
Abstract
Purpose
There are many independent factors that influence the outcome of refractive surgeries, consisting of patient characteristics and environmental factors. We studied the accuracy of central ablation depth compared to online pachymetry results.
Methods
A total of 153 eyes that underwent TransPRK at Bina Eye Hospital, Tehran, Iran, were evaluated from November 2010 to January 2012 in a retrospective cross-sectional study. The relevant data were registered and bivariate correlations and linear regression association were investigated statistically.
Results
The mean age was 29 ± 5 years. Distribution of refractive errors was as follows: compound myopic astigmatism 123 (80.4%), simple myopia 24 (15.7%), and mixed astigmatism 6 (3.9%). Mean ambient temperature and humidity levels intraoperatively were 23.49 ± 1.16°C and 28.91 ± 6.16%, respectively. There was a significant difference (p<0.001) between the preassumed central ablation depth (131.68 ± 32.72 μm) and the net level of ablation depth (measured by online pachymetry, 168.04 ± 41.47 μm). Temperature and humidity levels were not in any statistically significant correlation with the net amount of difference found. The backward linear regression was done to reveal the association between ablation depth and several variables.
Conclusions
This study showed that there is deviation in optical coherence pachymetry online measurements done with SCHWIND AMARIS laser. Ambient temperature and humidity levels intraoperatively do not influence the outcome. However, basic structural characteristics of patients along with change in refractive index and corneal shrinkage because of corneal dehydration are associated with the differences.
Introduction
Refractive errors of the eye are correctable with corneal laser refractive surgeries. They are currently the most accurate treatments with the fewest side effects (1). Transepithelial photorefractive keratectomy (TransPRK) corrects the corneal curvature without creating a flap (1). A laser pulse is applied to remove an appropriate amount of corneal tissue from a spherocylindrical surface in either of the techniques.
This new single-step approach is superimposing a defined epithelial thickness profile (almost 55 μm at the center and 65 μm at the periphery 4 mm radially from center) with aspheric ablation profiles. Corneal thickness plays an important role in the outcome of such surgeries. It influences all stages of the treatment (2), and provides a structural support (3). The ablation process cannot be adjusted after the initial programming starts. However, stromal evaporation and swelling during laser treatment may diminish the accuracy of the results (2, 3). Overablation leads to unwanted correction, and may cause postoperative corneal ectasia (4–6).
There are many independent factors that are found to affect the volume of ablation depth in laser methods other than TransPRK. They consist of several patient characteristics and environmental factors. Patient-specific data, pre-operative shape of cornea, planned ablation depth, laser setting, and environmental setup are believed to be influential (7, 8).
Optical coherence pachymetry (OCP) is a noncontact method of measuring corneal thickness intraoperatively (9–12). It may improve safety in any laser procedure by providing insight into the physical changes of the cornea during surgery. Optical coherence pachymetry has been employed for real-time monitoring of photorefractive keratectomy (PRK) (11), laser-assisted in situ keratomileusis (LASIK) (10, 12-14), and laser-assisted subepithelial keratomileusis (14) techniques and its reliability and applicability is established.
We evaluated the difference between the planned and the measured central ablation depth (CAD) (OCP) right after laser ablation termination. Possible factors causing deviation were investigated.
Methods
A total of 153 eyes of 80 patients that underwent TransPRK eye surgery from November 2010 to January 2012 at Bina Eye Hospital, Tehran, Iran, were retrospectively studied. We evaluated the difference between the intended CAD and the OCP measured corneal thickness removal. A single surgeon carried out all the procedures employing the SCHWIND AMARIS 500 laser (SCHWIND eye-tech-solutions GmbH, Kleinostheim, Germany).
All patients signed a provided informed consent. Approval for this study was obtained from the local institutional review board at Tehran University of Medical Sciences, Tehran, Iran, in accordance with the Declaration of Helsinki. They all had pre-operative examinations providing their general characteristics. Patients discontinued wearing contact lenses for at least 2 weeks prior to surgery. Environmental conditions, ambient air humidity and temperature, were recorded by standard devices that are incorporated in the laser. Room temperature and humidity were also controlled by standard devices in the operating room.
