
Abstract
Purpose
We performed a retrospective study to evaluate the surgical efficacy and timing of 23-G vitrectomy for acute endophthalmitis following cataract surgery, and to determine when silicone oil tamponade and intraocular lens (IOL) removal are indicated during vitrectomy for endophthalmitis.
Methods
We enrolled 21 patients (21 eyes) diagnosed with acute endophthalmitis following cataract surgery who underwent endoscope-assisted 23-G vitrectomy using a wide-angle noncontact lens. Silicone oil tamponade was performed when retinal tear or detachment occurred. The IOL was not removed during primary vitrectomy. Postoperative systemic broad-spectrum antibiotics were used.
Results
All infections were controlled by treatment. Best-corrected visual acuity was >0.05 in 14 patients (66.7%) after treatment, which was significantly higher than that before treatment (2/21, 9.5%). Two patients experienced retinal detachment at 10 and 14 days after primary vitrectomy; the IOL was removed during secondary surgery, and silicone oil tamponade was performed. One patient experienced endophthalmitis recurrence 2 months after vitrectomy; secondary surgery was performed to remove the peripheral vitreous body, the pars plana of the ciliary body, and the IOL and capsule.
Conclusions
Vitrectomy should be performed when acute endophthalmitis is diagnosed following cataract surgery. Silicone oil tamponade should be performed only when retinal break or detachment occurs. The IOL does not necessarily require removal.
Introduction
Cataracts are the leading cause of blindness in the elderly (1), and cataract surgery has emerged as one of the most common and successfully performed eye surgeries. As the elderly population increases, an increasing number of cataract surgeries have been performed. The large numbers of affected individuals and extensive experience of surgeons render cataract surgery relatively safe, but uncommon complications can occur.
The complication of acute endophthalmitis often occurs 1–2 weeks following cataract surgery, and has the potential to cause severe visual impairment (2). Although the general incidence of endophthalmitis is low (approximately 0.13–0.7%) (3), 90% of cases occur following cataract surgery (4). Therefore, designing preventative strategies to decrease the risk of endophthalmitis after cataract surgery, which will ultimately help prevent postoperative visual impairment, is important.
The primary cause of endophthalmitis after cataract surgery is bacteria from the cornea, conjunctiva, lacrimal glands, eyelids, and extraocular muscles (5). The most frequently isolated bacterium is Staphylococcus epidermidis, followed by S aureus, Streptococcus spp, and Gram-negative bacteria (3, 5). As the majority of cases are attributed to Gram-positive bacteria, antibiotics that are selective against Gram-positive bacteria, such as vancomycin and cefazolin, are most often used as treatment (6, 7). Intravitreal injection of antibiotics is recommended for the effective management of bacterial endophthalmitis (8, 9), as systemic administration of antibiotics such as vancomycin may not achieve effective bactericidal concentrations due to poor penetration of the drugs into the vitreous humor (10).
Vitrectomy is an effective alternative treatment option for endophthalmitis after cataract surgery (8, 11). It removes bacteria, inflammatory cells, and other toxic substances from the vitreous cavity via cutting and aspirating the vitreous content. Vitrectomy has the additional benefits of providing better diffusion of antibiotics and removing inflammatory membranes, which promotes recovery of vision (12).
Several studies have shown that vitrectomy improves visual acuity in patients with endophthalmitis (8, 13), and sutureless 23-G vitrectomy has been reported to have many advantages, such as shorter operating and recovery times, as well as less postoperative discomfort (14, 15); moreover, the procedure has been demonstrated as safe for treating postoperative endophthalmitis (16). Although it is generally accepted that vitrectomy should be performed immediately in severe endophthalmitis, controversies remain concerning the use of silicone oil tamponade and removal of the intraocular lens (IOL) during vitrectomy for severe endophthalmitis.
In this retrospective study, we performed 23-G vitrectomy to treat endophthalmitis in 21 patients (21 eyes) who had undergone cataract surgery. We evaluated the surgical efficacy and timing of vitrectomy for endophthalmitis after cataract surgery. The findings from this study will guide the treating physician as to when silicone oil tamponade should be used and when the IOL should be removed during vitrectomy for endophthalmitis.
Materials and Methods
Patients
The study was performed with prior approval from the Medical Ethics Committee of Jinan Second People's Hospital; all study subjects provided informed consent prior to enrollment. This study included 21 eyes from 21 patients who developed acute endophthalmitis following cataract surgery, which had been carried out between January 2010 and June 2014. With the exception of 2 patients (2 eyes) who underwent cataract surgery at our hospital, the remaining 19 patients had undergone cataract surgery at other hospitals. Intravitreal injection of drugs was administered in 10 of those 19 eyes.
