
Abstract
Purpose
Cystoid macular edema may occur following scleral buckling and therefore deteriorate the visual outcome. Inflammation may be the major causative factor in the development of postoperative cystoid macular edema. This case demonstrates the effectiveness of a dexamethasone implant as a treatment after the onset of choroidal inflammation and cystoid macular edema 6 months following scleral buckling and having visual acuity restored.
Methods
A 59-year-old phakic woman treated with scleral buckling for macula-off retinal detachment presented 2 months after surgery with cystoid macular edema with choroidal inflammation. Optical coherence tomography and fluorescein angiography were performed. From the time of the diagnosis, the patient's condition had been nonresponsive to medical therapy and only partially responsive to sub-Tenon triamcinolone acetonide. An intravitreal implant with a sustained release of 0.7 mg dexamethasone was implanted.
Results
Following an intravitreal injection with a dexamethasone implant, the macular edema subsided completely and optical coherence tomography showed decreased foveal thickness from 510 μm to 220 μm. Choroidal fluorescein leakage disappeared. Best-corrected visual acuity improved from 0.70 to 0.20 logMAR, a condition maintained throughout the 6 months of follow-up.
Conclusions
Cystoid macular edema and choroidal inflammation are difficult to treat, but the improvement observed in this case of post scleral buckling macular edema and choroidal inflammation showed how a dexamethasone implant proved to be useful during the 6-month follow-up.
Keywords
Introduction
Scleral buckling (SB) is a surgical procedure used to repair rhegmatogenous retinal detachment (RRD). Clinical reports indicate that final anatomic success rates are favorable following SB.
There are several complications associated with SB, which may contribute to the visual outcome, including cystoid macular edema (CME), which may occur 4–6 weeks postoperatively (1).
It is generally accepted that inflammation plays a dominant role in postoperative CME (2). Also, the encircling band may cause changes in the circulation of the retina and the choroid (3). There are postoperative complications related to these alterations in blood supply, such as anterior and posterior segment ischemia with CME, which influences visual recovery (3). Subclinical ischemia following scleral buckling may exist in many more cases than have been reported (3). During recent years, the advent of intravitreal pharmacologic therapies has opened up a new perspective in the treatment of postoperative CME.
This case study shows the efficacy of a dexamethasone implant as treatment after the onset of choroidal inflammation and CME after SB throughout 6 months of follow-up.
Case report
A 59-year-old phakic woman with high myopia (sf-9 D) was referred to our clinic in October 2013 because of macula-off RRD. The patient had undergone SB surgery with cryotherapy as retinopexy. One month later, best-corrected visual acuity (BCVA) improved from hand motion to 0.20 logMAR and fundus biomicroscopy revealed complete reattachment of the retina. In December 2013, the patient showed a new painless visual loss in her left eye with the appearance of metamorphopsia. The BCVA was 0.70 logMAR, IOP was 14 mm Hg, and slit-lamp examination showed no signs of ocular inflammation. Funduscopic examination revealed CME with no signs of inflammation and complete reattachment of the retina. Fluorescein angiography (FA) (Spectralis® OCT, Heidelberg Engineering, Heidelberg, Germany) showed signs of choroidal inflammation with early fluorescein leakage, choroidal infiltration, and CME (Fig. 1). There were no signs of uveitis in her fellow eye.
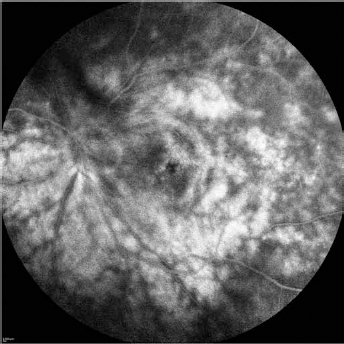
Fluorescein angiography at baseline shows signs of choroidal inflammation with early fluorescein leakage, choroidal infiltration, and cystoid macular edema.
Spectral-domain optical coherence tomography (SD-OCT) (Spectralis® OCT) was also performed, showing a remarkable increase in retinal thickness and an irregular retinal profile with the disappearance of the foveal depression. Moreover, diminished retinal reflectivity and optically empty intraretinal spaces typical of CME with an underlying serous foveal detachment were noted. Foveal thickness was 640 ± 4 μm (Fig. 2).
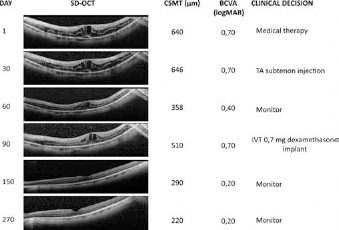
Progression of cystoid macular edema during the follow-up period. The figure illustrates spectral-domain optical coherence tomography (SD-OCT) scans, the central subfield mean thickness (CSMT), best-corrected visual acuity (BCVA), and clinical decision related to specific clinical features. Day refers to days after diagnosis of cystoid macular edema. TA = triamcinolone acetonide; IVT = intravitreal.
In order to exclude posterior unilateral uveitis related to infection or a systemic disease, a visit to the rheumatologic unit was carried out for laboratory screening, where a complete hemogram and serum electrolyte levels were assessed and found to be within normal limits. A comprehensive assessment was done to rule out other possible causes of uveitis.
