
Abstract
Purpose
We investigated the clinical staging and management of cataracts to decrease the incidence of complications of phacoemulsification and improve the postoperative visual function of patients with exfoliation syndrome (XFS) with cataract.
Methods
Cataracts with XFS were divided into early, middle, and late stages using the Emery-Little lens opacities classification system. Phacoemulsification and intraocular lens (IOL) implantation were performed in all eyes. The incidences of intraoperative and early postoperative complications of phacoemulsification were compared, and differences in the outcomes of phacoemulsification were evaluated.
Results
There were 23, 31, and 34 eyes with early-, middle- and late-stage XFS, respectively. The mean ultrasound time, cumulative dissipated energy, and incidence of moderate to severe corneal edema and wound burn in the late-stage group were significantly higher than in the early- and middle-stage groups (p<0.05). The incidence of zonular dehiscence, capsular rupture, vitreous loss, and iritis were not significant among the 3 groups (p>0.05). Intraocular pressure rise in the early postoperative period and the level of optic atrophy in the late-stage group were significantly higher than in the other 2 groups (p<0.05). The gain in visual acuity in the early- and middle-stage groups after surgery was better than in the late-stage group of XFS, and the difference was statistically significant (p<0.05).
Conclusions
The clinical staging of cataract with XFS contributed to the choice of operation time and its management. Phacoemulsification and IOL implantation in early- and middle-stage XFS induced fewer complications and led to better recovery of visual function after surgery.
Introduction
Exfoliation syndrome (XFS) is an age-related disorder of the extracellular matrix in which abnormal fibrillar material is produced and progressively accumulates in tissues throughout the anterior segment and in the connective tissues of various viscera (1, 2). Clinically, the abnormal fibrillar material and the connective tissue lesions of XFS lead not only to severe chronic open-angle glaucoma but also to acceleration of cataract formation, lens subluxation, and angle-closure glaucoma (2–4). It is well known that eyes with XFS are at higher risk for developing cataract (5, 6). The clinical features of this kind of XFS-related cataracts are a hard nucleus, zonular weakness, and poor pupil dilation. Cataract surgery in the presence of XFS is associated with a greater number of complications. For example, many studies reported that it was associated with an increased risk of intraoperative and postoperative complications, such as zonular dialysis, vitreous loss, prolonged corneal edema, sustained inflammatory reaction, and lens decentration (7–11). Recent studies performed by experienced surgeons of the risk of complications in XFS in cataract surgery have shown a lower rate compared with earlier studies, which found up to a 10-fold increase (12–15). The decrease is due to development of phacoemulsification and the use of a combination of appropriate devices, technologies, and approaches. In the aforementioned studies, the overall outcomes for patients with XFS undergoing cataract surgery were similar to those of non-XFS patients. However, these studies included patients with different levels of nuclear density of cataracts with XFS. Exfoliation syndrome is a progressive disease, which worsens with age. With increasing age, zonular dialysis and the hardness of the nucleus increase. Theoretically, the degree of nuclear density in cataracts influences the incidence of intraoperative and postoperative complications of phacoemulsification.
In order to decrease the incidence of complications of phacoemulsification and improve the postoperative visual function of patients with XFS with cataract, there is an urgent need to develop a standard staging method of XFS and an appropriate window phase on cataract surgery. To our knowledge, there have been no published studies on this so far.
Our primary goal was to investigate the staging of cataracts with XFS based on clinical features. Our secondary goal was to compare the incidence of intraoperative and early postoperative complications of phacoemulsification in different clinical stages of cataracts with XFS, excluding eyes with glaucoma and zonule instability, such as lens subluxation, zonule dialysis, iridodonesis, and phacodonesis. In addition, differences in visual acuity and intraocular pressure (IOP) following phacoemulsification in different clinical stages of cataracts with XFS were evaluated.
Methods
All eyes from August 1, 2012, to December 31, 2013, underwent a preoperative examination, including measurement of visual acuity, IOP, and A- and B-scan biometry. Detailed slit-lamp biomicroscopy under maximal mydriasis was performed. The presence of XFS, the grade of cataract, and iridodonesis, phacodonesis, and zonulysis were noted. A detailed fundus examination was conducted. Exfoliation syndrome eyes with glaucoma and zonule instability, such as lens subluxation, zonule dialysis, iridodonesis, and phacodonesis, were excluded. The study group consisted of XFS eyes without coexisting ocular disease, previous ocular surgery, or trauma. The research followed the tenets of the Declaration of Helsinki and was approved by the Ethics Committee of the Eye and ENT Hospital of Fudan University. Informed consent was obtained from all patients.
