
Abstract
Purpose
To evaluate choroidal thickness in highly myopic eyes with choroidal neovascularization (CNV), 3 or more years after treatment with photodynamic therapy (PDT), intravitreal ranibizumab (IVR), or both (PDT + IVR).
Methods
The medical records of patients with high myopia and CNV treated with PDT or IVR in our department were reviewed. Eyes meeting the inclusion criteria were assigned to 3 groups: PDT, IVR, and PDT + IVR. A fourth group, “dry myopic maculopathy,” included the contralateral highly myopic eyes that never developed CNV. All patients performed a cross-sectional evaluation with best-corrected visual acuity (BCVA), measurement of axial length, color fundus photography, and enhanced depth imaging with spectral domain optical coherence tomography.
Results
Forty-two eyes (21 patients) were included: 11 eyes (26.2%) in the PDT group, 8 (19.0%) in the IVR group, 9 (21.4%) in the PDT + IVR group, and 14 (33.3%) in the dry maculopathy group. Subfoveal choroidal thickness showed no significant differences between groups (p>0.05). Positive correlation was found between BCVA and macular choroidal thickness (r = +0.293, p<0.001). Regression analysis showed that age (p<0.001), axial length (p<0.001), sex (p = 0.001), and myopic lesions such as tessellated fundus (p = 0.046) and patchy atrophy (p = 0.008) were predictive of choroidal thickness. Type of treatment was not predictive of choroidal thickness.
Conclusions
Older age and greater axial length are the major factors associated with macular choroidal thinning in highly myopic eyes submitted to CNV treatment. The type of treatment performed for myopic CNV had no predictive contribution for choroidal thickness.
Keywords
Introduction
Myopic degeneration is a leading cause of visual impairment in many parts of the world (1-4). It is associated with excessive and progressive elongation of the globe, resulting in a variety of fundus changes that lead to visual impairment, including choroidal neovascularization (CNV) and chorioretinal atrophy (5-11). Chorioretinal atrophy, secondary or not to myopic CNV, results in photoreceptor cell death and thus to irreversible loss of central visual function (12, 13). The underlying mechanisms and pathologic course, however, are not well understood, especially at the choroidal level (14). Previous histologic studies have already shown choroidal thinning, with lack of vessels in some areas and pronounced thinning of the choriocapillaris in others. Replacement of the normal choroidal structure with fibrous tissue is common (15, 16).
Enhanced depth imaging (EDI) spectral domain optical coherence tomography (SD-OCT) has been recently developed and enables in vivo cross-sectional imaging of the choroid (17). Recent reports showed successful examination and measurement of choroidal thickness in normal and pathologic eyes using SD-OCT and also using high-penetration OCT (18-26).
Fujiwara et al (16) reported that the choroid in highly myopic eyes is thinner than in normal eyes. Ikuno and Tano (14) also reported that the choroid undergoes further thinning with age and degree of myopia. Choroidal thickness evaluation by EDI OCT is therefore an interesting approach to evaluate in vivo the pathophysiologic changes of the choroid in highly myopic eyes. The morphologic and functional prognosis was addressed in a few studies (27, 28), and the impact of different treatment strategies for myopic CNV in choroidal thickness has not been studied. Therefore, the purpose of this study is to evaluate macular choroidal thickness in pathologic myopic eyes without CNV or with CNV submitted to different treatment modalities, and its relation to visual acuity and myopic maculopathy phenotype (29).
Materials and Methods
This was a retrospective study conducted at the Ophthalmology Department of Centro Hospitalar e Universitário de Coimbra and at the Association for Innovation and Biomedical Research on Light and Image (AIBILI). Written informed consent was obtained from all subjects and the study was conducted in accordance with the tenets of the Declaration of Helsinki and after institutional review board approval.
The medical records of consecutive patients with pathologic myopia followed in our department were examined. The inclusion criteria were 1) highly myopic eyes, defined as having a spherical equivalent refractive error equal to or more negative than −6.00 D and/or axial length (AL) equal or superior to 26.0 mm; 2) CNV treated with photodynamic therapy (PDT) and/or intravitreal ranibizumab (IVR) without other previous treatments; 3) contralateral highly myopic eyes that never developed CNV; 4) minimum follow-up of 3 years. The exclusion criteria included history of amblyopia, glaucoma, uveitis, dense cataract, diabetic retinopathy, retinal vascular abnormalities, laser treatment, intravitreous injection of triamcinolone, previous vitrectomy, and scleral buckling procedure.
