
Abstract
Purpose
We evaluated the efficacy of sub-Tenon block in decreasing perioperative pain, incidence of intraoperative oculocardiac reflex (OCR), and postoperative nausea and vomiting (PONV) in pediatric squint surgery.
Methods
A total of 67 children age 2-12 years, American Society of Anesthesiologists Physical Status 1 and 2, were randomized to receive either sub-Tenon block (ST) in the operative eye or 2 mcg/kg of intravenous fentanyl (F) for squint surgery after induction of general anesthesia in this double-blind study. Postoperative pain was measured by either modified Children's Hospital of Eastern Ontario Pain Scale (CHEOPS) or Visual Analogue Scale (VAS). Pain in the postoperative period (up to 2 hours) was measured as the primary endpoint. Other parameters measured in the groups were intraoperative hemodynamics, postoperative modified CHEOPS or VAS at shifting, 1, 2, 6, 12, and 24 hours after surgery, incidence of intraoperative OCR, and PONV at shifting, 30 minutes, 1, 2, 6, 12, and 24 hours after surgery.
Results
There was no statistical difference in the postoperative pain scores in the recovery room up to 2 hours after surgery. The VAS and CHEOPS scores were not different in the groups up to 24 hours after surgery. The incidence of OCR was significantly higher in group F than group ST. The incidence of PONV was significantly higher in group F than group ST at 30 minutes and 1 hour after the surgery (41%, 47% vs 19%, 9%, respectively, p<0.05). However, there was no statistically significant difference in intraoperative hemodynamics and PONV scores after 2 hours in the postanesthesia care unit.
Conclusions
Use of sub-Tenon block does not decrease the incidence of postoperative pain significantly in children undergoing squint surgery. However, it leads to a statistically significant decrease in the incidence of intraoperative OCR and PONV in the early recovery period in these patients.
Keywords
Introduction
Squint surgery in children is usually associated with moderate to severe pain, depending on the number of muscles being corrected and the type of procedure. The mainstay of analgesia in the intraoperative and postoperative period is intravenous opioids along with nonsteroidal anti-inflammatory drugs (NSAIDs). Squint surgery is associated with high incidence of intraoperative oculocardiac reflex (OCR) and postoperative nausea and vomiting (PONV). Use of opioids can further aggravate both these complications associated with squint surgery. On the other hand, use of NSAIDs, especially in high doses, may be controversial in small children. Pain, nausea, and vomiting are undesirable in the postoperative period, as they will prolong postoperative recovery in children, many of whom are planned to have same-day procedures. Use of regional blocks as a supplement to general anesthesia decreases intraoperative and postoperative opioid requirement along with providing early recovery and early discharge readiness after various procedures (1). Use of peribulbar block has been shown to provide better intraoperative and postoperative analgesia, decrease the incidence of intraoperative OCR and PONV, and increase early discharge readiness in children undergoing various eye surgeries (2). However, side effects of peribulbar block, e.g., increased forward pressure, hypotonia of the eye, ophthalmic complications, which include globe perforation, retrobulbar hemorrhage, and optic nerve damage, and systemic complications like central neuraxial blockade and local anesthetic toxicity, although rare, may deter the use of peribulbar and retrobulbar block in children. Sub-Tenon block (STB), on the other hand, has been found to be much safer than the above mentioned blocks (3). Use of STB along with general anesthesia has been shown to be a safer and superior alternative to intravenous fentanyl in children undergoing cataract surgery under general anesthesia (4). However, their use has not been explored extensively in pediatric squint surgery under general anesthesia. The primary aim of this study was to assess if use of preoperative STB decreases the incidence of pain in the postoperative period in children undergoing squint surgery under general anesthesia. The secondary aim was to compare the incidence of intraoperative pain, OCR, and PONV with or without supplementation with STB.
Materials and Methods
After obtaining institutional ethical committee approval, 76 children were recruited after satisfying the inclusion criteria (age 2-12 years, American Society of Anesthesiologists [ASA] I or II physical status). Written informed consents were obtained from the parents. Preanesthetic checkup was done prior to surgery and children who were able to understand the Visual Analogue Scale (VAS) were made familiar with the scale, which was on a hard board with different shades of red. The score zero was equivalent to no pain and white on the scale while score of 10 was equivalent to maximum pain and deep red on the scale. Increasing score was equivalent to deepening color. We routinely use this scale in our postanesthesia care unit for assessment of pain in children. The children and their parents were not told about the group allocation. Allocation to groups was done based on a computer-generated random number placed in opaque, sealed envelopes opened just before induction of anesthesia.