Diagnostic criterion of XFS
The diagnostic criterion of XFS (1, 9, 16) was the existence of exfoliation material on the anterior lens capsule or on the pupil margin in either eye with dilation of the pupils. Patients with IOP less than 21 mm Hg and no clinical evidence of glaucomatous optic neuropathy were classified as having XFS.
Clinical staging of cataracts with XFS
Cataracts with XFS was divided into 3 stages–-early, middle, and late–-using the Emery-Little lens opacities classification system. The pseudoexfoliation deposits on the crystalline lens and iris under slit-lamp biomicroscopy were also assessed. Early-stage cataracts with XFS had grade II nucleus opacity and mild pseudoexfoliation deposits on the crystalline lens and pupillary margin (Fig. 1). Twenty-three eyes were classified and included in this group. Middle-stage cataracts with XFS had grade III nucleus opacity and middle pseudoexfoliation deposits on the crystalline lens and pupillary margin (Fig. 2). Thirty-one eyes were classified and included in this stage. Late-stage cataracts with XFS had grade IV to V nucleus opacity and severe pseudoexfoliation deposits on the crystalline lens and pupillary margin (Fig. 3). Thirty-four eyes were classified and included in this group.

Early-stage cataracts with exfoliation syndrome: grade II nucleus opacity and mild pseudoexfoliation deposits on the crystalline lens and pupillary margin under slit-lamp biomicroscopy.
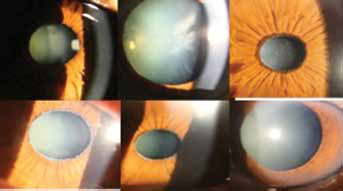
Middle-stage cataracts with exfoliation syndrome: grade III nucleus opacity and medium pseudoexfoliation deposits on the crystalline lens and pupillary margin under slit-lamp biomicroscopy.
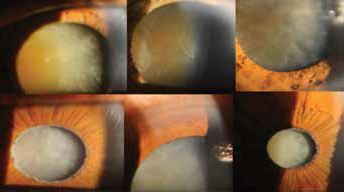
Late-stage cataracts with exfoliation syndrome: grade IV to V nucleus opacity and severe pseudoexfoliation deposits on the crystalline lens and pupillary margin under slit-lamp biomicroscopy.
Operation techniques
All surgeries were performed under topical anesthesia by the same surgeon (Y. Jiang). A 2.6-mm superior or superior temporal clear corneal tunnel incision was used. A 0.9-mm-wide paracentesis was carried out for the insertion of the chopper. Subsequently, Duovisc (Alcon Laboratories, Fort Worth, Texas, USA) was used to maintain the anterior chamber, and continuous curvilinear capsulorhexis and hydrodissection were performed. Endocapsular phacoemulsification of the nucleus with the phaco chop or straight phaco chop technique and cortical aspiration were performed using an Infiniti phacoemulsifier (Alcon Laboratories) (17, 18). The anterior chamber and the capsular bag were refilled with Duovisc. A standard capsular tension ring (Morcher GmbH, Stuttgart, Germany) was inserted into the capsular bag in patients with a high risk of zonule instability. A foldable intraocular lens (IOL) was implanted into the capsular bag using an injector cartridge system. The residual viscoelastic material was removed using an irrigation/aspiration handpiece. Balanced salt solution was injected through the paracentesis to maintain the anterior chamber. At the end of the surgery, the wound was checked and found to be watertight. In cases with posterior capsular rupture and vitreous loss, a 3-piece foldable acrylic IOL was implanted in the sulcus after anterior vitrectomy. Postoperatively, all the patients were treated with topical 0.1% Tobradex (Alcon Laboratories) and 0.1% Pranoprofen (Sumika Finechem, Osaka, Japan) 4 times a day for 1 month, followed by weekly tapering. In cases of elevated IOP (IOP ≥22 mm Hg), timolol maleate (0.5%) eyedrops 2 times daily were added to this regimen.
Examination
Pupil size was obtained by the surgeon using a sterile stainless steel ruler under a surgical microscope. Intraoperative and early postoperative complications (3 days after cataract surgery), postoperative visual acuity, and IOP values were noted for each eye. Postoperative intraocular inflammation was defined as +1, +2, +3, or +4 according to the number of cells in the anterior chamber region visualized by a light slit 1 mm in width and 3 mm in height.