Eyes with history of myopic CNV meeting the inclusion criteria were assigned to 3 groups according to treatment received during follow-up: PDT, IVR, and PDT + IVR. The kind of treatment used for myopic CNV was determined as follows: after PDT approval for the treatment of myopic CNV this was the standard treatment used in our department (PDT group); however, after IVR approval in the treatment of CNV secondary to age-related macular degeneration, new cases of myopic CNV were always treated with IVR in spite being an off-label use (IVR group). Eyes with myopic CNV with poor response to PDT were also switched to IVR during follow-up (PDT + IVR group). Both treatments were never performed simultaneously during follow-up. A fourth group, dry myopic maculopathy, included the contralateral highly myopic eyes without history of CNV, which never required any treatment.
In addition to patient demographics, the initial best-corrected visual acuity (BCVA) with Early Treatment of Diabetic Retinopathy Study (ETDRS) charts recorded before starting treatment and complete history of the following procedures was recorded from medical records: PDT, IVR, cataract surgery, and refractive surgery.
A cross-sectional evaluation was performed in all patients including BCVA (ETDRS charts), slit-lamp examination, and dilated fundus stereoscopic examination with +90 D and +60 D lenses. In phakic patients with no prior refractive surgery, the most recent manifest refraction was recorded. The manifest refraction in patients who had prior cataract or refractive surgery was excluded. Measurement of AL was performed in all patients with Biograph Allegro® (WaveLight AG, Erlangen, Germany) or by A-scan ultrasonography (OcuScan® RxP, Alcon, California, USA), if the previous failed. Color fundus photography and SD-OCT with Spectralis OCT (Heidelberg Engineering, Heidelberg, Germany) in choroidal mode (EDI OCT) were performed in order to classify the myopic maculopathy and to measure choroidal thickness.
Classification of myopic maculopathy in the color fundus photographs was made by 2 of the authors (C.L.F., R.M.S.) independently, and in accordance to the progression pattern proposed by Hayashi et al (29): tessellated fundus, diffuse chorioretinal atrophy, patchy chorioretinal atrophy, presence of lacquer cracks, active CNV, and macular atrophy. Tessellated fundus was defined as the condition in which the choroidal vessels could be visualized through the retina, as a result of the hypoplastic retinal pigment epithelium (RPE) (30). Diffuse chorioretinal atrophy appears as a more yellowish-white posterior fundus, because of the greater atrophy of the RPE. The patchy chorioretinal atrophy consists of a grayish-white, well-defined lesion (31). Macular atrophy was defined as the area of chorioretinal atrophy that developed around a myopic CNV, and was determined by the visibility of the sclera in color fundus photography (32) (Fig. 1). In cases of disagreement, the color fundus photographs were assessed jointly until a consensus was reached.
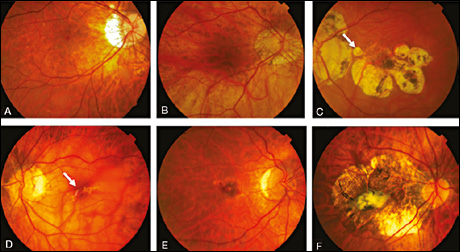
Color fundus photographs representing different types of myopic maculopathy, according to Hayashi et al. (A) Tessellated fundus, OD. (B) Diffuse chorioretinal atrophy, OD. (C) Patchy chorioretinal atrophy (arrow), OS. (D) Lacquer cracks (arrow), OS. (E) Active choroidal neovascularization, with macular hemorrhage, OD. (F) Extensive macular atrophy, OD.
To measure choroidal thickness we performed EDI OCT with Spectralis OCT (Heidelberg Engineering, Heidelberg, Germany) in all patients. The method of obtaining EDI OCT images and choroidal thickness measurements was performed as previously reported (16-18). Briefly, the choroid was imaged in the choroidal mode with the SD-OCT system. In the choroidal mode the signal from the retinochoroidal portion of the scanned region is enhanced relative to that in the vitreoretinal portion. Both the horizontal and vertical sections passing through the center of the fovea were used for the choroidal thickness measurements. The choroidal thickness was defined as the distance from the outer border of the hyperreflective line corresponding to the RPE to the inner scleral border. Choroidal thickness measurements were obtained manually under the fovea using the scale supplied with the software and at 1,000 μm intervals from the fovea to 3 mm in the nasal, temporal, superior, and inferior directions (Fig. 2). Each image was measured by 2 independent observers (C.L.F., A.S.B.). Data with discrepancies of 15% were reanalyzed by the senior author (R.M.S.). The value averaged from the 13 choroidal thickness readings was considered to be the macular choroidal thickness. The value of the central reading was considered the subfoveal choroidal thickness. The type of myopic maculopathy found in each reading point was also recorded.