Surgery and Laser Setting
Patients' records are rechecked after entering the operation room for complete pre-operative examination and data. The intended eye to be treated is periorbitally scrubbed with povidone-iodine 10% topical antiseptic and anesthetic drops (Anesthocain 0.5%, Sina Darou, Tehran, Iran) are administered. The laser device is calibrated every 2 hours and the laser fluence and voltage (low/high) is determined with regards to the ambient temperature and humidity. The laser tracker is also calibrated. Static cyclotorsion control is investigated prior to patient's supine position and then is reinvestigated after positioning. Dynamic cyclotorsion control starts with initiation of the ablation process. After patient preparation and positioning, the laser ablation plan is set into integrated CAM software (aberration-free mode). Several variables are defined including patient's name, age, sex, corneal properties (curvature, thickness, optical zone), and CAD. The ablation process begins and there is no alcohol administration through the procedure. Mitomycin and antibiotic eyedrops are utilized at the end of the operation.
Online OCP
Online OCP, an optical coherence tomography (OCT) device, was used as previously described (9, 10, 12). Optical coherence pachymetry is a noncontact pachymetry technique that uses 1310-nm wavelength light waves. Low coherence light reflects and scatters on the surface of the eye and at the posterior corneal surface. The interferometer uses a parallel reference light beam to measure the light travel time. It continuously measures the central corneal thickness without interrupting the laser procedure. Nowadays, it is inserted inside laser systems as a third-generation device.
The OCP measurements (Heidelberg Engineering GmbH, Heidelberg, Germany) were recorded pre-operatively (with first alignment of the eye) and postoperatively (at the end of the procedure). After laser ablation, the true stromal thinning (measured CAD [OCP]) was calculated as the difference between these 2 values. The deviation in pachymetry between measured CAD (OCP) and planned CAD was calculated (deviation pachymetryOCP-planned = CADOCP –CADplanned). Refractive outcomes were evaluated at a 3-month interval.
Statistical analysis
Data were analyzed using SPSS version 17 (SPSS Inc., Chicago, Illinois, USA). The absolute values of measured (OCP) and planned CADs were compared by t test. Bivariate and multivariate correlations (Pearson product-moment correlation coefficient) and multiple linear regression association with backward variable selection were statistically investigated to evaluate contributors to deviation in pachymetry. Refractive outcomes were compared postoperatively using paired sample analysis. p Values <0.05 were considered statistically significant.
Results
Table I summarizes the patients' general characteristics. More patients were female. Most of the patients had compound myopic-astigmatism refraction error.
Participants' Demographic Data
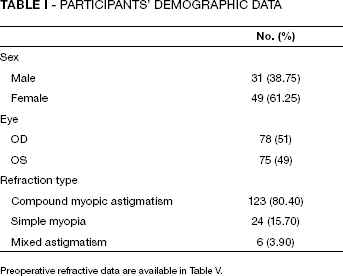
Pre-Operative refractive data are available in Table V.
Patient age ranged from 19 to 50 years. Refractive features and different laser settings are included in Table II. Temperature and humidity were roughly consistent with the standard range (operation mode standard temperature 18°C–24°C, humidity 30%–45%). There is a difference between mean ablation and treatment times (~16 seconds), which is mainly due to the preablation period and is mostly related to patient incompliance and position changing. That causes a few seconds delay to reposition the eyes. Comparison between the mean value of CAD and deviation pachymetryOCP-planned showed a significant difference (131.68 ± 32.72 μm and 168.04 ± 41.74 μm, respectively, p<0.001). Univariate correlation analysis showed significant association of CAD, corneal astigmatism, ablation, and treatment time with deviation in ablation depth. Our results reveal that a higher value of CAD, ablation and treatment time, and corneal astigmatism causes deviation from the planned CAD (Tab. III).
- Participants' Study Parameters
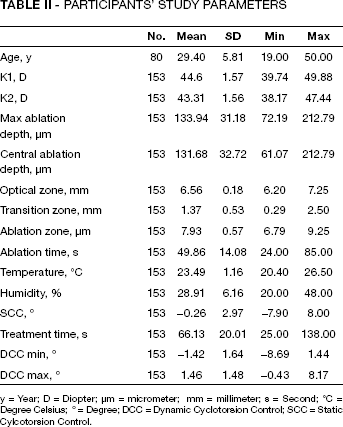
y = Year; D = Diopter; μm = micrometer; mm = millimeter; s = Second; °C = Degree Celsius; ° = Degree; DCC = Dynamic Cyclotorsion Control; SCC = Static Cylcotorsion Control.