Statistical analysis
The statistics were performed using STATA 10.0 (Stata Corp., College Station, Texas, USA) statistical software. The one-way analysis of variance Scheffe test, χ 2 test, and non-parametric Kruskal-Wallis test were used to analyze the variables studied. A p value <0.05 was considered statistically significant.
Results
Eighty-eight eyes (86 patients) were diagnosed with XFS (22 women and 64 men). The mean (± SD) age was 75 ± 8.17 (range 58–100 years). A total of 23, 31, and 34 eyes were classified as early-, middle-, and late-stage XFS, respectively. Phacoemulsification was applied to the right eye in 40 eyes, to the left eye in 48 eyes, and to both eyes in 2 patients. Differences in age among the 3 groups were not statistically significant (p>0.05, Kruskal-Wallis test). The main results for the eyes in the 3 groups are shown in Table I.
Results for the eyes in the 3 groups
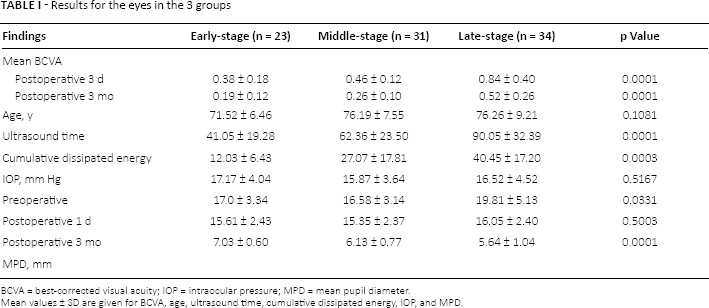
BCVA = best-corrected visual acuity; IOP = intraocular pressure; MPD = mean pupil diameter.
Mean values ± SD are given for BCVA, age, ultrasound time, cumulative dissipated energy, IOP, and MPD.
The mean (± SD) best-corrected visual acuity (BCVA) (log-MAR acuity) 3 days and 3 months after the surgery in the early- and middle-stage groups was higher than that in the late-stage group of XFS, and the difference was statistically significant (p>0.05, Kruskal-Wallis test). The mean (± SD) ultrasound time and mean cumulative dissipated energy in the early- and middle-stage groups were lower than those in the late-stage group of XFS, and the difference was statistically significant (p<0.05, Kruskal-Wallis test). The mean (± SD) preoperative and postoperative IOP of the groups 3 months after the surgery was not significantly different (p>0.05, Scheffe test). However, the mean (± SD) IOP on the first day after the surgery in the early- and middle-stage groups was lower than that in the late-stage group of XFS, and the difference was statistically significant (p<0.05, Scheffe test).
After maximal mydriasis, the mean (± SD) pupil diameter was 7.03 ± 0.60 mm, 6.13 ± 0.77 mm, and 5.64 ± 1.04 mm in the early-, middle-, and late-stage group, respectively. The differences in the pupil diameter among the 3 groups were statistically significant (p<0.05, Kruskal-Wallis test). A pupil diameter of 4 mm or less was observed in 0 eyes, 1 eye, and 6 eyes in the early-, middle-, and late-stage groups, respectively, and this finding was statistically significant (p<0.05, χ 2 test).
Intraoperative and early postoperative complications are shown in Table II. No zonular dehiscence was observed in the early-stage group. Zonular dehiscence was observed in 2 eyes in the middle-stage group and in 4 eyes in the late-stage group. It was less than 90°. In-the-bag implantation of a capsular tension ring (CTR) and foldable IOL could be performed in all eyes. Lens decentration was not observed in any eye in the 3 groups in the early postoperative period.
Intraoperative and early postoperative complications in the 3 groups
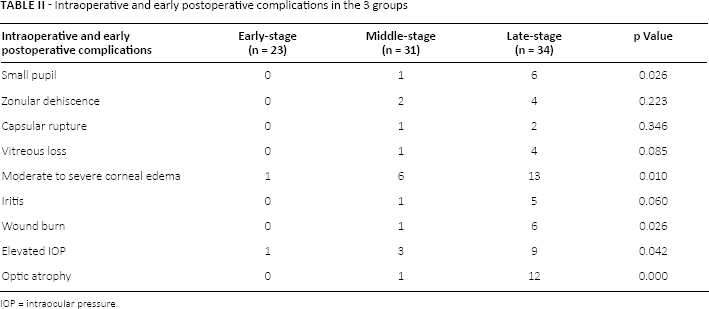
IOP = intraocular pressure.