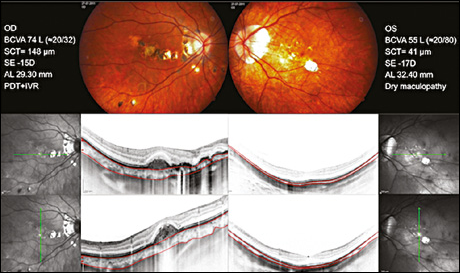
Both the horizontal and vertical sections passing through the center of the fovea were used for choroidal thickness measurement as seen in this 25-year-old man. AL = axial length; BCVA = best-corrected visual acuity; IVR = intravitreal ranibizumab; PDT = photodynamic therapy; SCT = subfoveal thickness; SE = spherical equivalent.
Statistical analyses were performed using Stata software version 12.0 (StataCorp LP). Data were presented descriptively and analyzed statistically. First univariate analyses were performed to identify statistically significant results. To test for statistically significant differences between independent groups, the Mann-Whitney test was used; to test statistically significant differences between paired groups, the Wilcoxon test was used. Correlations between parameters were tested using the Spearman correlation coefficient. To identify predictive parameters for choroidal thickness and visual acuity, a multivariate analysis was performed using regression analyses (median and interquartile regression analyses).
Results
Patient demographic data
Forty-two consecutive eyes from 21 patients, 8 male and 13 female, with a mean age of 54.2 ± 15.0 years (range 25–84) were included. Eleven eyes (26.2%) were included in the PDT group, 8 (19.0%) in the IVR group, 9 (21.4%) in the PDT + IVR group, and 14 (33.3%) in the dry maculopathy group. Mean age, follow-up, initial and final BCVA, refractive error, AL, the type and number of treatments, subfoveal and macular choroidal thickness of all eyes and for each group are presented in Table I. Age was not statistically different between groups (p>0.05). Axial length, however, was superior in the PDT group, and this was statistically significant when compared to the other 3 groups (IVR, p = 0.025; PDT + IVR, p = 0.018; dry maculopathy, p = 0.027). There were no other significant differences in AL between groups.
Summary Of Clinical Data Of All Eyes And By Group
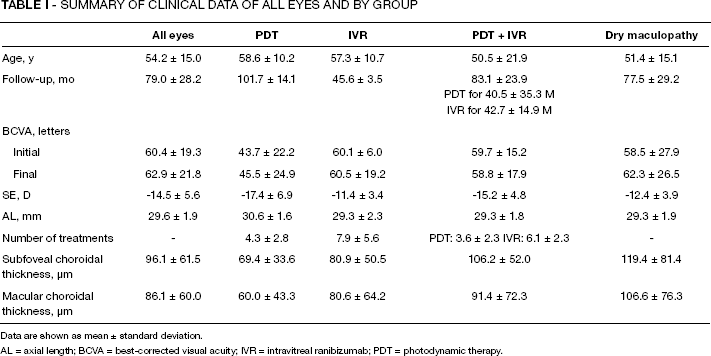
Data are shown as mean ± standard deviation.
AL = axial length; BCVA = best-corrected visual acuity; IVR = intravitreal ranibizumab; PDT = photodynamic therapy.
Ten eyes (23.8%) were pseudophakic (2 in the PDT group, 3 in the IVR group, 2 in the PDT + IVR group, and 3 in the dry maculopathy group), 1 eye (2.4%) in the dry maculopathy group was aphakic, and 4 eyes (9.5%) of 2 patients were submitted previously to refractive surgery (2 in the PDT + IVR group, 1 in the IVR group, and 1 in the dry maculopathy group). The main myopic retinal complications found on OCT (excluding CNV) are presented in Table II.
Main Associated Pathologic Features Found In Oct
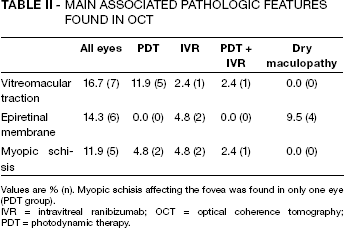
Values are % (n). Myopic schisis affecting the fovea was found in only one eye (PDT group).
IVR = intravitreal ranibizumab; OCT = optical coherence tomography; PDT = photodynamic therapy.
