
Abstract
Purpose:
We describe a technique to avoid decentration of the visual axis of the Boston type 1 keratoprosthesis (Kpro), performing 2 concentric trephinations with femtosecond laser.
Methods:
Two concentric side cuts were performed in a donor cornea using the 150-kHz Intralase™ FS laser. Within the same applanation procedure, an 8.5-mm-diameter anterior side cut was performed, followed by a concentric 3-mm-diameter anterior side cut.
Results:
The technique was successfully replicated in 7 cases.
Conclusions:
Femtosecond laser-assisted double trephination results in a correctly prepared donor cornea, and in an inner side precisely matched with the prosthesis. At the end of the surgery, the Kpro was correctly centered.
Introduction
The Boston keratoprosthesis (Kpro) is the most widely used artificial cornea or keratoprosthesis. It is a treatment option for corneal disease cases not amenable to standard penetrating keratoplasty: in particular, it was developed to treat patients with blindness due to end-stage corneal disease and poor prognosis for penetrating keratoplasty, such as eyes with repeated graft failure, severe corneal neovascularization, and limbal stem cell deficiency as a result of chemical and thermal burns, provided the ocular surface is still wet (1, 2).
Several different devices exist, but the Boston type 1 Kpro is the treatment of choice for eyes with adequate tear film and a functional blink (3-4-5). The device was approved by the Food and Drug Administration for marketing in 1992. An active keratoprosthesis research program continues in Boston and other centers worldwide, fostering continued innovation with the device. Recent advances in design have contributed to improved outcomes (6-7-8-9-10).
However, as with any new procedures, the optimal parameters for the surgical technique are continually being refined. Surgical preparation of the Boston type 1 Kpro involves using a full-thickness corneal donor button, 8.5—9.0 mm in diameter, with a central trephined 3-mm hole: centration of the 3-mm Kpro pupil on the fovea is integral for image quality and its optics afford excellent visual acuity and field of vision assuming that the alignment of the Kpro is optimized (11). The manufacturer's recommended steps for Kpro preparation involve punching the donor with an 8.5-mm or greater diameter followed by a 3-mm central punch, but creating the inner 3-mm hole first, centering the outer ring on the inner hole, has been hypothesized to improve centration (12). Sarayba et al (13) demonstrated an alternative to more challenging manual dissection methods for Alpha-Cor-like Kpro implantation and centration with femtosecond laser: the surgical technique was further refined and allowed for rapid and easy execution. Moshirfar et al (14) described a replicable technique for femtosecond laser—assisted preparation on an artificial chamber of donor tissue for Boston type 1 Kpro, to provide accurate double trephination for optimized alignment in the visual axis. This procedure requires 2 consecutive full-thickness cuts (performed with 60 kHz Intralase™ FS laser; Abbott Medical Optics, Abbott Park, Illinois, USA) and before the second cut, the laser cone must be lifted off the surface of the cornea and reapplanated, with risk of fluid flowing through the cut, and positive probability to cause distortion of the cornea producing definitive asymmetric Kpro unit.
We propose a modification of this technique for minimizing centration error and producing smooth trephinated edges (both central and peripheral) without loss of contact between the cornea and the applanation cone of the femtolaser.
Materials and Methods
From December 2011 to April 2013, a consecutive series of 7 patients (7 eyes) underwent a Boston Kpro implantation. Beneficial effects and potential complications of the surgical procedure were explained to all patients. Fully informed consent was obtained from each patient and each case has been studied in a prospective manner. Prior to surgical intervention, all patients underwent a baseline ophthalmic examination that included measurement of best-corrected visual acuity, biomicroscopy, applanation tonometry, B-scan ultrasonography, and ultrabiomicroscopy (UBM).