Capsular rupture was observed in 0 eyes, 1 eye, and 2 eyes in the early-, middle-, and late-stage groups, respectively. Vitreous loss was observed in 0 eyes, 1 eye, and 4 eyes in the early-, middle-, and late-stage groups, respectively. Anterior vitrectomy was performed in capsular rupture and vitreous loss eyes. A 3-piece foldable acrylic IOL was implanted in the sulcus in all these eyes. Nucleus drop was not observed in any eye in the 3 groups. The incidence of zonular dehiscence, capsular rupture, and vitreous loss among the 3 groups was not statistically significant (p>0.05, χ 2 test).
Moderate to severe corneal edema was seen in 1 eye, 6 eyes, and 13 eyes in the early-, middle-, and late-stage groups, respectively. Wound burn was seen in 0 eyes, 1 eye, and 6 eyes in the early-, middle-, and late-stage groups, respectively. The difference in the incidence of moderate to severe corneal edema and wound burn among the 3 groups was statistically significant (p<0.05, χ 2 test). Iritis was seen in 0 eyes, 1 eye, and 5 eyes in the early-, middle-, and late-stage groups, respectively, which was not statistically significant (p>0.05, χ 2 test).
The number of eyes with an IOP>21 mm Hg was 1 eye, 3 eyes, and 9 eyes in the early-, middle-, and late-stage groups, respectively. The difference in the number of eyes with an IOP>21 mm Hg was statistically significant (p<0.05, χ 2 test). More eyes had an IOP above normal limits in the early postoperative period of the late-stage group. Optic atrophy was seen in 0 eyes, 1 eye, and 12 eyes in the early-, middle-, and late-stage groups, respectively, which was statistically significant (p<0.05, χ 2 test).
Discussion
According to worldwide studies, there is evidence showing that genetic factors may play an important role in the pathogenesis of XFS (19, 20). The Uygur population in Xinjiang is more susceptible to this disease than other ethnic groups (16). We recruited Uygur patients from Kashi, located in the south of the Tianshan Mountains, where the residents are mainly Uygur. Epidemiologic studies have shown that the prevalence of XFS is 5.1% in the Kashi Uygur (21). Although the incidence of XFS is known to increase with age, no significant difference was found with age among our early-, middle-, and late-stage groups. In the present study, 72.73% of the patients in the XFS group were men. This finding is similar to that reported by Akinci et al (22) in Turkey. All our patients were farmers, whose main production activity was outdoor sheep farming. It is highly likely that, together with genetic factors, environmental factors, such as extended periods spent in the sunshine, may play an important role in the pathogenesis of cataracts with XFS.
Due to poor economic conditions, lack of medicine, and unawareness of the disease, patients with XFS in Kashi do not tend to seek medical treatment until they have almost lost their visual acuity. Severe cataract is the most common cause of blindness. Phacoemulsification in cataract treatment is an efficient and safe procedure. It improves patients’ visual acuity and results in a low number of postoperative complications (23–25). However, severe cataract with XFS is always accompanied by poor pupil dilation, zonulopathy, and glaucoma. Consequently, the incidence of intraoperative and postoperative complications of phacoemulsification greatly increases. Deciding how best to decrease the incidence of intraoperative and postoperative complications of phacoemulsification is a common problem faced by surgeons. The intraoperative and postoperative complications of phacoemulsification in soft cataracts are less than those in hard cataracts. Therefore, the first step is clinical staging of cataracts with XFS. As the complications of phacoemulsification in early- and middle-stage cataracts with XFS are less than those in late-stage cataract, it is advisable to perform phacoemulsification in the early and middle stages of the disease.
Studies reported that eyes with XFS have a significantly greater prevalence of nuclear cataract than eyes without XFS (22, 26). In the present study, nuclear cataracts with XFS were divided into early, middle, and late stages using the Emery-Little lens opacities classification system. Phacoemulsification and IOL implantation were performed in all cataracts with XFS in this study. The ultrasound time and the dissipated energy in the late-stage group were significantly higher than those of the other 2 groups. Consequently, the incidence of moderate to severe corneal edema and wound burn in the late-stage group was higher than in the other 2 groups. In other studies, XFS did not have a negative influence on endothelial cell loss, but XFS in cases of high phaco impact significantly increased the risk of endothelial cell loss (7, 24).