Choroidal thickness analysis
All mean choroidal thickness readings recorded are presented in detail in Table III. Globally, the nasal and inferior choroid was thinner than the temporal and superior choroid. The choroidal thickness increased in the inferior to superior direction, and in the nasal to temporal direction. However, the mean subfoveal thickness was greater than the temporal reading 1 mm away. There was a statistically significant difference between the subfoveal choroidal thickness and the 1 mm nasal and inferior choroidal thickness readings (p<0.05). The choroid in areas of peripapillary atrophy was exceedingly thin or not visualizable and the choroid in areas adjacent to the peripapillary atrophy was markedly thin. When each group was considered separately, we found that the same pattern was present in nearly all groups (Figs. 3 and 4). Eyes in the dry maculopathy group had thicker choroids compared to eyes that developed CNV from any of the treatment groups. However, no statistically significant differences in choroidal thickness were found when evaluating the same reading points, including subfoveal choroidal thickness (p>0.05). When considering only treatment groups, we also found that eyes treated with PDT almost always had the thinnest choroidal thickness values, while eyes in the PDT + IVR group had the highest choroidal thickness values. Again, there were no statistically significant differences in choroidal thickness between treatment groups for the 13 reading points, including subfoveal thickness (p>0.05).
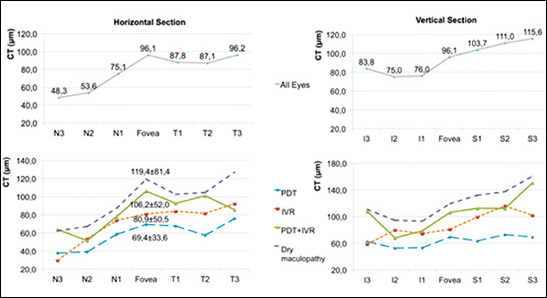
Choroidal thickness (CT) in all eyes (top row) and by group (bottom row), horizontal and vertical sections. I1-3 = 1–3 mm inferior to fovea; IVR = intravitreal ranibizumab; N1-3 = 1–3 mm nasal; PDT = photodynamic therapy; S1-3 = 1–3 mm superior; T1-3 = 1–3 mm temporal.
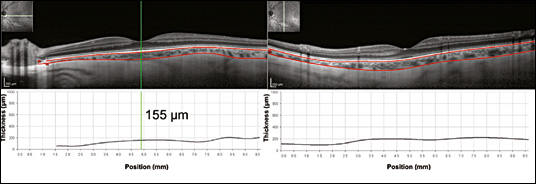
Horizontal and vertical sections showing choroidal thickness increasing in the nasal to temporal direction and in the inferior to superior direction. Left eye of a 49-year-old woman, best-corrected visual acuity of 82 L (≍20/25), spherical equivalent of −6.75 D, axial length of 26.29 mm, subfoveal thickness of 155 μm, dry maculopathy group.
Mean Choroidal Thickness Of All Eyes And By Group (μM)
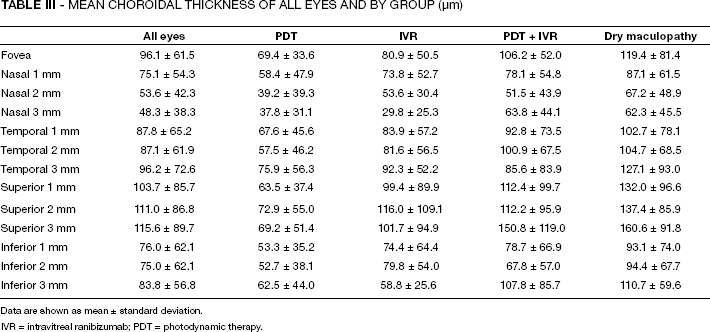
Data are shown as mean ± standard deviation.
IVR = intravitreal ranibizumab; PDT = photodynamic therapy.
Macular choroidal thickness (average from the 13 choroidal thickness readings taken in each eye) was 60.0 ± 43.3 μm in the PDT group, 80.6 ± 64.2 μm in the IVR group, 91.4 ± 72.3 μm in the PDT + IVR group, and 106.6 ± 76.3 μm in the dry maculopathy group (mean ± SD). When comparing macular choroidal thickness between groups, a statistically significant difference was found between the PDT group and the IVR (p = 0.025), PDT + IVR (p = 0.005), and dry maculopathy (p<0.001) groups. The difference in macular choroidal thickness was not significant between the IVR and PDT + IVR groups (p = 0.452). Macular choroidal thickness in the dry maculopathy group was the thickest, and besides PDT, the difference was significant compared to the IVR group (p = 0.009), but not for PDT + IVR (p = 0.077) (Fig. 5).