Surgical Procedure
A 20-cc syringe filled with preservative liquid of the cornea donor was connected via a 3-way connector to the artificial anterior chamber (Coronet, Artificial Anterior Chamber. Network Medical Products Ltd., North Yorkshire, England). A corneoscleral rim was then inserted into an artificial anterior chamber and laid on the endothelial side on a preservative fluid bubble, and secured onto the artificial anterior chamber. The syringe plunger was pushed down by the surgeon: pushing increases the force on the plunger, increasing the pressure on the test chamber. Pressure was maintained by closing the 3-way connector and by blocking the test chamber screw, ensuring maximum stability.
Central corneal thickness was obtained using an optical coherence tomography (OCT) online pachymeter integrated in the Schwind Amaris Excimer Laser system (Schwind Eye-Tech-Solutions, Kleinostheim, Germany): the advantages of online pachymetry are high resolution in micrometer range (through an interferometric principle) and no requirement of contact with the cornea.
Grafts were prepared and measured in this way, and were then firmly laid on a suitable table, and placed under the aperture of the 150-kHz Intralase™ FS laser (Abbott Medical Optics) (Fig. 1).
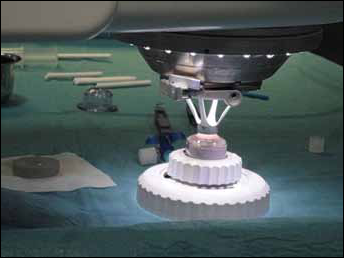
Applanation of the donor cornea.
Applanation was achieved next and without a suction ring, together with centering and cutting, according to the described procedures.
Two consecutive full-thickness flaps were performed with the femtosecond laser: each cut was performed with the same ID, changing parameters only switching eyes and planning 2 consecutive procedures. The setting for the first cut included an anterior side cut depth of 800 μm, diameter of 8.5 mm, and energy of 2.1 μJ. The side cut parameters were as follows: angle 90 degrees, spot and line separation 3/2. For the second cut, the parameters were kept the same, but diameter was changed to 3 mm and depth 900 μm.
To prevent distortion of the cornea, only one applanation was performed (“one touch”) and the procedures were performed consecutively, changing only OD and OS of the same ID without redocking twice. For this purpose, a different thickness was planned, and a different diameter in OD and OS, switching the eye schedule by software and maintaining the same cone and applanation pressure. This allows time savings as well as the preservation of pressure in the opened anterior chamber (Fig. 2).
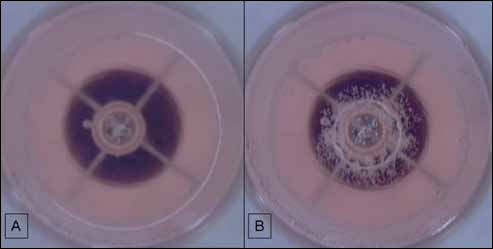
The
Once the procedure was finished, a forceps was used for easily dissecting the sclerocorneal graft (Fig. 3).

Separation of the donor button after the femtosecond-assisted trephination.
After the femtosecond-assisted carrier tissue preparation, the Boston Kpro was assembled according to the international protocol standard technique.
Sixteen 10-0 nylon single stitches were placed between the donor graft (with Kpro attached) and the patient's limbus.
After the surgical procedure, a semipermeable soft bandage corneal lens was placed (which should be changed every 3 months).
Postoperatively, the patients were generally discharged from the hospital after 1 day and then reviewed after 1 week, after 2 weeks, after 1 month, and every 1 month thereafter for 1 year and eventually every 3 months indefinitely.
Main outcomes measures were visual acuity and postsurgical complications.
Results
We studied 7 eyes of 7 consecutive patients (4 women and 3 men) who underwent femtosecond-assisted Boston Kpro implantation between December 2011 and April 2013. The mean age was 72.2 years (SD 10.1). The mean duration of follow-up was 11.8 months (SD 6.7) (range 4-20 months).
This technique was successfully applied in these 7 consecutive cases, all performed by the same surgeon (L.M.). The retention rate was 100% throughout the follow-up period.
