
Abstract
Purpose
To assess astigmatism induced by paired opposite clear corneal incision (OCCI) compared to single incisions and to investigate factors on which its effect depends.
Methods
The study comprised 326 eyes from 326 patients. In patients with <1.0 D corneal astigmatism, clear corneal incision was performed (CC group, n = 245), and in those with >1.0 D preoperative corneal astigmatism, a second, opposite clear corneal incision was made (OCCI group, n = 81). Both groups consisted of superior, temporal, and oblique subgroups according to the steepest meridian. Prior to the surgery, and after surgery, repeated keratometry was performed and surgically induced astigmatism (SIA) was calculated using vector analysis.
Results
Two weeks after the surgery, the SIA was 0.67 ± 0.44 D in the CC group and 1.15 ± 0.65 D in the OCCI group; 9 weeks after the operation, it was 0.61 ± 0.43 D in the CC group and 0.99 ± 0.57 D in the OCCI group (p<0.001). The SIA showed no significant postoperative change in our groups.
Conclusions
Opposite clear corneal incision reliably induces about 1.0 D of corneal astigmatism on the steep meridian in proportion to the rate of preoperative astigmatism. Its magnitude is independent of the location of the incisions and its effect remains unchanged during the postoperative period.
Introduction
Cataract surgeries are refractive interventions that, by using the latest techniques available, simultaneously aim to rapidly improve visual acuity without any correction, to decrease preoperative corneal astigmatism, and to restore accommodative processes as much as possible. It is well-known that residual astigmatism is one of the most significant limiting factors that has an impact on visual acuity and patient satisfaction after intraocular lens (IOL) implantation (1, 2).
Every procedure performed on the cornea induces a certain rate of astigmatism. Corneal incisions made during cataract surgeries reduce corneal power on the meridian of the incision. The rate of induced astigmatism is affected by the size (3–5), the shape (6), and the location of the incision (7–9). The paired opposite clear corneal incision (OCCI) technique, first described by Lever and Dahan (10), represents a further possible method for reducing astigmatism. This is in addition to limbal relaxing incisions (11), corneal refractive interventions, and toric IOL implantation.
The present study aims to assess the rate of corneal astigmatism induced by OCCI in comparison to clear corneal incisions with superior, temporal, and oblique locations, and to assess the postoperative changes of OCCI-induced astigmatism and the factors affecting it.
Patients and Methods
Our prospective study comprised 326 eyes from 326 patients waiting for cataract surgery. The mean age of the patients was 71.5 ± 8.5 years in the clear corneal incision (CC) group and 71.02 ± 13.26 years in the OCCI group (p = 0.7). The axial length was 23.4 ± 1.66 mm in the CC group and 23.57 ± 2.28 mm in the OCCI group (p = 0.61). Preoperative astigmatism was 0.61 ± 0.35 D in the CC group and 1.06 ± 0.34 D in the OCCI group. The exclusion criteria were any previous ocular surgery, trauma, corneal disease, or proved irregular astigmatism. The eyes were divided into 2 groups: in patients with <1.0 D preoperative corneal astigmatism, a clear corneal incision was performed (CC group, n = 245), and a paired OCCI was made in patients with ≥1.0 D preoperative corneal astigmatism (OCCI group, n = 81). Both groups consisted of superior, temporal, and oblique subgroups on the basis of the steepest corneal meridian. The orientation of corneal astigmatism was regarded as against-the-rule astigmatism in the case of the steepest keratometric readings being between 0-30 and 150-180 degrees, oblique astigmatism was between 30-60 and 120-150 degrees, and with-the-rule astigmatism was 60-120 degrees. Preoperative evaluation included visual acuity, refraction, assessment of spectacle correction, detailed slit-lamp biomicroscopy, applanation tonometry, dilated funduscopy, keratometry, and topography. Prior to each surgery, keratometric measurements were performed with the IOLMaster (Carl Zeiss Meditec, Jena, Germany, software version 5.4). A further calculation included the mean value of 3 automatically measured pieces of data.
Each phacoemulsification operation was performed under topical anesthesia by the same experienced ophthalmic surgeon using a coaxial technique. A 2-step clear corneal incision was performed with a 3.0 mm ClearCut blade (Alcon Laboratories, Fort Worth, Texas, USA) 1 mm anterior to the corneal limbus on the steepest corneal meridian defined by our previous keratometric measurements and marked at the slit-lamp examination with a needle. Then a 1.2-mm paracentesis was made at 60 degrees left of the main incision. During IOL implantation, there was no need for enlargement of the main incision. A breakdown of the incisions is as follows: 113 superior incisions were made, 53 temporal incisions, and 79 oblique CC incisions. After the incision was performed, a standard phacoemulsification was carried out, at the end of which a foldable IOL was implanted in the capsular bag.
In the OCCI group, at the end of the surgery, while the viscoelastic material was being removed, a second 3.0-mm CC incision was made at 180 degrees from the original incision by holding the aspirating handpiece in the eye. This allowed the surgeon perform a standard incision while keeping the bulbous tone. The opposite incision was performed the inferior position in 38 of the cases, in the nasal position in 23 cases, and in the oblique position in 20 cases.