Anesthesia was induced with incremental percentages of sevoflurane (5%-8%) in oxygen and nitrous oxide. Randomization and group allocation was done after securing intravenous access. Children allotted to group F received fentanyl 2 mcg/kg along with atracurium 0.3 mg/kg, while children allotted to group ST received only atracurium 0.3 mg/kg. Appropriate sized laryngeal mask airway (LMA) was inserted once jaw was adequately relaxed. Surgery was allowed to proceed. Sub-Tenon block was given to children in group ST by the operating surgeon. After cleaning and draping of the eye, a small conjunctival and limbal incision was made inferonasally and a short blunt metallic cannula was introduced through this aperture into the sub-Tenon space after dissection. Two to four milliliters of local anesthetic solution made with lignocaine 2% and bupivacaine 0.5% in 1:1 ratio was injected into this space. The observer anesthesiologist who was blind to the group allocation was called into the operation theatre at this time for further management of the case. Monitoring included recording of heart rate, blood pressure, SaO2, and EtCO2 every 1 minute after incision up to 5 minutes and every 5 minutes thereafter until the end of surgery. Ringer lactate was used as intravenous fluid intraoperatively and fasting and maintenance requirements were replaced adequately according to Segar formula (4 mL/kg for first 10 kg + 2 mL/kg for next 10 kg + 1 mL/kg for subsequent added body weight). Tachycardia or systolic hypertension (more than 20% of baseline), in response to incision, was treated with injection fentanyl, 1 mcg/kg, supplementation intravenously. The OCR was defined as fall in heart rate more than 10% than baseline or any abnormal rhythm on muscle handling. The surgeon was asked to leave the muscle on occurrence of OCR and 2 drops of 0.5% proparacaine were instilled in the eye. If the OCR recurred on restarting the surgery, intravenous injection of 10 mcg/kg of atropine was given. Any arrhythmias occurring on handling of the extraocular muscles was also recorded as OCR and was treated on same lines (i.e., by stopping the surgery and instilling 2 drops of 0.5% proparacaine). Total intraoperative use of fentanyl was recorded. Number of episodes of OCR and intervention done was noted. Ondansetron 0.1 mg/kg was administered intravenously to all patients. After completion of surgery, inhalational anesthetics were switched off and effect of residual muscle paralysis was reversed with intravenous neostigmine 50 mcg/kg and glycopyrolate 10 mcg/kg. The laryngeal mask airway (LMA) was removed after adequate respiratory efforts returned. Modified Aldrete score was assessed after removal of LMA. Modified Aldrete score was also assessed in the recovery unit and time at which modified Aldrete score became 10 was noted.
Postoperatively, pain was assessed by the anesthesiologist involved in the intraoperative management. All the children and their parents were also blinded to the group allocation.
Modified Children's Hospital of Eastern Ontario Scale (CHEOPS) was used to assess pain in patients who were younger than 7 years (5). In children older than 7 years and those who were able to comprehend VAS, pain was assessed by VAS scale. For children who were unable to point out the VAS score on the card, scoring was done by the anesthesiologist after asking them to look at the card and pointing at the appropriate score. Postoperative nausea and vomiting was scored as 0 for no nausea or vomiting, 1 for nausea without any vomiting or retching, 2 for 1 episode of vomiting in 30 minutes or severe retching, and 3 for ≥2 episodes of vomiting or severe retching in 30 minutes. Modified CHEOPS, VAS, and PONV scoring was done at 0, 0.5 hours, 1 hour, 2 hours, 6 hours, 12 hours, and 24 hours after shifting to the recovery. Up to 2 hours, if the pain score (either modified CHEOPS or VAS) was more than or equal to 4, intravenous fentanyl was given in appropriate doses. After 2 hours in recovery, analgesia was supplemented with oral ibuprofen in appropriate doses if required. Oral metoclopramide was used as rescue antiemetic.
Statistical analysis
Incidence of pain in the postoperative period in children undergoing squint surgery with opioid analgesia has been reported as 42% in a previous study from the same institute (6). We hypothesized that the incidence of pain will be less than 10% with use of STB. The sample size according to the Kelsey method with a power of 80% and an alpha error of 5% was calculated as 30 patients in each group. The statistical analysis was done by using Stata 11.0 (College Station, Texas, USA). The quantitative (nonparametric) data were analyzed by t test (data presented as mean ± standard deviation) or Wilcoxon rank-sum test (data presented as median [range]). Categorical (parametric) data were analyzed by chi-square test (data presented as number [%]). Fisher exact test was used wherever applicable. p Value less than 0.05 was taken as significant.
Results
The primary endpoint of the study was efficacy of STB for postoperative pain after squint surgery. A total of 30 children were intended to be recruited in each group. With a dropout rate expected of 20%, 76 children were initially recruited in the study after screening for inclusion criteria. Of the 38 children in the ST group, study protocol was not adhered to in 4 subjects as 2 mcg/kg of intravenous fentanyl was given inadvertently after securing IV access. Postoperative data collection from 3 patients in the ST group and 2 patients in the F group was incomplete as these patients were shifted to the ward before the study time period of 6 hours in the postanesthesia care unit. Final data analysis was done for 31 patients in the ST group and 36 patients in the F group (Fig. 1).