The patients' demographic characteristics and preoperative and postoperative data are shown in Table I.
DEMOGRAPHIC DATA AND POSTOPERATIVE RESULTS AND COMPLICATIONS
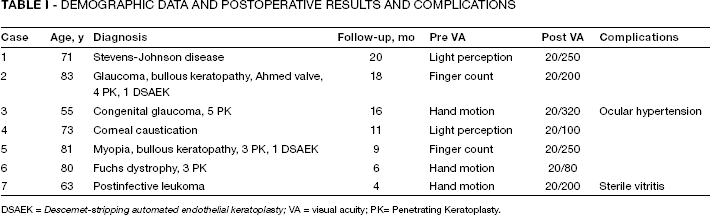
DSAEK = Descemet-stripping automated endothelial keratoplasty; VA = visual acuity; PK= Penetrating Keratoplasty.
Figure 4 shows one of the treated cases.
Discussion
Over the past 3 decades, Boston keratoprostheses have had some success in the treatment of corneal blindness but are associated with a high incidence of complications, including extrusion, corneal melting, infection, membrane formation, and glaucoma. In this respect, research actively continues on the Boston Kpro to improve design and outcomes and to expand indications for its use. Kpro patients are prone to develop inflammation, retroprosthetic membranes, and cellular debris within and around the PMMA back plate, and studies are investigating alternative keratoprosthesis materials including titanium (9, 15).
However, the preparation of the carrier tissue represents a crucial step, especially in the centering phase: the optics of the Boston type I Kpro rely on the centration of the central optic relative to the macula. The optical performance of the Kpro on an optical bench using a 3-mm pupil and precise alignment was evaluated and found to produce a sharp, crisp image with a tight point-spread function (16). The optical cylinder, under these optimized alignment conditions, produced scattered ghost images when the 3-mm pupil was widened to 10 mm. If the alignment of the Kpro is suboptimal with the cylinder off-axis from the fovea, then the projected image will most likely be further degraded (12). In addition to the optical advantages, a centered Kpro results in a much easier suturing to the host rim, with better distribution of tension. Khalifa et al (17) present a modification for minimizing centration error, punching the central 3-mm hole first and then using this hole to center within the Barron corneal punch's 4 vacuum ports.
Moshirfar et al (14) demonstrated that the femtosecond laser produces well-centered cuts with smooth trephinated edges and the use of an artificial anterior chamber avoids manual placement of the donor tissue, which can introduce decentralized error. However, in using this technique, they note that the peripheral edges are more irregular than the central edges due to a compromised anterior chamber system after the first full-thickness central cut: this may produce an oval Kpro unit and a potential mismatch when trying to insert the assembled unit into the recipient corneal opening.
With our technique, we are able to compensate for this inconvenience (Fig. 4) using a technical expedient: by switching OD to OS, we can carry out 2 procedures while keeping a single applanation, thus avoiding the risk of compromising the integrity of the anterior chamber. In addition, by carrying out the peripheral cut in advance, the probability of an anterior chamber collapse decreases, since ab interno pushing forces will arise on the apex of the corneal dome more than peripherally.
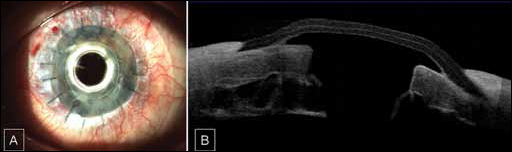
Keratoprosthesis and recipient cornea optimal juxtaposition after one-touch femtosecond-assisted trephination.
This process generates 2 relevant effects: first, the resulting cuts are perfectly concentric; secondly, cut margins are very regular, enabling a correct insertion of the optical section centrally, and a perfect peripheral congruence between donor and receiver.
Our technique was replicable and keratoprosthesis implantation can be facilitated by evaluating the effects of varying surgical parameters on mechanical stability.