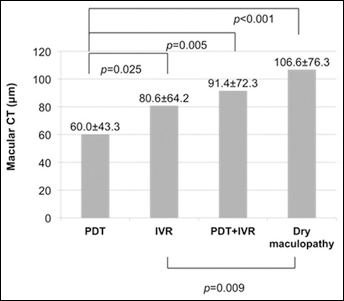
Macular choroidal thickness (CT) by group. Statistically significant differences between groups are presented (p<0.05). IVR = intravitreal ranibizumab; PDT = photodynamic therapy.
BCVA and choroidal thickness
A positive and moderate correlation between subfoveal choroidal thickness and the initial and final BCVA was found in the dry maculopathy group (r = 0.526, p<0.05, and r = 0.599, p<0.05, respectively), but not in any one of the treatment groups.
Macular choroidal thickness was directly but weakly correlated with both initial and final BCVA, when considering all eyes together (r = 0.261, p<0.001, and r = 0.293, p<0.001, respectively). In the dry maculopathy group, a positive and moderate correlation between macular choroidal thickness and the initial and final BCVA was also found (r = 0.557, p<0.001, and r = 0.533, p<0.001, respectively). In the remaining groups, the correlation was weak (PDT and IVR) or absent (PDT + IVR).
Type of myopic lesions and choroidal thickness
Myopic maculopathy fundus lesion frequency by group is presented in Table IV. Considering all eyes, the tessellated fundus had the thickest choroid readings (mean ± SD 194.3 ± 57.0 μm), followed by macular atrophy (82.0 ± 55.8 μm), diffuse chorioretinal atrophy (70.3 ± 49.1 μm), and patchy chorioretinal atrophy (36.2 ± 30.0 μm). Choroidal thickness of tessellated fundus was statistically different from diffuse chorioretinal atrophy, patchy chorioretinal atrophy, and macular atrophy (p<0.001). Choroidal thickness of patchy chorioretinal atrophy was the thinnest, and this was statistically significant compared to choroidal thickness of tessellated fundus, diffuse chorioretinal atrophy, and macular atrophy (p<0.001). Choroidal thickness of macular atrophy was not statistically different from choroidal thickness of diffuse atrophy (Fig. 6). Differences in choroidal thickness by group are presented in Table V.
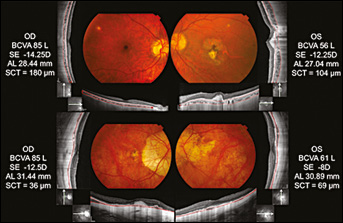
Choroidal thickness and myopic maculopathy. Top row: 31-year-old woman. OD, tessellated fundus, dry maculopathy group; OS, macular atrophy and tessellated fundus, photodynamic therapy (PDT) + intravitreal ranibizumab (IVR) group. Bottom row: 72-year-old man. OD, diffuse atrophy and macular atrophy, PDT + IVR group; OS, diffuse atrophy, dry maculopathy group. AL = axial length; BCVA = best-corrected visual acuity; SCT = subfoveal thickness.
Myopic Maculopathy Fundus Lesion Frequency By Group
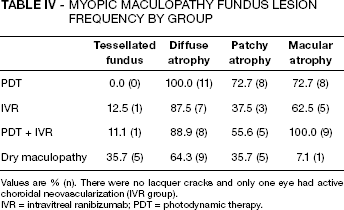
Values are % (n). There were no lacquer cracks and only one eye had active choroidal neovascularization (IVR group).
IVR = intravitreal ranibizumab; PDT = photodynamic therapy.
Differences In Choroidal Thickness Between Different Types Of Myopic Maculopathy, By Group
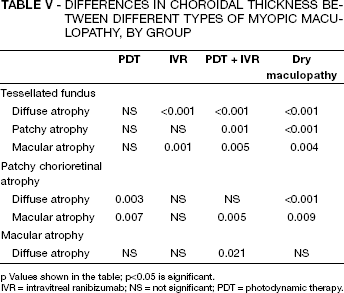
p Values shown in the table; p<0.05 is significant.
IVR = intravitreal ranibizumab; NS = not significant; PDT = photodynamic therapy.