At the end of the surgery, only CC incisions used for manipulation were hydrated; the OCCI incisions were not. The OCCI was also examined for leakage but we did not record any in any of the cases. During the first week of the postoperative period, patients received a combination of levofloxacin and dexamethasone, and eyedrops containing dexamethasone for a further 4 weeks.
At 2.13 ± 0.4 weeks and 8.9 ± 0.6 weeks postoperatively, all eyes were assessed for refraction and keratometry with the IOLMaster, and further calculations were performed with the mean of the 3 values obtained in an automated mode.
The methods of cataract operation and astigmatism reduction were explained to all patients and informed consent was obtained. The research protocol adhered to the tenets of the Declaration of Helsinki.
Statistical analysis was performed with MedCalc 10.0 and SPSS statistical software (SPSS 16.0, SPSS Inc., Chicago, Illinois, USA). Descriptive statistical results were described as mean, SD, and 95% confidence interval of the mean. The normality of the data was tested by the Kolmogorov-Smirnov test. If the normality was rejected (p<0.05), nonparametric test was used. In such cases, the Mann-Whitney U test was carried out for the comparison between groups or variables; in the case of comparing 2 or more groups, the analysis of variance (ANOVA) test was used; and the Spearman rank test was applied for the assessment of correlations. The surgically induced astigmatism (SIA) was calculated with Holladay-Cravy-Koch vector analysis (12) on the basis of the preoperative and postoperative results of automated keratometry. A p value below 0.05 was considered statistically significant.
Results
No incision-related complications (wound leak or endophthalmitis) were observed in the OCCI group. In the case of SIA, the Kolmogorov-Smirnov test rejects normality (p<0.001). In the second postoperative week, the overall SIA was 0.67 ± 0.44 D in the CC group and 1.15 ± 0.65 in the OCCI group; by the ninth week, it was 0.61 ± 0.43 D in the CC group and 0.99 ± 0.57 D in the OCCI group. In the case of the CC and OCCI groups that were divided into superior, oblique, and temporal subgroups, the astigmatism induction of CC incisions significantly depended on the place of the incision (ANOVA, p = 0.03); however, the magnitude of SIA was not affected by the locations of the incision in the OCCI group (ANOVA p = 0.9). Considering all 6 subgroups, the statistical occurrence of SIA is not significantly lower by the ninth week than by the second week of the postoperative period (p>0.05 in each case) and is only minimally so in a clinical sense. Preoperative and postoperative data are detailed in Table I; values of the 6 subgroups are shown in Table II.
Patient Characteristics
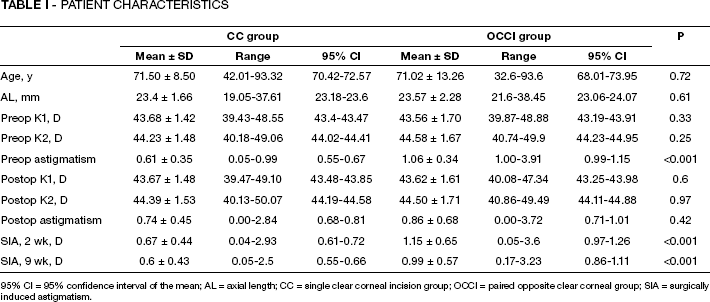
95% CI = 95% confidence interval of the mean; AL = axial length; CC = single clear corneal incision group; OCCI = paired opposite clear corneal group; SIA = surgically induced astigmatism.
Rate of Surgically Induced Astigmatism Based On The Locations And Types (Cc Or Occi) Of The Incisions 2 And 9 Weeks After Surgery
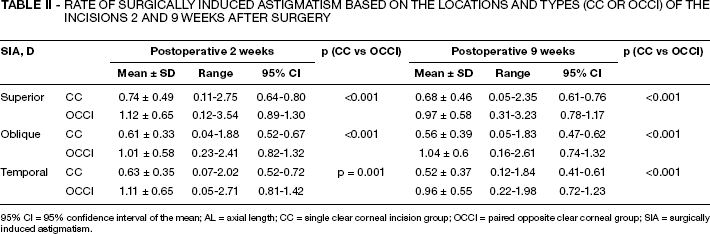
95% CI = 95% confidence interval of the mean; AL = axial length; CC = single clear corneal incision group; OCCI = paired opposite clear corneal group; SIA = surgically induced astigmatism.
A positive, significant correlation was found between preoperative corneal astigmatism and overall SIA assessed 2 and 9 weeks after surgery (r = 0.32 and r = 0.35, p<0.001), and we observed a weak but statistically significant correlation between age and overall SIA measured 2 and 9 weeks after operation (r = 0.15, p = 0.01; r = 0.16, p = 0.01).
