
Abstract
Purpose:
To investigate the effect of axial length on peripapillary retinal nerve fiber layer (RNFL) thickness in myopic, hyperopic, and emmetropic eyes in children by Cirrus HD spectral-domain optical coherence tomography (OCT).
Methods:
Subjects were divided into 3 groups according to their refractive status: myopic (n = 36), emmetropic (n = 30), and hyperopic (n = 28) eyes. The RNFL thickness measurements were taken from the superior, inferior, nasal, and temporal quadrants in the peripapillary region by Cirrus HD OCT. Axial length was also determined for each patient.
Results:
The myopic eyes had thinner average RNFL and RNFLs of temporal, superior, nasal, and inferior quadrants than the hyperopic eyes (p1<0.001, p2 = 0.004, p3 = 0.011, p4 = 0.006, p5 = 0.033, respectively). In addition, average peripapillary RNFL thickness and RNFL thicknesses of all quadrants had significant negative correlations with axial length. On the other hand, after applying modified Littmann formula for correction of magnification effect, the differences among the 3 groups disappeared (all p>0.05).
Conclusions:
We have shown that axial length and accordingly refractive status influenced peripapillary RNFL thickness measurements by Cirrus HD OCT in children. Therefore, to make a correct diagnosis of glaucoma or other optic neuropathies in children, either axial length—induced magnification effect should be corrected by ophthalmologists or the current Cirrus HD OCT database should be revised taking axial length into consideration.
Keywords
Introduction
Evaluation of peripapillary retinal nerve fiber layer (RNFL) thickness is an important method for detecting early glaucomatous damage (1, 2). Optical coherence tomography (OCT), which provides in vivo quantitative analysis of peripapillary RNFL, has been extensively used for the diagnosis and follow-up of glaucoma and other optic neuropathies (3, 4). However, all the commercially available OCT devices have databases including only individuals 18 years of age and older.
The latest OCT devices, spectral-domain (SD) OCTs, supply higher resolution and faster scan rate compared with time-domain (TD) instruments (5). Previous studies using TD-OCT have shown that RNFL thickness measurements could be affected by axial length and refractive status of the eye not only in adults but also in children (6-9). In addition, recent studies using Cirrus HD SD-OCT have demonstrated the influence of axial length on measurements of RNFL thickness in healthy adults (10-12). Kang et al (12) evaluated the effect of myopia on peripapillary RNFL thickness. They showed that axial length affected the average RNFL thickness, and myopia affected the RNFL thickness distribution. High myopic subjects were likely to exhibit different RNFL distribution patterns. They stated that since ocular magnification significantly affects the RNFL assessments in such patients, this should be considered in diagnosing glaucoma. Savini et al (10) demonstrated that RNFL thickness decreased with longer axial lengths in all 4 quadrants and average measurement. Correcting for axial length—induced ocular magnification by means of the Littmann formula resolved the relationship between axial length and RNFL thickness.
In a recent study (13), peripapillary RNFL thicknesses of myopic, emmetropic, and hyperopic children's eyes were compared using RTvue SD-OCT (Optovue, Fremont, California, USA), and it has been revealed that RNFL thickness profiles were significantly different among these eyes. Spherical equivalent (SE) refraction had a significant effect on RNFL thickness and for every diopter change toward hyperopia, the average RNFL thickness increased by 1.7 microns. However, the study did not investigate whether the correction of axial length—related magnification effect could eliminate these differences in children as in adults. In the present study, we aimed to investigate and compare peripapillary RNFL thicknesses of myopic, emmetropic, and hyperopic children's eyes and to evaluate the correlation between the peripapillary RNFL thickness and axial length by one of the most widely used SD-OCTs, Cirrus HD OCT. In addition, we evaluated if correction of ocular magnification could resolve the relationship between axial length and RNFL thickness in children.
Materials and Methods
Ninety-four eyes of 94 children were enrolled in the study. Subjects were divided into 3 groups according to their refractive status: myopic (n = 36), emmetropic (n = 30), and hyperopic (n = 28) eyes. All subjects and parents were informed about the study and consented to participate. This study followed the tenets of the Declaration of Helsinki and it was approved by the local ethics committee.