Regression analysis was performed to identify the predictive variables of choroidal thickness from among age, sex, AL, type of myopic maculopathy, and kind of treatment used for myopic CNV (PDT, IVR, and PDT + IVR). For this purpose, we used median regression analysis and interquartile regression analysis. The following parameters showed a predictive value for the choroidal thickness: age (p<0.001) and AL (p<0.001), both with negative contribution; sex (p = 0.001) was also predictive, with male sex associated with higher choroidal thickness; peripapillary atrophy (p = 0.005), with negative contribution; as for the type of myopic maculopathy, only tessellated fundus (p = 0.046) and patchy chorioretinal atrophy (p = 0.008) were predictive of choroidal thickness, with positive and negative contributions, respectively. The interquartile model identified only age as a predictive parameter (p = 0.048). None of the treatments used for myopic CNV showed predictive value for choroidal thickness, and therefore type of treatment used had no impact on choroidal thickness.
We also performed regression analysis to identify the predictive variables for final BCVA from among subfoveal choroidal thickness, age, sex, AL, type of myopic maculopathy, and kind of treatment used for myopic CNV. The following parameters showed a predictive value for the final visual acuity: sex (p = 0.018) (with men having lower BCVA) and AL (p = 0.001) with a negative contribution. However, the mean AL was significantly superior in men, 30.0 ± 1.8 mm (15 eyes in men), when compared with women, 29.4 ± 1.9 mm (27 eyes in women) (p<0.001). The interquartile model identifies only AL as a predictive parameter (p = 0.002) for BCVA. Subfoveal choroidal thickness was not a predictor of BCVA in any of the models used for regression analysis. Also and importantly, the kind of treatment used for myopic CNV had no predictive value for final BCVA.
Discussion
Our study shows that the choroidal thickness of highly myopic eyes without CNV or after treatment for myopic CNV depends essentially on age and AL. Importantly, we also found that different myopic maculopathy phenotypes presented with significant differences in choroidal thickness and that the type of treatment used for myopic CNV had no influence on choroidal thickness.
Recent studies evaluating choroidal thickness in highly myopic eyes by means of EDI OCT showed that the choroid of highly myopic eyes is very thin, and this is significant when compared with normal eyes (14, 16, 18). In our study we also found very thin choroids associated with high myopia and with the same thickness pattern reported by Fujiwara et al (16): choroidal thickness was greatest 3 mm temporal to the fovea and decreased nasally, reaching a minimum 3 mm nasal to the fovea. However, and in contrast, we did not find a depression in subfoveal choroidal thickness as reported by them in their subgroup analysis of eyes with history of CNV. Our results are more in line with their non-CNV group. We also completed macular choroidal thickness analysis with a vertical macular meridian on EDI OCT, and we found that the choroid also increases in the inferior to superior direction. This also confirms previous reports (28).
Eyes in the dry maculopathy group had thicker choroids than the eyes in treatment groups (PDT, IVR, and PDT + IVR). Therefore, eyes with a history of treated CNV had thinner choroids compared with eyes that never developed CNV. This was in accordance with previous studies (16). Although the differences between choroidal thickness reading points, including subfoveal, were not statistically different between the dry maculopathy group and treatment groups, we found a significant difference when macular choroidal thickness was considered and compared between groups. In fact, the difference in macular choroidal thickness between dry maculopathy and PDT and IVR groups was significant. It is known that choroidal thickness in high myopia undergoes further attenuation with increasing age and degree of myopia (16). Recent studies also demonstrated that age, refractive error, and AL correlated significantly with subfoveal or macular choroidal thickness in highly myopic eyes without history of CNV (14, 27, 28, 33). In this study we also found by regression analysis that age and AL were strong predictors of choroidal thickness, with negative predictive value. This helps to explain why eyes in the dry maculopathy group had higher choroidal thickness readings, as patients in this group were younger (although not significantly) than patients in the PDT and IVR groups. Also, and perhaps most importantly, we found that eyes in the dry maculopathy group had the highest prevalence of tessellated fundus, which was identified as a predictive parameter of higher choroidal thickness in regression analysis.