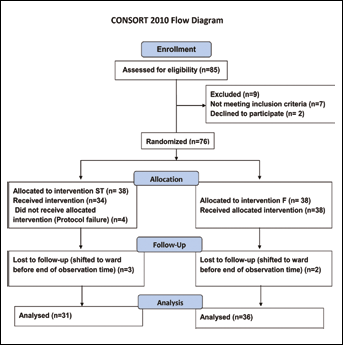
Flow of patients in the study.
The groups were matched demographically (Tab. I). The average age, weight, sex distribution, ASA status, number of muscles operated on, and duration of surgery was similar between the groups. Difference in incidence of pain in each group did not reach statistical significance at any time point (Tab. II). Number of patients requiring rescue analgesics was not significantly different in the groups (Tab. II). Intraoperative hemodynamics were also not significantly different in the groups at any time point. Use of intraoperative supplemental fentanyl was greater in group F but did not reach statistical significance (Tab. I). The incidence of PONV was significantly higher in patients of group F as compared to group ST at 1 hour (47% vs 9%, p<0.001) (Tab. III). The incidence of intraoperative OCR and use of intraoperative atropine was also significantly greater in group F as compared to group ST (p<0.001) (Tab. I). There was no difference in modified Aldrete score at reversal and time for children to reach Aldrete score of 10.
Demographic And Perioperative Data
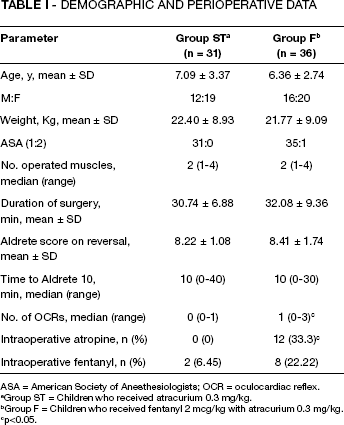
ASA = American Society of Anesthesiologists; OCR = oculocardiac reflex.
Group ST = Children who received atracurium 0.3 mg/kg.
Group F = Children who received fentanyl 2 mcg/kg with atracurium 0.3 mg/kg.
p<0.05.
Incidence Of Pain And Use Of Rescue Analgesics In The Postoperative Period
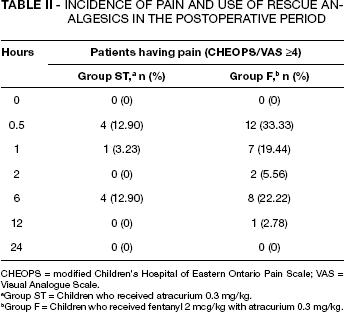
CHEOPS = modified Children's Hospital of Eastern Ontario Pain Scale; VAS = Visual Analogue Scale.
Group ST = Children who received atracurium 0.3 mg/kg.
Group F = Children who received fentanyl 2 mcg/kg with atracurium 0.3 mg/kg.
Incidence Of Ponv
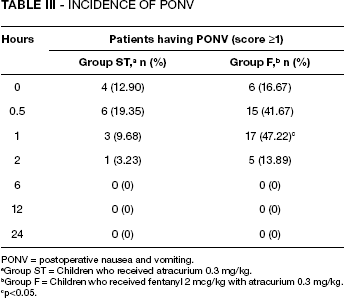
PONV = postoperative nausea and vomiting.
Group ST = Children who received atracurium 0.3 mg/kg.
Group F = Children who received fentanyl 2 mcg/kg with atracurium 0.3 mg/kg.
p<0.05.