Bivariate Correlation Analysis and Univariate Regression of Each Factor to Test Its Influence on The Difference of OCP Calculated Ablation Depth and Central Ablation Depth
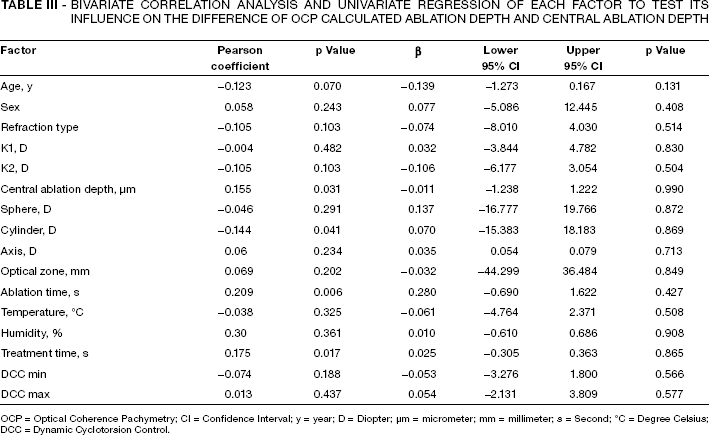
OCP = Optical Coherence Pachymetry; CI = Confidence Interval; y = year; D = Diopter; μm = micrometer; mm = millimeter; s = Second; °C = Degree Celsius; DCC = Dynamic Cyclotorsion Control.
Linear regression analysis with backward variable selection showed a significant model of influence of some investigated factors on deviation pachymetryOCP-planned (F = 2.907, R2 = 0.076, p = 0.024 with df 4). Random individual effects of age, sex, ablation time, and K2 are shown in Table IV. Follow-up visits at 3 months showed significant improvement for refractive errors (Tab. V).
Multiple Linear Regression Model Showing The Influence of Age, Sex, Ablation Time, and K2 On Deviation Pachymetry OCP-Planned
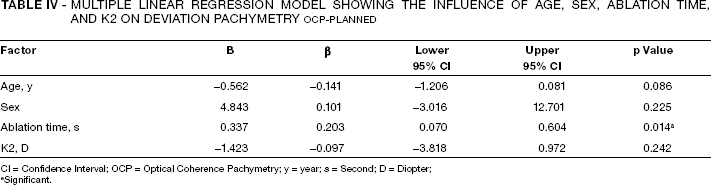
CI = Confidence Interval; OCP = Optical Coherence Pachymetry; y = year; s = Second; D = Diopter;
Significant.
- Refractive Outcomes Compared 3 Months Postoperation
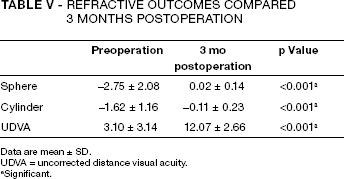
Data are mean ± SD.
UDVA = uncorrected distance visual acuity.
Significant.
Discussion
TransPRK could make errors in the rate of photoablation between the epithelial tissue and the stroma (15). Notably, there is a significant difference between preassumed CAD and the outcome of ablation measured by OCP; the ablation depth outcome shows a deviation from nominal values (28%, 36.36 μm, p<0.001). It is important to keep a minimum thickness of stromal tissue to save the mechanical integrity of the cornea. It should be kept in consideration that the main factor determining the corneal refractive power is its curvature and not the thickness. However, clinical outcomes after months or a year must be considered and surveyed. The scarring process, epithelial changes, hyperplasia, and other factors will affect the postoperative measurements. Our ongoing study shows promising clinical results for uncorrected distance visual acuity follow-up at 3 months postoperation (Tab. V). Together with the fact that ablation time was the best predictor for the observed differences and that TransPRK are ablations with much longer lasing time than other techniques, this confirms that the difference measured is not an overablation with a resulting overcorrection, but the difference measured is mainly due to intraoperative dehydration processes during excimer laser treatment, as described previously (9, 13, 16-18). Online OCT is reported to be sensible to a shift in the hydration index of the cornea (19). As dehydration is directly related to longer time of laser procedure, it justifies the significant effect of ablation time on the amount of deviation measured (Tab. IV).
