
Abstract
Purpose
To evaluate the effects of yellow micropulse laser in eyes with diabetic macular edema (DME).
Methods
In this retrospective interventional case series, 22 eyes of 17 patients with visual impairment secondary to persistent DME received one single session of yellow micropulse laser. Patients were divided into 2 groups: group 1, naive eyes; and group 2, previously treated eyes. Main outcome measures included changes in central retinal thickness (CRT) and best-corrected visual acuity (BCVA). Possible atrophic changes of the retinal pigment epithelium as a result of yellow micropulse laser application were evaluated with fundus autofluorescence.
Results
At baseline, the mean logMAR BCVA was 0.39 ± 0.18 and the mean CRT was 361.8 ± 70.95. The mean BCVA improved to 0.31 ± 0.19 (p = 0.0091) and 0.31 ± 0.19 (p = 0.0078) at 3 and 6 months of follow-up, respectively. The mean CRT improved to 331.3 ± 48.46 (p<0.0001) and 328.1 ± 53.25 (p<0.0001) at 3 and 6 months of follow-up. Subgroup analysis showed that only in naive eyes was there a beneficial effect on visual acuity and central macular thickness.
Conclusions
In eyes with DME, yellow micropulse laser produces a statistically significant improvement in BCVA and CRT in the short term.
Introduction
Diabetic macular edema (DME) is a major cause of central vision impairment in persons with diabetic retinopathy and can occur at any stage of the disease (1). To date, the most widely accepted method to treat visual impairment secondary to DME is intravitreal injection of ranibizumab, as reported by the RESTORE and DRCRnet studies (2, 3), which demonstrated that ranibizumab monotherapy provided superior visual acuity gain over standard focal/grid laser photocoagulation in patients with visual impairment due to DME.
Despite the advent of new pharmacologic agents able to restore visual acuity, little has changed in the protocols of photocoagulation for the visual impairment secondary to DME originally proposed by the Early Treatment Diabetic Retinopathy Study (ETDRS) (4). Focal/grid photocoagulation administered with its laser-induced thermal retinal destruction remains the standard treatment modality that has been demonstrated to modify the production of vasoactive cytokines including vascular endothelial growth factor (VEGF) (5-8). On the other hand, conventional photocoagulation is associated with a number of risks and adverse events (macular scotomas, damage of photoreceptors, enlargement of laser retinal scars, choroidal neovascularization, and subfoveal fibrosis) (9-13), which led researchers to explore less aggressive, i.e., “mild” or “light” laser treatment strategies with comparable results to the modified ETDRS procedure (14-21). However, although mild or light barely visible laser applications are less destructive, they still cause irreversible damage to the photoreceptors, which results in a reduction of retinal sensitivity similar to that of the standard modified ETDRS photocoagulation (14).
Better understanding of cellular and molecular changes inducible with laser exposures and advances in laser technology are contributing to a paradigm shift in laser treatment strategies from destructive threshold photocoagulation with continuous wave (CW) lasers to nondamaging subthreshold photostimulation with micropulse emitting lasers (21). Unlike in conventional photocoagulation, where the CW laser energy is adjusted to cause a rapid temperature rise that spreads and produces the visible white inner retina burn endpoint, in subthreshold photostimulation with micropulse laser emission technique, the photothermal effects are finely controlled and confined at the retinal pigment epithelium (RPE) level, and the train of repetitive micropulses allows the user to consistently perform therapeutically effective tissue-sparing treatments in the absence of visible burn endpoints (21). So far, most randomized controlled clinical trials comparing the treatment of eyes with DME with standard CW laser threshold photocoagulation versus subthreshold treatment with micropulse lasers have been conducted using the 810-nm infrared micropulse laser (IR-MPL), which has been reported to be safe and at least as effective as the standard of care (17-21). Recently, other laser wavelengths became available with the micropulse emission mode, including the 577-nm yellow wavelength (22). The principal aim of this study was to determine functional and morphologic short-term changes after 577-nm yellow micropulse laser (Y-MPL) treatment in eyes with center-involving DME.
