regarding central corneal thickness at 1 year control. These results suggest that cornea initially thins after CXL and rethickening process continues over months postoperatively.
Several confocal microscopic and experimental studies demonstrated early keratocyte apoptosis and progressively increased keratocyte repopulation accompanied with enhanced density of stromal fibers, which was approximately completed at 6 months after CXL (26-28). Furthermore, reorganization of the collagen lamella continues over years (28). Early and late postoperative rearrangements of the corneal microstructure may explain the differences in pachymetry measurements at different time points of postoperative course as in the above mentioned studies. In our study, significant corneal thinning may be considered as a result of early postoperative corneal tissue loss and accompanying CV reduction supports this idea. Persistent corneal thinning at 6 months in our study might be due to limited follow-up.
In the current study, we also assessed the relations between Scheimpflug parameters and clinical outcomes of CXL treatment. The changes in Scheimpflug parameters between baseline and 6 months were not correlated with the improvement in visual acuity after CXL, although corneal thinning was correlated with the decrease in maximum K. In contrast to our study, Greenstein et al (18) found negative correlation between corneal thinning (baseline–3 months) and improvement in max K at 1 year, although time points of the measurements were different from our study. We suggest that after CXL, cornea significantly thins with an improvement in maximum keratometry, and this finding might be an important indicator of complicated corneal healing process after CXL.
In conclusion, our study demonstrated relatively short-term effects of CXL treatment on visual acuity, maximum K, CV, corneal thickness, and anterior chamber parameters. Corneal collagen crosslinking induces a complicated long-term corneal healing and remodeling process. Underlying mechanisms and long-term effects of CXL treatment on anterior segment parameters should be investigated.