Among the total study population, 15 patients (15 eyes; 71.4%) were male. Clinical symptoms following cataract surgery were progressive decline in visual acuity, eye pain, increased secretion, swollen eyelids, conjunctival congestion and edema, corneal edema, gray keratic precipitates, and anterior chamber exudation or empyema (Fig. 1). All patients underwent B-scan ocular ultrasound to investigate vitreous opacities. The duration between the onset of clinical symptoms, diagnosis, and treatment ranged from 1 to 14 days. Vitreous specimens for bacterial culture and drug sensitivity tests were obtained in a timely manner from the infected eyes.
Surgical procedures
We performed 23-G pars plana vitrectomy immediately upon diagnosis of infectious endophthalmitis. If the cornea was clear, the anterior chamber of eyes with excessive empyema and vitreous opacities was irrigated, followed by extensive removal of the vitreous body by endoscope-assisted vitrectomy using a wide-angle noncontact lens. To treat bacterial infection, additional irrigation was carried out using 500 mL balanced salt solution (BSS) supplemented with vancomycin (10 mg) and ceftazidime (20 mg). To treat fungal infections, additional irrigation was carried out using 500 mL BSS supplemented with amphotericin B (400 μg).
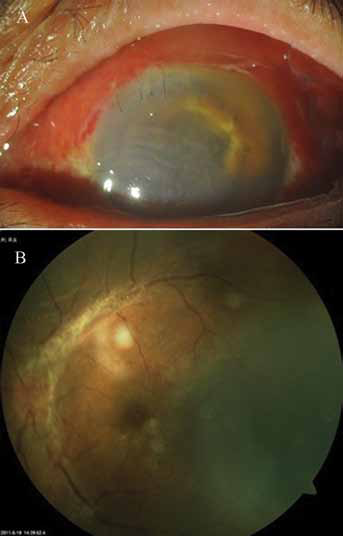
Photographs of a representative patient with acute endophthalmitis after cataract surgery. (A) The left eye of a 68-year-old man with acute endophthalmitis occurring 5 days after cataract surgery. Previtrectomy, the visual acuity of the patient was only sufficient for detecting hand motion. (B) Funduscopic examination of the patient after primary vitrectomy. Visual acuity was 0.2 after vitrectomy.
Eyes with severe corneal edema preventing clear fundus observation were treated by removing the central part of the vitreous body by vitrectomy, followed by irrigation with antibiotics. Secondary vitrectomy was performed after the cornea was clear.
Silicone oil tamponade was performed if retinal breaks or detachment were found during surgery. The silicone oil was removed after 3–6 months. In no patient was the IOL removed during primary vitrectomy.
Postoperative management
All patients received postoperative systemic or topical broad-spectrum antibiotic therapy involving cephalosporin and quinolones. We followed patients for 6.2 ± 2.7 months (range 3–9 months).
Statistical analysis
We performed analyses using SPSS 19.0 (IBM SPSS, Armonk, NY, USA). Categorical data were compared using the χ2 test. Probability values <0.05 were considered statistically significant.
Results
Pathogens
Eight of the 21 vitreous specimens (38.1%) produced positive bacterial cultures of the following bacteria: S epidermidis (n = 4), S aureus (n = 2), Streptococcus (n = 1), and Escherichia coli (n = 1).
Surgical treatment
The mean operation time for all vitrectomies was 45 ± 12 minutes. For 2 patients, the scleral tunnel was not well-closed during vitrectomy, and required suturing. Another 2 patients experienced retinal tears with large areas of retinal and blood vessel necrosis, which both required silicone oil tamponade. In 2 other patients, retinal detachment occurred at 10 and 14 days after primary vitrectomy. The retinal tears occurred in the periphery of the central part of the inferior retina, distal from the puncture hole in the periphery of the retina; the IOL was removed during secondary surgery, and silicone oil tamponade was performed. Three patients developed severe corneal edema; as the fundus was not clearly visualized, the central part of the vitreous body was removed by primary vitrectomy, and secondary vitrectomy was performed 3 days after the primary vitrectomy when the cornea was clear. One patient experienced recurrence of endophthalmitis 2 months after vitrectomy; we performed secondary surgery to remove the peripheral vitreous body, pars plana of the ciliary body, IOL, and capsule. There was no infection during the 9-month follow-up period. All patients developed corneal edema and aqueous flare, which occurred between days 5 and 7 after surgery. Endophthalmitis was controlled after surgery.