Discussion
During cataract surgery, a spherocylindrical refractive change occurs. Nowadays, one of the main goals of cataract operations is to reduce, or at the very least to not enlarge, preoperative corneal astigmatism. During modern cataract surgeries, mostly clear corneal incisions are performed. It is well-known that corneal incisions induce corneal flattening on the meridian of the incision (13), and such induced astigmatism depends on the features of the incision (5–9). According to histologic examinations, clear corneal incisions heal within 60 days (14), and some publications suggest that the rate of SIA is certain to not change significantly within 6 weeks (15). Other studies propose that mean astigmatism may remain unchanged for 12 weeks (16) or even 1 year (17) after the clear corneal incision was performed. However, as this is all monitored by vector analysis, the results are highly dependent on the method of the calculation (17). Others observed small against-the-rule shifts in the cylinder 1 year after the operation (18). According to our examinations, there is a certain decrease in induced astigmatism between the second and ninth weeks of the postoperative period, but this neither exceeds the statistical level of significance nor is it clinically significant in CC and OCCI cases. Consequently, SIA is stable with respect to time in cases with 3.0-mm CC and OCCI incisions.
A number of studies have been published on the astigmatic effects of different corneal and scleral incisions (5, 9). It is known that temporal and sclerocorneal wounds induce smaller corneal flattening, while superior and clear corneal incisions induce larger corneal flattening on the meridian of the incision. Corneal incisions of 3.0 mm or more induce significant astigmatism (5, 7, 9, 19). In the case of microincisional cataract surgeries with incisions smaller than 2.0 mm, one would think that no significant astigmatic effect is induced; however, it has been recently proved that such incisions induce 0.42-0.5 D astigmatism (20).
Many publications confirm that superior incisions induce higher and indirect astigmatism, and that temporal incisions induce lower and direct astigmatism (7, 23). This is also supported by our study, in which we used 3.0-mm incisions. The underlying reason for the lower astigmatic effect of temporal incisions is likely that as sclerocorneal fibers run downwards, such incisions involve less fibers being cut (8), and also that the cornea is 1 mm larger horizontally than it is vertically.
Matsumoto et al (24) advise that if preoperative astigmatism is higher than 0.5 D, the major incision should be made on the steep meridian, and in the case of it being above 1.2 D, an incision longer than 3.2 mm or an additional incision should be performed.
Corneal astigmatism higher than 1.5 D can be treated by performing 2 opposite corneal incisions (paired OCCI) (10, 16, 30), limbal relaxation incision (31), excimer laser treatment, or toric IOL implantation.
Previous studies using the OCCI technique observed an overall SIA between 1.4 and 2.25 D after a postoperative period of 2 to 3 months (10, 16, 27, 29), although a significantly lower SIA of about 0.5-0.6 D, which almost equals the value of CC incisions, has also been reported in some literature (28, 30). All the SIA data detected after OCCI incisions and published in literature so far is summarized in Table III. It can be clearly seen that with a longer incision than made in our study, a higher SIA is usually observed. Lever and Dahan (10), the first to describe the OCCI technique, suggested paired corneal incisions in cases of preoperative astigmatism above 1.75 D. This level could be shifted to 1.0 D, as its effective results are suggested by our investigations, as well as the fact that in 95% of the cases, an induced astigmatism of about 1.0 D was obtained and at such keratometric readings another type of correction could not have been adopted. Moreover, the higher the preoperative astigmatism, the higher the rate of SIA detected by the OCCI method, though this is also true for the CC method. Due to the total size of the 2 incisions, the theoretical risk of endophthalmitis is higher in the case of OCCI; however, no related complications have been reported so far and no such case was observed in our study.
Surgically Induced Astigmatism With Paired Opposite Clear Corneal Incision Published In The Literature By Year Of Publication
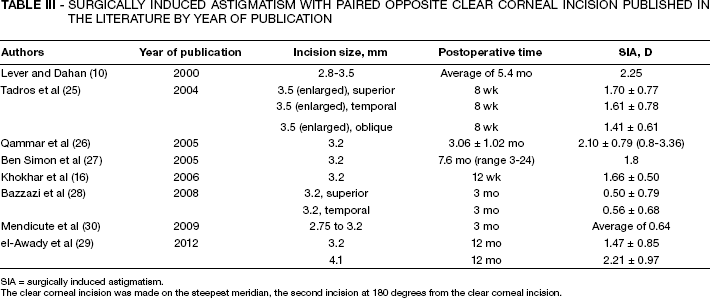
SIA = surgically induced astigmatism.
The clear corneal incision was made on the steepest meridian, the second incision at 180 degrees from the clear corneal incision.
As there is a well-known difference between the astigmatic effects of superior and temporal incisions (7–9), why such alterations have not been reported in the case of OCCI arises. Tadros et al (25) found that the astigmatic effect of superior, temporal, and oblique OCCI incisions showed no statistical difference, though a slightly higher SIA was detected in the case of superior incisions. In our study, the rate of induced astigmatism is independent of the location of the incision in the OCCI method. Further investigations should be carried out to explain the similarity in the rates of induced astigmatism detected in superior, oblique, and temporal OCCI incisions.
In summary, the paired OCCI method is a simple intervention without extra costs in cases where preoperative corneal astigmatism is between 1.0 and 1.5 D. It gives a relatively predictable result, practically independent of the location of the incision, which shows no significant change in the postoperative period.