When comparing between treatment groups, we found that eyes in the PDT group presented with the thinnest choroids, both subfoveal and macular, while PDT + IVR eyes had the thickest. Although the difference in subfoveal choroidal thickness was not statistically different among the 4 groups, when the macular choroidal thickness was considered, a significant difference was found between the PDT group and the other 3 groups. Photodynamic therapy accelerates thrombosis and it has been reported that it causes changes in the choroidal filling pattern, which often persisted as long as 16.5 months after PDT (34). It was also suggested that the damage induced by PDT on the surrounding choroid may be more severe in highly myopic eyes, which have thinner retinas and choroids than nonmyopic eyes, thereby promoting atrophic changes in the choroid (34). However, the reason for these results is probably once again related to the predictive factors for choroidal thickness found in regression analysis: first, the patients in the PDT group were older than patients in the remaining groups, and age was found to have a negative predictive value for choroidal thickness; however, mean age was not statistically different between groups; secondly, the mean AL in the PDT group was statistically superior to the mean AL of all other groups, and AL was shown to be a negative predictor of choroidal thickness. Importantly and for the first time, this study also demonstrates that none of the treatments used for myopic CNV (PDT, IVR, and PDT + IVR) had a predictive value for choroidal thickness. Therefore, the low thickness choroidal readings obtained for the PDT group were probably more related to the demographic characteristics of the sample rather than the treatment per se. Therefore, one important conclusion of this study is that PDT and/or IVR treatments are not related to and do not accelerate the progression of macular choroidal thinning associated with advanced high myopia in the long term.
Some studies have demonstrated that visual acuity seems to be correlated with subfoveal and macular choroidal thickness in highly myopic eyes. Fujiwara and coworkers reported a positive correlation between BCVA and subfoveal choroidal thickness in eyes with and without history of myopic CNV (16). Wang et al found a correlation between BCVA and macular choroidal thickness (not subfoveal choroidal thickness) but only in eyes with diffuse chorioretinal atrophy without CNV, and not in eyes with tessellated fundus (28). Their explanation is that eyes may have reduced visual acuity because of development of lacquer cracks or when compromised choroidal circulation failed to maintain physiologic demands of the RPE and outer retina in more advanced stages of pathologic myopia without CNV. More recently, Nishida et al (27) also reported a positive correlation between BCVA and subfoveal choroidal thickness in eyes without myopic CNV. In our study, we also demonstrated a positive and moderate correlation between subfoveal choroidal thickness and both initial and final BCVA in eyes without history of myopic CNV, the dry maculopathy group. This correlation was stronger in our study than in these previous reports. However, no correlation was found for subfoveal choroidal thickness and BCVA in the 3 treatment groups, which included only eyes with history of CNV. As for macular choroidal thickness, again, only in the dry maculopathy group, without history of CNV, a moderate correlation was found with initial and final BCVA. To our knowledge, Fujiwara et al (16) were the only authors to report a correlation between subfoveal choroidal thickness and BCVA in eyes with a history of CNV treated with PDT, IVR, or both. We also found a correlation in 2 of the 3 treatment groups (PDT and IVR), but this correlation was weak and it was only significant for macular choroidal thickness, instead of subfoveal choroidal thickness.
In our regression analysis, and among subfoveal choroidal thickness, age, sex, AL, type of myopic maculopathy, and kind of treatment used for myopic CNV, only AL was identified as a predictive parameter for BCVA in both interquartile and median models. Interestingly, subfoveal choroidal thickness was not predictive for BCVA in any of the models used in regression analysis. Thus, our results are not in accordance with previous reports. Nishida et al (27) reported that the only significant predictor of visual acuity was subfoveal choroidal thickness, in spite of the significant inverse correlation between AL and visual acuity found in their study. Also, they included only eyes without history of CNV, and in our study most eyes have history of myopic CNV. In fact, they state that their study demonstrates that choroidal thickness is the most important predictor for visual acuity in high myopia but only in eyes without macular pathology such as CNV. Wang et al (28) also demonstrated that only age and macular choroidal thickness were significant predictors of BCVA, whereas refractive error and AL showed no significant association with BCVA. However, they also included only eyes without CNV. Therefore, in eyes with history of myopic CNV, the relationship of visual acuity to choroidal thickness and AL is less clear, and more studies are needed to clarify this topic.
Sex was also identified as a predictive parameter with negative contribution to visual acuity, but only in the median regression analysis. However, male patients had a significantly superior AL in our study, which may justify the male sex association with worse BCVA. The small sample (15 eyes in men vs 27 eyes in women) may have contributed to this outcome. Recently, Wei and associates also found that male sex was associated with thicker choroids in a large population (35). Male sex showed a positive predictive value for choroidal thickness in our study, which included only highly myopic eyes. Therefore, this point should be further explored and taken into account when performing comparative studies of choroidal thickness in the future.