Each subject underwent detailed ophthalmologic examination including determination of refractive error, visual acuity (by Snellen charts), and intraocular pressure (IOP) (by Goldmann applanation tonometry), slit-lamp examination, perimetry (by Octopus 101, Haag Streit, Koeniz, Switzerland), and funduscopy. The refractive error value was calculated via the SE by an ophthalmologic examination after a cycloplegic refraction test. The axial length was measured using ultrasound biometry (Micropach Model 200P, Sonomed, Lake Succes, N:Y: USA).
Subjects with astigmatism >2.00 D, amblyopia, retinal and optic disc diseases, choroidal crescent, peripapillary atrophy, corneal disorders, strabismus, glaucoma, IOP elevation, and a previous history of ophthalmic surgery or ocular trauma were excluded from the study.
Peripapillary RNFL thickness measurements were performed using Cirrus HD SD-OCT (Carl Zeiss Meditec), which has been shown to have an excellent reproducibility and reliability in the pediatric population (14). The measurements were performed by the same blinded investigator, with pupil dilation of the subjects. Average peripapillary RNFL thickness and peripapillary RNFL thicknesses of temporal, nasal, inferior, and superior quadrants were measured along a circle with a diameter of 3.46 mm around the center of the disc for each subject. The RNFL thickness was measured by averaging the results of 3 sequential circular scans. Cirrus HD OCT algorithms find the optic disc and automatically place a scan circle with 3.46 mm diameter around it. Scans with signal strengths <7 or with artifacts were excluded.
The Littmann formula (t = p×q×s) (15) as modified by Bennett et al (16) and later adopted by Leung et al (7) and Kang et al (12) was used to correct the ocular magnification effect. The details of the formula have been described by Kang et al (12) as follows: in this formula, t is the actual fundus dimension, p is the magnification factor for the camera of the imaging system, q is the magnification factor of the eye, and s is the measurement obtained using OCT. Factor p is an instrument-dependent constant. The ocular magnification factor q of the eye can be measured with the formula q = 0.01306 × (axial length–1.82). In addition, p is a constant in a telecentric system which is known to be 3.382 for Cirrus HD OCT. According to the formula, actual radius of scan circle on the fundus (mm) = 3.3820 × 0.01306 × (axial length–1.82) × 1.73 mm. Then, the real RNFL thickness at a 1.73-mm radius can be calculated from the RNFL thickness observed at a 1.73-mm radius.
In the Littmann formula, 1.82 is the distance from the cornea to the second principal plane. However, the correct reference point should be the exit pupil of the eye because telecentric systems place their focal point within an aperture stop, not at a principal plane, thereby describing the path of chief rays. That would make the 1.82 more appropriately 3.68, the distance from the cornea to the exit pupil of the eye. Therefore, in our analyses we used a modified Littmann formula as follows: actual average RNFL thickness at 1.73 mm radius circle = 3.382 × 0.01306 × (axial length–3.68) × observed average RNFL thickness on the optic disc cube scan.
Several methods have been used to estimate the ocular magnification factor on the basis of the degree of ametropia, keratometry, or axial length (12, 15-18). However, we used the axial length method because this method is believed to be more accurate than other methods (12, 19).
Statistical Analysis
Statistical analysis was performed by using SPSS version 16.0. All variables were checked with Kolmogorov-Smirnov test. Pearson correlation coefficients were used to assess relations between the RNFL thickness and axial length. Sex was compared with chi-square test. The other variables were compared by one-way analysis of variance test among the 3 groups. Levene test was used to evaluate the homogeneity of the variances. p<0.05 Was considered as statistically significant. When an overall significance was observed, dual post hoc tests were performed using Bonferroni test.
Results
Table I shows the descriptive and clinical parameters of the subjects. There were no significant differences among the groups concerning age and sex. SE and axial length were significantly different among the 3 groups (all p<0.001). The SE values ranged from –0.50 to –5.00 in the myopic eyes, from +0.50 to +7.50 in the hyperopic eyes, and from –0.25 to +0.25 D in the emmetropic eyes. All subjects had visual acuities of 1.0 or better. None of the subjects had evidence of glaucoma such as IOP ≥21 mm Hg, increased optic disc excavation, or visual field defect.