Patients and Methods
This study was a retrospective case series carried out at the University Eye Clinic of Genova, Italy. The Institutional Review Board of the University of Genova approved the study protocol and the collection of data. The data collection complies with Italian law. The study was conducted in accordance with the provisions stated in the Declaration of Helsinki. All patients signed written informed consent. All patients with visual impairment secondary to DME were recruited from May 2012 to March 2013. Patients were proposed to enter the study if they did not sufficiently respond to standard anti-VEGF therapy or to standard focal/grid laser photocoagulation or if they were unwilling to undergo at least 3 monthly intravitreal injections. Eligibility criteria included a diagnosis of either type I or type II diabetes mellitus; the presence of macular edema was documented by biomicroscopy and contact lens examination and confirmed by spectral-domain optical coherence tomography (SD-OCT) and fluorescein angiography. Exclusion criteria included evidence of macular ischemia defined as angiographic evidence of more than 6 clock hours of macular capillary nonperfusion and tractional macular edema judged to be the primary cause of the edema. Other exclusion criteria included a history of vitrectomy, a history of cataract surgery, or any other intraocular surgery within 3 months before the study entry. Eyes were excluded if previously treated for macular edema (including sub-Tenon injection of triamcinolone, intravitreal injection of any drugs, or macular laser photocoagulation) within 6 months before the study entry. Best-corrected visual acuity (BCVA) was measured at baseline and 3 and 6 months by certified examiners using ETDRS charts and quantified in logMAR units. Central retinal thickness (CRT) was measured using a SD-OCT machine (Topcon 3D OCT-2000) by way of the 12 radial scan protocols at baseline and 3 and 6 months. Fundus autofluorescence (F) (Topcon Spaide AF filters) was performed at baseline and follow-up visits in order to evaluate possible atrophic changes of the RPE.
Eyes were also divided into 2 groups: naive eyes (group 1) and previously treated eyes (group 2).
After mydriasis with tropicamide (1%) and topical anesthesia with Benoxinate (0.4%) eyedrops, an area centralis contact lens (Volk Optical, Mentor, Lake, Ohio, USA) was applied. The 577-nm yellow laser (OcuLight SLx, Iridex Corp., Mountain View, California, USA) was used. Treatment parameters were standardized to a spot size of 200 μm, exposure duration of 0.2 s, power at 200 mW in micropulse emission with a duty cycle of 5%. Once the subthreshold treatment parameters were set, a variable number of confluent high-density exposures were applied depending on the extension of the edema (on average between 250 and 450 spots). The primary outcome measures for the study were mean variation of the CRT and BCVA at 3 and 6 months compared to baseline. Secondary outcome measure was any evidence of RPE damage at autofluorescence.
Results
Overall, a total of 22 eyes of 17 patients (11 male, 6 female; mean age 62 years, range 45–76 years) were included in the analysis. The mean duration of DME was 39.4 months (range 21–82 months) and the mean HbA1c value at baseline was 7.9%. Five eyes were previously treated with anti-VEGF drugs and focal/grid laser photocoagulation, 5 eyes were treated with anti-VEGF drugs only, and 12 eyes were naive. At baseline, the mean logMAR BCVA was 0.39 ± 0.18 and improved to 0.31 ± 0.19 (p = 0.0091) and 0.31 ± 0.19 (p = 0.0078) at 3 and 6 months of follow-up, respectively. At baseline, the mean CRT was 361.8 ± 70.95 μm and improved to 331.8 ± 48.46 (p<0.0001) and 328.1 ± 53.25 (p<0.0001) at 3 and 6 months of follow-up. Optical coherence tomography, color fundus photograph, and F did not show atrophic changes of the RPE (Fig. 1). None of the patients complained of scotoma or had evidence of laser spots, scars, or any other macular complications attributable to Y-MPL. At baseline in group 1 (n = 12), the mean logMAR BCVA was 0.39 ± 0.19 and improved to 0.27 ± 0.18 (p = 0.027) and 0.27 ± 0.17 (p = 0.0187) at 3 and 6 months of follow-up, respectively. At baseline, the mean CRT in group 1 was 350.9 ± 74.7 μm and improved to 319.4 ± 51.43 (p = 0.0030) and 311.2 ± 49.43 (p = 0.0108) at 3 and 6 months of follow-up. At baseline in group 2 (n = 10), the mean logMAR BCVA was 0.38 ± 0.18 and improved to 0.36 ± 0.20 (p = 0.3) and 0.38 ± 0.20 (p = 0.9) at 3 and 6 months of follow-up, respectively. At baseline, the mean CRT in group 2 was 369.2 ± 66.81 μm and improved to 342.4 ± 41.97 (p = 0.05) and 341.6 ± 54.83 (p = 0.04) at 3 and 6 months of follow-up.