Both baseline and final BCVA were inferior in the PDT group compared to all other groups, but final mean AL in the PDT group was significantly superior to the AL of all other groups, and regression analysis identified AL as the strongest predictor of BCVA. Another aspect is that PDT eyes also have higher prevalence rates of patchy and diffuse chorioretinal atrophy and a lower rate of tessellated fundus compared to the other 3 groups. This reinforces the idea that eyes in the PDT group are probably in a more advanced stage of myopic maculopathy, with higher AL and associated lower visual acuity. Also, type of treatment had no predictive value in regression analysis for BCVA and inferior functional outcome in the PDT group was therefore probably more related to the demographic characteristics of the sample and not the type of treatment performed.
At the end of follow-up, visual acuity stabilized in all groups regardless of the treatment used. These results appear to be in contradiction with previous reports of superior functional and anatomical outcomes in eyes treated with anti–vascular endothelial growth factor (VEGF) compared to eyes treated with PDT (32, 34). However, those studies compared the functional outcomes at 1 or 2 years follow-up, and instead we evaluated them in eyes with minimum follow-up of 3 years. We speculate that other factors in the natural history of the disease, like the development of macular atrophy around a regressed CNV, could contribute to limit in the long term the initial visual gain, so that in time the superiority of one kind of treatment over the other is lost. For example, El Matri et al showed that 12 months after starting treatment for myopic CNV with anti-VEGF, gain in BCVA was no longer significant (32). Again, type of treatment had no predictive value for final BCVA in this study, reinforcing the idea that other factors may be of a much greater prognostic importance in myopic CNV. Further studies addressing this topic in eyes with long-term follow-up are needed to clarify and support these findings. In this study, we also showed that the type of myopic maculopathy lesion was associated with choroidal thickness: the tessellated fundus lesion had the highest values of choroidal thickness, followed by macular atrophy, diffuse chorioretinal atrophy, and patchy chorioretinal atrophy. Choroidal thickness readings of tessellated fundus were not only higher, but also statistically different from the choroidal thickness readings of the other lesions recorded. The choroidal thickness associated with patchy atrophy was significantly inferior to the other 3 phenotypes recorded. Our regression analysis showed also that type of myopic maculopathy was predictive of choroidal thickness, with tessellated fundus being predictive of thicker choroids while patchy chorioretinal atrophy was predictive of thinner choroids. This was also in accordance with Wang et al (28). He and his associates found that the choroid in eyes with tessellated fundus is significantly thicker than in eyes with diffuse atrophy, and that presence of lacquer cracks was associated with even thinner choroidal thickness. We completed his evaluation by including eyes with all types of myopic maculopathy phenotypes proposed by Hayashi et al and showing their predictive value on choroidal thickness (29). Our findings are also in accordance with their work on the natural history of pathologic myopia, which showed that the tessellated fundus may be the first fundus lesion observed in myopic maculopathy, and is characterized by younger age, better BCVA, less myopia, shorter AL, lower incidence of staphyloma, and now with thicker choroids. Also and in accordance with the progression pattern proposed by Hayashi et al, diffuse and patchy atrophy are more advanced stages of myopic maculopathy and therefore associated with progressively thinner choroids. We did not find lacquer cracks at the time of EDI OCT measurements, but they were found in color fundus images from the beginning of follow-up, and this is also in accordance with the statement by Hayashi et al that lacquer cracks appear more commonly early in the progression of myopic maculopathy and not in the late stages, as was the case in most eyes included in this study (29). Macular choroidal thickness is probably an important factor in myopic maculopathy progression, affecting the prognosis, and can be a good indicator of its severity, as suggested by Wang et al (28).
There are important limitations to this study. Besides its retrospective design and small sample, choroidal thickness measurements were obtained manually by 2 independent observers, because currently there is no automated software to measure choroidal thickness, and also the variability of measurements for very thin choroidal measurements has not been determined. New automated software will reduce the bias involved and the time required to measure macular choroidal thickness. Although the overall group was not small, the subgroups were, and follow-up was different. However, and for the first time, we evaluated both subfoveal and macular choroidal thickness after different treatments for myopic CNV, showing that type of treatment has no influence on choroidal thickness. We found also that choroidal thickness is related to macular myopic lesions found at the retinal level.
In conclusion, the choroid in highly myopic eyes is very thin and undergoes further thinning as the myopic maculopathy progresses. Significant differences in choroidal thickness between myopic maculopathy patterns were found. Older age and greater AL are the major factors associated with macular choroidal thinning and the type of treatment showed no predictive contribution for choroidal thickness.