DESCRIPTIVE AND CLINICAL PARAMETERS OF THE GROUPS (MEAN ± SD)
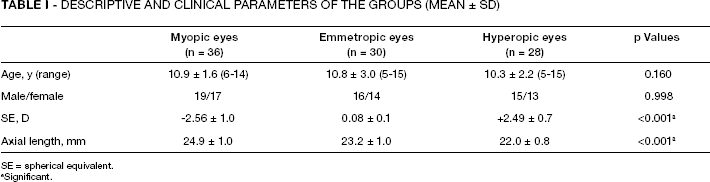
SE = spherical equivalent.
Significant.
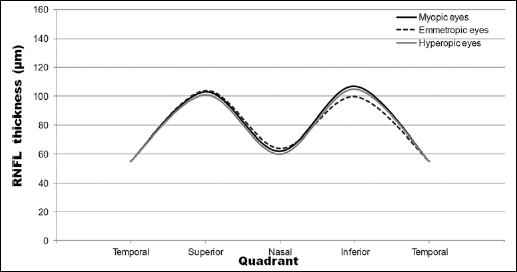
The peripapillary RNFL parameters of the subjects are given in Table II. Average RNFL thicknesses were 89.0 ± 6.6, 93.3 ± 7.9, and 98.6 ± 9.1 microns in the myopic, emmetropic, and hyperopic eyes, respectively. Average RNFL thicknesses and RNFL thicknesses of temporal, superior, nasal, and inferior quadrants were significantly different among the 3 groups (p1<0.001, p2 = 0.006, p3 = 0.010, p4 = 0.007, and p5 = 0.017, respectively). Pairwise tests showed that the myopic eyes had thinner average RNFL and RNFLs of temporal, superior, nasal, and inferior quadrants than the hyperopic eyes (p1<0.001, p2 = 0.004, p3 = 0.011, p4 = 0.006, p5 = 0.033, respectively) (Fig. 1). However, the emmetropic eyes had similar RNFL thicknesses with the myopic and hyperopic eyes in all quadrants (all p>0.05) except for inferior quadrant (p = 0.042, between the emmetropic and hyperopic eyes). On the other hand, after applying modified Littmann formula for correction of magnification effect, the differences among the 3 groups disappeared (p1 = 0.823, p2 = 0.874, p3 = 0.528, p4 = 0.717, and p5 = 0.178, for average, and temporal, superior, nasal, and inferior quadrants, respectively) (Tab. III, Fig. 2). After the corrections, average RNFL thicknesses were 81.5 ± 6.5, 80.6 ± 6.4, and 81.8 ± 8.2 microns in the myopic, emmetropic, and hyperopic eyes, respectively.
PERIPAPILLARY RNFL PARAMETERS OF THE GROUPS (MEAN ± SD) (IN MICRONS)
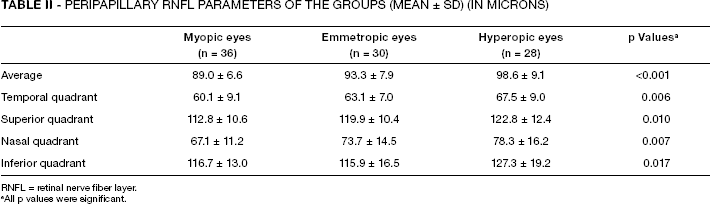
RNFL = retinal nerve fiber layer.
All p values were significant.
PERIPAPILLARY RNFL PARAMETERS OF THE GROUPS AFTER CORRECTION OF MAGNIFICATION EFFECT (MEAN ± SD) (IN MICRONS)
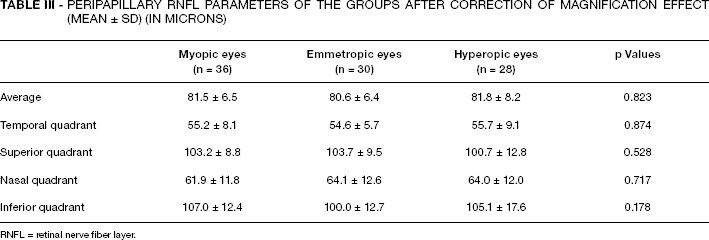
RNFL = retinal nerve fiber layer.