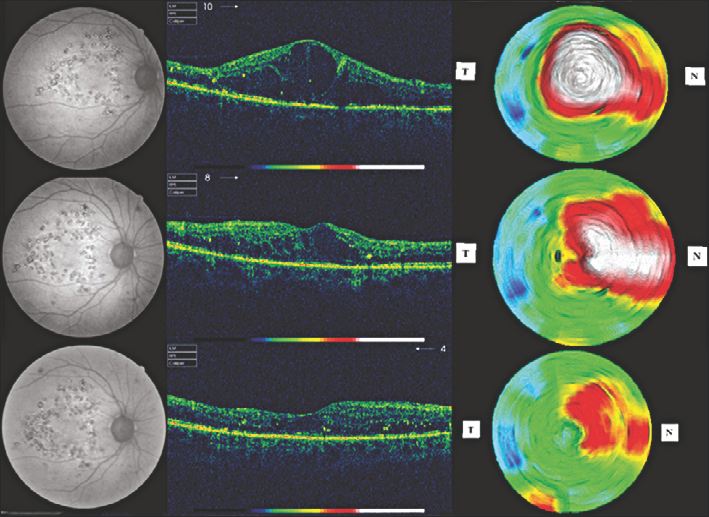
Diabetic macular edema at baseline (upper-line), 3 (middle-line) and 6 (bottom-line) months after yellow micropulse laser. At baseline autofluorescence (upper-line, left), OCT b-scan (upper-line center) and thickness map (upper line right) show significant edema with grid laser photocoagulation scars. At 3 and 6 months autofluorescence (middle-line and bottom-line left) did not show any further damage of the RPE while OCT b-scan (middle-line and bottom line, center) and thickness map (middle-line and bottom-line right) show a significant decrease of the edema.
Discussion
The results of this study show that treatment with the 577-nm Y-MPL is effective in terms of stabilization or improvement of vision and reduction or resolution of DME, at least in the short term. Subgroup analysis showed that naive eyes might respond better than previously treated eyes.
Several clinical trials have demonstrated the safety and efficacy of subthreshold treatment with IR-MPL (16-22), but little is known about the use of Y-MPL in DME (22). The 577-nm wavelength from the optically pumped semiconductor laser is well absorbed in melanin and has a specific high absorption coefficient peak in oxyhemoglobin (HbO). Conversely, the 810-nm diode laser's wavelength is practically absorbed only by melanin and with a lower absorption coefficient with respect to shorter visible wavelengths.
Both 577-nm and 810-nm wavelengths can reach the ocular fundus almost unaffected by ocular media opacity and by retina thickness, by virtue of their negligible scattering compared to blue and green laser wavelengths. Furthermore, these wavelengths are not absorbed by macular pigments and, more importantly, by xanthophyll, which is located in the inner and outer plexiform layers where thermal damage is undesirable (23).
The 810-nm infrared beam interacts with the melanin in the RPE and with the melanocytes in the choroid, producing deep photothermal effects. The 577-nm yellow beam interacts with the melanin in the RPE and whatever energy can pass through the RPE layer is strongly absorbed by the oxyhemoglobin in the immediately underneath choriocapillaries, with thinner photothermal effects confined to the RPE–choriocapillaries complex. This “2 layers–2 chromophores” absorption has important and reassuring positive implications for the surgeon performing subthreshold treatments without a visible endpoint feedback, because the combined absorption in the RPE–choriocapillaries complex, with an RPE layer with variable melanin distribution and a choriocapillaries layer with homogeneously distributed oxyhemoglobin, gives to the 577-nm wavelength the theoretical advantage of producing more uniform and consistent invisible photothermal effects across the whole retinal fundus.
The morphologic advantage of Y-MPL is the absence of visible scars, whereas the functional advantages include the absence of scotomas and preservation of color vision and contrast sensitivity. In a recent report, Y-MPL was compared with IR-MPL from both a morphologic and functional point of view in DME at 5% duty cycle. The results of this study confirmed that the safety of both yellow and infrared micropulse laser treatments is comparable (22). In our case series, all eyes were treated with the same fixed dose emission and did not show any visible or otherwise detectable sign of laser-induced RPE damage at ophthalmoscopy and autofluorescence. Subgroup analysis revealed that naive patients maintained a statistically significant increase in BCVA and decrease in CMT at 3 and 6 months compared to previously treated eyes. We can speculate that in our case series BCVA and CMT variations are not influenced by possible late effect of anti-VEGF or grid laser photocoagulation.
We found it difficult to rely on laser energy parameters administered without the comfort of an ophthalmoscopically visible endpoint confirming the adequacy of the treatment, but were rewarded by the clinical responses, which indicate an unexpectedly wide effective therapeutic window.
A limitation of the study is that it involved a small, retrospective, and not randomized sample size with a short follow-up. Nonetheless, this study offers useful outcome data of this form of treatment for DME. These data should be used for future randomized studies done to assess whether this technology can be used routinely in clinical practice.