The patient was initially treated with oral prednisolone (75 mg/day) for 1 week, with a weekly taper of 5 mg; oral administration of acetazolamide (250 mg/day) for 15 days; 1% topical prednisolone acetate 4 times a day; and 0.1% bromfenac sodium eyedrops twice a day for 30 days. However, the macular edema and BCVA were unaffected at the 1-month follow-up.
A sub-Tenon injection with corticosteroid (40 mg triamcinolone acetonide [TA]) was subsequently administered. One month following the sub-Tenon injection, OCT showed a decrease in foveal thickness (358 ± 32 μm) and a resolution of the subfoveal retinal detachment (Fig. 2). The BCVA increased to 0.40 logMAR but FA showed no change in choroidal inflammation with manifested CME.
The macular edema worsened 60 days post sub-Tenon injection; the patient reported a new subjective reduction of BCVA (0.70 logMAR); OCT macular thickness was 510 μm with new intraretinal cysts (Fig. 2).
Considering the partial and transient improvement after sub-Tenon steroid injection, a dexamethasone implant with a sustained release of 0.7 mg dexamethasone was implanted. The patient was aware of the off-label nature of the treatment and gave informed consent for the procedure.
Two months postinjection, BCVA was 0.20 logMAR. The macular edema was markedly reduced with a central subfield mean thickness of 290 μm (Fig. 2). The FA showed resolution of choroidal leakage (Fig. 3). This condition remained stable during 6 months of follow-up (Fig. 2).
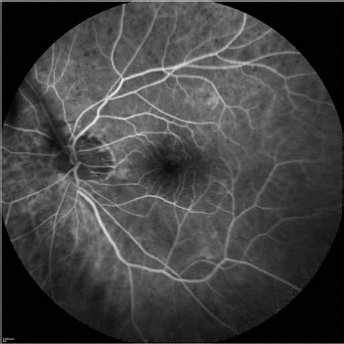
Fluorescein angiography 1 month after dexamethasone implant shows complete resolution of the choroidal leakage.
Discussion
This case study is of a patient with choroidal inflammation and CME following SB. Scleral buckling is an effective procedure for treatment of RRD, but complications may lead to decreased vision and failure of treatment. Postoperative CME has been reported in 14%-42% of patients following SB with an encircling band (1). Cystoid macular edema was reported in the literature as a rare complication of scleral necrosis following SB (4) or in cases of noninfectious uveitis.
Our patient had no signs of scleritis: there was no conjunctival injection and no pain; a B-scan ultrasound did not show any signs of scleral or orbital inflammation. Regarding noninfectious uveitis, the laboratory tests to identify systemic disease all resulted negative, and the fellow eye had no signs of uveitis. Hence, inflammation was the probable underlying pathogenesis for this postoperative complication.
Although advanced age was reported to be a risk factor for CME after ocular surgery, Tunc et al (1) showed no significant difference in mean age between those patients who developed CME and those who did not. The patient in this case study was not of advanced age.
During previous SB, cryotherapy was used as retinopexy, and some authors believe that this method may induce more scleral and choroidal inflammation in comparison to laser retinopexy, therefore playing a role in the difference of CME frequency after SB (1). In contrast, Avitabile et al (5) demonstrated that the rate of postoperative complications was not influenced by the type of retinopexy.
Previous reports indicate higher CME rates in aphakic and pseudophakic patients following SB (1). The affected eye of our patient was phakic. Postoperative CME was observed at higher rates if the macula was detached preoperatively compared to the patients without macular involvement, even if the patient had had successful anatomic reattachment of the retina (1). Our patient had macula-off retinal detachment.
The changes in the choroid and retinal microcirculation induced by SB surgery may be another possible cause related to CME (3). The encircling band causes changes in the circulation of the retina and the choroid (6), which might be improved after relaxation of the encircling band.
The pathogenesis of CME in this patient is unknown but inflammation was the major causative factor in the development of CME and choroidal leakage. Steroids were used to reduce postoperative complications following SB, and oral corticosteroids are always administered by us. We decided to treat the patient with sub-Tenon injections of TA to test the therapeutic response to corticosteroid and intraocular pressure control. Sub-Tenon TA injection was able to reduce CME, but was ineffective in reducing choroidal inflammation, whereas sustained delivery of 0.7 mg dexamethasone implant induced a significant improvement of BCVA from 0.70 to 0.20 logMAR and complete remission of macular edema and choroidal leakage throughout 6 months of follow-up.
Many studies have reported the efficacy of 0.7 mg dexamethasone implant in the management of postoperative CME (7), but to date no studies have reported the use of this implant for CME following SB.
Our results have shown that a dexamethasone implant leads to rapid improvement in both functional (BCVA) and morphologic (FA and SD-OCT) parameters of CME. The advantage of this treatment, compared to steroid intravitreal injections, is long-term control of inflammation and macular edema with a reduced frequency of administration.
Footnotes
Acknowledgments
The authors thank Veronica Gavin, BSc, TEFL, for English proofreading.
Financial support: No financial support was received for this submission.
Conflict of interest: None of the authors has conflict of interest with this submission.