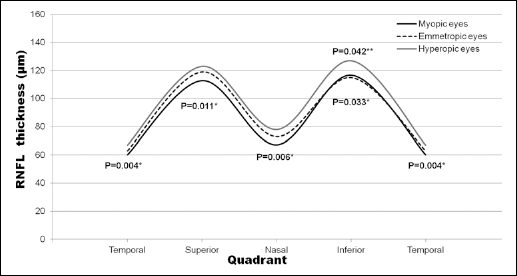
Comparison of Cirrus HD spectral-domain optical coherence tomography retinal nerve fiber layer (RNFL) thickness profiles among the myopic, emmetropic, and hyperopic eyes. *For comparison of myopic and hyperopic eyes by Bonferroni test. **For comparison of emmetropic and hyperopic eyes by Bonferroni test.
Comparison of Cirrus HD spectral-domain optical coherence tomography retinal nerve fiber layer (RNFL) thickness profiles among the myopic, emmetropic, and hyperopic eyes after correction for ocular magnification. All p>0.05 for comparisons among the 3 groups (one-way analysis of variance).
Correlation analyses among all the subjects showed that average peripapillary RNFL thickness and RNFL thicknesses of temporal, superior, nasal, and inferior quadrants had significant negative correlations with axial length (r1 = –0.442, p1<0.001, r2 = –0.288, p2 = 0.006, r3 = –0.498, p3<0.001, r4 = –0.340, p4 = 0.001, r5 = –0.303, p5 = 0.004, respectively) (Fig. 3). However, after correction of magnification effect, average peripapillary RNFL thickness and RNFL thicknesses of temporal, superior, nasal, and inferior quadrants had no significant correlation with axial length (r1 = 0.147, p1 = 0.174, r2 = 0.195, p2 = 0.070, r3 = 0.131, p3 = 0.226, r4 = –0.040, p4 = 0.715, r5 = –0.187, p5 = 0.084, respectively) (Fig. 4).
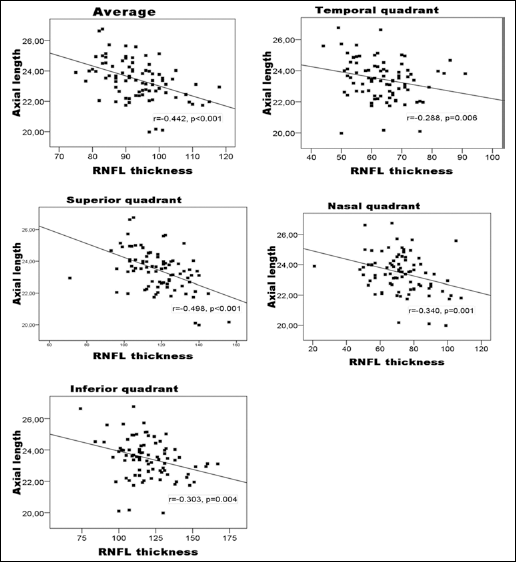
Correlation between axial length (mm) and average, temporal, superior, nasal, and inferior retinal nerve fiber layer (RNFL) thicknesses (microns) in the study subjects.
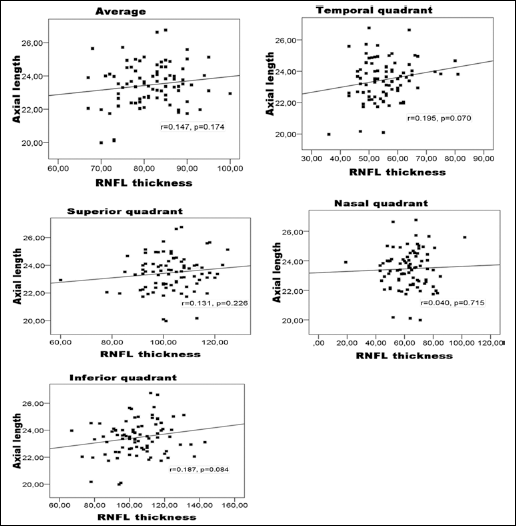
Correlation between axial length (mm) and average, temporal, superior, nasal, and inferior retinal nerve fiber layer (RNFL) thicknesses (microns) in the study subjects after correction of ocular magnification effect.