Intraoperative ultrasound measurements encounter many restrictions. They require contact with the stromal bed, possible incitement of inflammation, and reproducibility of measurement location (13). This would interfere with the ablation process. Therefore, OCP noncontact technology could have relative advantages (11, 12, 20). Overablation is reported in many techniques and measurements (11, 16-18). Others have compared other techniques than OCP and provided data favoring OCP usage intraoperatively (14).
An important goal of TransPRK is to make an ablation depth of concisely predictable measures to have the most exact refractive correction. Central ablation depth depends on multiple factors in various refractive surgery methods. Patient pre-operative characteristics like corneal thickness (21), refraction specificities, age (22), or environmental factors like humidity and temperature (8, 23) are examples. Patient-to-patient different corneal epithelial thickness could be another factor (14). Therefore, ethnicity could play an important role as a confounding factor (Iranian population in our study).
Most of these factors act in conjunction (Tab. IV) and do not greatly affect the outcome of ablation (Tab. III). Using a multiple regression analysis with backward method, we investigated the potential influential factors to make a difference from the preassumed CAD (Tab. IV). Ablation time is found to be the most significant. It is anticipated that more ablation needed due to higher refractive errors results in a chance of more deviation. There may be other factors involved.
Interestingly, intended CAD was free of any dependence of humidity and temperature in our study, although operations were performed in a variety of environmental conditions (20.4°C–26.5°C, 20%–48% humidity). However, there is a known effect of dehydration due to exposure of stromal tissue to ambient air during ablation that could influence the removal (9, 13, 16-18). Optical coherence pachymetry measurement provides continuous measurement intraoperatively. It does not involve chemical or mechanical aids in the removal of the corneal epithelium. The single-step feature eliminates the potential risk of dehydration of the stromal bed. Unlike alcohol-assisted PRK, there is no risk of alcohol escape and unlike epi-LASIK, no epikeratome is required; therefore there is no risk of a stromal incursion (24).
Optical coherence pachymetry incorporated in laser platform was applied for each individual. Other studies have reported consistent OCP data with ultrasound and Orbscan measurements (13). Others found a slight difference in corneal thickness measured by different methods (12, 20, 25, 26). Optical coherence pachymetry measurement is not the only practical measurement and in cases who have had previous laser refractive surgeries, it shows some restriction due to changes in tissue clarity (27, 28). However, we excluded such cases. A possible deviation using the same technology was discussed previously (29), showing the safety limits of OCP. The OCP measures the difference in light traveling time between the reflections of anterior and posterior corneal surface (the phase difference) but uses the corneal refractive index (built in as a constant factor) to calculate out of that the corneal thickness (9, 10, 12). As the refractive index changes with dehydration, the pseudo-overablation indicated by OCP, especially at the end of the surgery and of course more evident in TransPRK (because of ablation time), is explainable.
Our results could help to improve laser algorithms by optimizing the default software values incorporated into laser instruments. However, we only assessed single point changes in corneal thickness, CAD, which provides good information about the residual stromal thickness but the changes in corneal curvature actively determines the clinical outcome. TransPRK demonstrates faster epithelial healing, excellent corneal clarity, stability, and reduced postoperative pain. It seems that given the simplicity, efficacy, and stability of the results, TransPRK could potentially become more mainstream (30).
There were limitations to our study. It was a retrospective study and data were extracted from electronic patient records. There may be confounding factors that we have not investigated. There is a possibility of a systemic shift of measurement device (change of refractive index), which takes over importance the longer the treatment lasts. We could include a sufficient number of cases; therefore a reliable analysis of studied parameters could be reached. We did not have postoperative real ablation measurements to compare the results; however, we compared our instrument results with its own measurements.
This study showed that there is deviation from intended CAD in TransPRK eye surgery with regards to OCP online measurements done with the SCHWIND AMARIS laser. This could be related mainly to change in refractive index and to corneal shrinkage because of corneal dehydration as the water content of the cornea decreases with time. Interestingly, intraoperative ambient temperature and humidity levels did not influence the outcome. Basic structural characteristics of patients are associated with differences, of which sphere and cylinder levels are directly under the instrument's operation area.