Poor pupil dilation is one of the most common problems in cataract surgery in eyes with XFS (22, 23). Eyes with XFS are almost always characterized by insufficient mydriasis. The mean pupil diameter in the late-stage group was significantly smaller than that in the early- and middle-stage groups in our study. The numbers of pupils less than 4 mm were significantly greater in the late-stage group than in the early- and middle-stage groups. To dilate the pupils, sphincterectomies or iris retraction hooks were performed and applied to the patients with miosis of 4 mm or less. There was no difficulty in performing anterior continuous curvilinear capsulorhexis in any eye.
The incidence of zonular dehiscence, capsular rupture, vitreous loss, and iritis in the late-stage group was not significantly higher than that in the early- and middle-stage groups.
A higher risk of ocular hypertension after cataract surgery in eyes with XFS has been reported. This was due to more severe inflammation after cataract surgery in eyes with XFS due to pathologic iris vessels with increased permeability for proteins (27). The rise in IOP 1 day after phacoemulsification was significantly higher in the late-stage group than in the early- and middle-stage groups. The number of eyes with an IOP>21 mm Hg in the late-stage group was also significantly higher than in the early- and middle-stage groups. Yet in our study, the number of eyes with intraocular inflammation was not significantly higher. We speculate that the thickness of the cornea resulting from moderate to severe corneal edema is one explanation for the high IOP. It is easy to control high IOP with the administration of antiglaucoma drugs. Postoperatively, the IOP was not significantly different among the 3 groups after 3 months.
The numbers of eyes with optic atrophy (0 eyes, 1 eye, and 12 eyes in the early-, middle-, and late-stage groups, respectively) is an interesting observation that is worth further investigation. The characteristics of optic atrophy are pale papilla, but with normal ratio of cup size to disk diameter. Exfoliation syndrome is a chronic, systemic, connective tissue disorder. It is primarily associated with vasculopathies, including transient ischemic attack, hypertension, angina, and myocardial infarction (3, 28). The connective tissue degeneration of the lamina cribrosa of the sclera and ischemic lesions in optic nerve may attribute to this optic neuropathy.
As to the gain in visual acuity, whether the mean BCVA on the first day or 3 months after surgery, it was better in the early- and middle-stage groups than that in the late-stage group.
Generalized zonular weakness in XFS is progressive. Zonular weakness or dialysis is the primary risk factor for surgical complications in XFS. Capsular tension ring may be the optimal choice to protect probable zonular insufficiency of XFS (29, 30). As the diameter of the CTR is larger than that of the capsule bag, the centrifugal forces of the ring expand the capsular equator and buttress weak areas, providing equal distribution of support over the remaining zonules. Other advantages of CTR include a decreased prevalence of posterior capsule opacification (31) and possibly a reduced incidence of capsular contraction syndrome. However, standard CTR does not recenter a severely subluxed capsular bag or prevent progressive zonular loss. Not all CTR implantations are as effective as expected in preventing zonulo-capsular complications. Meanwhile, late spontaneous in-the-bag IOL and capsular tension ring dislocation in XFS are probable (32–35). Some surgeons advocate the use of the CTR in all XFS cases to protect against capsule contraction and progressive decentration. Capsular tension ring implantation results in improved IOL centration, reduced tilt, and decreased numbers of complications in XFS eyes (36). In view of this, standard CTR implantation is beneficial in decreasing capsular bag-related complications in XFS with high risk factors. Risk factors that predict zonular instability in XFS include a shallow or hyperdeep anterior chamber depth, increased age, increased cataract density, and reduced pupil size (23, 37). Optical low-coherence reflectometry before surgery enables preoperative detection of zonular weakness in patients with these risk factors (38). In our study, no subluxed capsular bag, capsular contraction syndrome, decentration, or dislocation of IOL after surgery was observed.
Conclusion
The clinical staging of cataract with XFS has contributed to the choice of operation time and its management. Clear corneal tunnel phacoemulsification and IOL implantation in early-and middle-stage XFS result in fewer complications and lead to better recovery of visual acuity after surgery. Preoperative detailed slit-lamp biomicroscopy under maximal mydriasis and careful intraoperative management, accompanied by the implantation of CTR, underpin the success of the operation.
Footnotes
Financial support: Supported by the Project of the National Nature Science Foundation of China (no. 81270989) and by the Project of Shanghai Science and Technology Committee Foundation (no. 124119a9900).
Conflict of interest: None of the authors has conflict of interest with this submission.