Discussion
The present study showed that the myopic eyes in children had significantly lower measurements of average peripapillary RNFL thickness and peripapillary RNFL thicknesses of all quadrants than the hyperopic children's eyes by Cirrus HD SD-OCT. In addition, axial length was conversely correlated with peripapillary RNFL thickness in all quadrants in the study population. However, these differences and correlations disappeared after correction of ocular magnification effect.
Recently, by using SD-OCT devices, it has become possible to measure peripapillary RNFL thickness with better resolution and much faster scan rate (5). However, as in TD-OCTs, these devices do not perform any adjustment for correcting ocular magnification (10). Therefore, comparing the RNFL thickness measurements with the normative database of the internal software may be misleading for diagnosis and follow-up of glaucoma or other optic neuropathies.
Several studies using TD-OCT have revealed that mean peripapillary RNFL thickness was conversely correlated with axial length in myopic and hyperopic populations of both adults and children (6-9). Recently, a few studies (10-12) have investigated the effect of axial length and refractive status on peripapillary RNFL thickness by Cirrus HD SD-OCT. Yoo et al (11) have found that with the exception of the temporal quadrant, which had a positive correlation, average 360° RNFL thickness and RNFL thicknesses of superior, inferior, and nasal quadrants showed significant negative correlations with axial length in young adults. However, they did not perform the correction of magnification effect. In a recent study, peripapillary RNFL thicknesses of 15 short (<22.5 mm), 15 medium (22.5-25.5 mm), and 15 long (>25.51 mm) eyes of adults aged between 25 and 55 years were measured and compared (10). There were statistically significant differences among the mean values measured in short, medium, and long eyes, in all quadrants, with the only exception of temporal quadrant, which had no correlation. In addition, RNFL thickness decreased with longer axial lengths in superior, inferior, nasal, and temporal quadrants, as well as in 360° mean measurement. In accordance with our study, correcting for axial length—induced ocular magnification by means of the Littmann formula resolved the relationship between axial length and RNFL thickness. Our results might be caused by the relationship between axial length and peripapillary RNFL thickness due to 2 reasons. First, the refractive error is strongly dependent on the axial length; secondly, previous studies have shown that RNFL thickness values do not change after excimer laser surgery to correct myopia (20, 21).
The RNFL thickness is conversely related to the distance from the optic nerve head center in healthy subjects (22, 23). The scan circle with larger diameter of myopic eyes results in a larger distance from the optic nerve head center. Therefore, it is not surprising to find that RNFL thickness measurements are lower in myopic eyes than in hyperopic eyes. As a result, comparison of RNFL thickness between the eyes with longer or shorter axial length using the same-sized scan circle may be misleading. For example, when we applied the Littmann formula to the standard radius (1.73 mm), the radius decreased to 1.39 mm in a 20-mm-long eye and to 1.85 mm in a 26-mm-long eye. When the axial length—induced ocular magnification was taken into account by correcting the measured values, the statistical relationships disappeared. To our knowledge, this is the first time we have found that correction of magnification effect by Littmann formula erased the relationship between axial length and peripapillary RNFL measured by Cirrus HD SD-OCT in children.
There was no subject flagged by the instrument as glaucoma suspect among our subjects. We believe that it was because of that there was no subject with very high myopia in our study (the SE of myopic subjects were ranged from -0.50 to -5.00 in the myopic eyes). If there were paitents with higher myopia thay could be considered as glaucoma or glaucoma suspect by the instrument. According to our results, increased axial length increased the possibility that RNFL thickness values would be below the normal limits. Therefore, measurements obtained from myopic eyes might cause overdiagnosis of glaucoma. On the other hand, decreased axial length increased the possibility that the RNFL thickness values would be above the normal limits. Accordingly, measurements obtained from hyperopic eyes might cause underdiagnosis of glaucoma.
In conclusion, we have shown that axial length and accordingly refractive status influenced peripapillary RNFL thickness measurements by Cirrus HD OCT in children. The current normative database may be misleading for a correct diagnosis of glaucoma or other optic neuropathies in varying degrees of myopia or hyperopia in children. Therefore, to make a correct diagnosis, axial length—induced magnification effect should be corrected by ophthalmologists or the current Cirrus HD OCT database should be updated by taking axial length into consideration.