Discussion
The main purpose of this study was to evaluate if preincision STB provides superior analgesia as compared to intravenous fentanyl when used for children undergoing squint surgery. The study failed to prove the hypothesis that STB will provide superior analgesia over intravenous fentanyl. Perioperative pain management in children is marred by many factors. This patient population is different not only in their expression of pain but also in the complex assessment of their pain, which is confounded by other perioperative factors such as absence of parents, hunger, and unfamiliar surroundings. Conventional pain management techniques for postoperative analgesia in adults are used restrictively in children. Opioids are used sparingly for fear of respiratory depression and sedation. Opioids may also exaggerate PONV, especially in children undergoing squint surgery. Use of acetaminophen and NSAIDs is the second line of choice. Acetaminophen, although found safe in children, may not be adequate for severe postoperative pain, and ibuprofen, the most commonly used NSAID, has better analgesic efficacy but its use may be associated with hypersensitivity reactions, gastrointestinal symptoms, and renal insufficiency (7). Over the past few decades, regional analgesia has increasingly been used for postoperative analgesia in children. Various modalities of regional analgesia, i.e., central neuraxial anesthesia, peripheral nerve blocks, and plexus blocks, have been proven to decrease postoperative pain, opioid consumption, hospital stay, and other morbidities in various surgeries. Ophthalmic blocks, however, are underused for postoperative analgesia in children. Many reasons for this can be postulated. First, in many countries anesthesiologists are poorly versed with various ophthalmic blocks, thus depending on surgeons to perform them, who may deem it unnecessary under general anesthesia (8). Secondly, the conventional retrobulbar and peribulbar blocks are associated with risk of rare but definite ocular and systemic complications. Finally, the postoperative period in these patients is associated with other complications such as agitation, nausea, vomiting, and sedation, which may have priority over pain in management strategies. However, a recent updated report by the ASA Task Force on Acute Pain Management states that aggressive and proactive pain management is necessary to overcome the historic undertreatment of pain in children and regional blockade with local anesthetics should always be considered wherever possible (9). The STB was chosen in this study as it has one of the highest safety profiles of any ophthalmic regional anesthetic technique and provides effective intraoperative and postoperative analgesia (10). In our study, however, there was no statistically significant difference in the incidence of pain in the intraoperative and the postoperative period. One reason for this insignificant difference in analgesia could be the high incidence of emergence delirium in children undergoing squint surgery under general anesthesia with sevoflurane (11). Subjective pain assessment tools like the modified CHEOPS may not be able to differentiate emergence delirium from postoperative pain (12), thus potentially increasing the incidence of pain in the study group receiving STB as well. Morris et al (13) found similar results in their study involving 54 children aged 1-16 years. They found that postoperative mean pain scores were similar in children receiving or not receiving preoperative STB with levobupivacaine. All the children in their study groups received preoperative diclofenac and paracetamol. No intraoperative opioids were used in either of the groups, with some patients receiving remifentanil only at induction of anesthesia. The mean pain scores in the postoperative period were not statistically different in either of the groups at any observation point. Steib et al (14), however, found a decrease in both intraoperative and postoperative analgesic consumption in 19 children aged 2.5-6 years who received STB with 0.5% bupivacaine at the start of surgery. They also found a significant decrease in number of episodes of OCR and PONV in children who received the block. On the other hand, Sheard et al (15) used sub-Tenon lignocaine in 111 patients under the age of 15 years undergoing squint surgery under general anesthesia and did not find any decrease in requirement of systemic analgesic in the postoperative period in children who received the block. Children who received the block in their report, however, did experience significantly less pain immediately at the start of the postoperative observation period, but the later time points did not show this difference. Thus the previous few studies are equivocal regarding the postoperative analgesic efficacy of STB in patients undergoing squint surgery under general anesthesia.
We found a significant decrease in the incidence of PONV in patients who received block up to 2 hours in the recovery period. Steib et al (14) have also reported this positive effect of STB in their study. Morris et al (13), however, did not find any difference in the incidence of PONV in their study, although their report does not mention the type and dose of antiemetic used in children who underwent surgery. We used 100 mcg/kg of ondansetron in our study before start of surgery. Incidence of PONV with ondansetron as sole antiemetic is variously reported as between 30% (16) and 58% (17) with the dose used by us (100 mcg/kg). Combination antiemetic therapy is known to reduce incidence of PONV more effectively than ondansetron alone (18). Postoperative nausea and vomiting is known to be reduced after peribulbar block and topical instillation of local anesthetic drops as well in children undergoing squint surgery (19). The decrease in PONV after regional anesthetic block is probably related to suppression of afferents carried via the trigeminal nerve (20). Similarly, a decrease in the incidence of intraoperative OCR as was seen in this study and reported in previous studies may also be related to suppression of afferent arm of trigeminovagal reflex by the STB (14).
Sub-Tenon block has been associated with lesser minor and major complications (21). However, vision-threatening complications like orbital and retrobulbar hemorrhage, scleral perforation, damage to the inferior and medial rectus muscles, optic neuropathy, and retinal and choroidal vascular occlusion have been reported with this block, and life-threatening complications like cardiorespiratory arrest due probably to subarachnoid spread through optic nerve sheath has been reported (22). Some ophthalmologists may have reservations regarding use of local anesthetics as this can lead to myotoxicity, leading to muscle fibrosis (23). In conclusion, use of STB did not provide better analgesia as compared to intravenous fentanyl in children undergoing squint surgery under general anesthesia. Preoperative STB as compared to intravenous fentanyl decreased incidence of intraoperative OCR and PONV in the early recovery period.
Our study may have been limited by the fact that a placebo control was not used in either of the groups.