Visual acuity
In all patients, the surgery resolved the endophthalmitis; in addition, the empyema in the anterior chamber disappeared, allowing preservation of the eyeball, and visual acuity was improved. In some patients, the best-corrected visual acuity (BCVA) was >0.3 (Tab. I). While only 2 patients (9.5%) overall had BCVA >0.05 before treatment, 14 patients (66.7%) overall had BCVA >0.05 after treatment, and the difference was significant (χ2 = 15.003, p = 0.002).
Best-corrected visual acuity before and after treatment
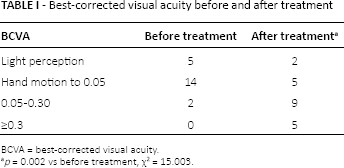
BCVA = best-corrected visual acuity.
p = 0.002 vs before treatment, χ2 = 15.003.
Discussion
Most studies indicate that vitrectomy should be performed for severe endophthalmitis after cataract surgery (8, 11). When intravitreal injection of antibiotics is ineffective for relieving endophthalmitis after 4–6 hours, vitrectomy should be performed immediately. If vitrectomy is not feasible at the local hospital, intravitreal injection of antibiotics should be administered, and the patient should be transferred to another hospital for vitrectomy.
The large instrument diameter in 20-G vitrectomy produces a large surgical incision, frequently resulting in access to the sclera that can lead to iatrogenic retinal breaks and traction of the base of the vitreous body. In contrast, 23-G vitrectomy uses a sophisticated, minimally invasive surgical instrument, which reduces the size of the surgical incision and decreases postoperative complications and operating time (17, 18). In the present study, we used noncontact wide-angle viewing, which allows 130° visualization, to facilitate the 23-G vitrectomy, reducing operating time and facilitating surgery.
The American Endophthalmitis Vitrectomy Study Group recommends that vitrectomy should be performed for routine endophthalmitis to remove the central part of the vitreous body, as excessive compression may lead to retinal breaks when the base of the vitreous body is removed (8). In this study, the IOL was not removed during primary vitrectomy, but 3 cases needed IOL removal during secondary vitrectomy. It is recommended that the IOL and capsule be removed in recurrent endophthalmitis after primary vitrectomy, as certain bacteria, such as Enterococcus faecalis, can easily adhere to the IOL and capsule. This strategy also addresses the complication wherein routine doses of antibiotics cannot achieve the minimum inhibitory concentration in the IOL and capsule, leading to poor prognosis and frequent recurrence (19, 20). The IOL should also be removed in cases involving large defects in the posterior capsule and suspensory ligament, as following its suturing to the sclera, or when silicone oil tamponade is required, the IOL may leak silicone oil into the anterior chamber. In general, for all other cases, the surgeon should aim to preserve the IOL.
As silicone oil has antimicrobial properties, and pathogens may gradually die in the nutrient-deficient silicone oil (21), several doctors advocate its use for increasing the success rate of vitrectomy and for improving visual acuity in patients with acute endophthalmitis (22). However, silicone oil tamponade and repeated surgeries are associated with increased risks and complications. Therefore, surgeons should use silicone oil tamponade with caution. In the present study, silicone oil tamponade was only used in eyes with retinal break or detachment. Postoperative delivery of local or systemic antibiotics controlled infection in all cases in this study. In the 2 patients who experienced retinal detachment, the retinal tears occurred in the periphery of the central part of the inferior retina, suggesting that retinal breaks may result from posterior traction of the residual vitreous cortex. Edema causes the retina to become thinner, rendering it more fragile and more at risk of tearing. Timely surgery to repair retinal breaks can achieve good retinal reattachment. To avoid retinal detachment caused by traction by the residual vitreous cortex, it is recommended that the posterior vitreous body be detached as soon as possible. However, care should be taken to avoid iatrogenic retinal breaks.
In summary, vitrectomy should be performed when acute endophthalmitis is diagnosed following cataract surgery. If vitrectomy cannot be performed at a local hospital, intravitreal injection of antibiotics should be administered initially, and patients should be transferred to another hospital for vitrectomy. Silicone oil tamponade is not necessary unless retinal break and/or detachment occur. With the exception of recurrent endophthalmitis and infection by bacteria such as E faecalis, it is not necessary to remove the IOL. In addition, where there are large defects in the posterior capsule and suspensory ligament requiring silicone oil tamponade, the IOL should be removed to prevent the entry of silicone oil into the anterior chamber. Although these treatments are effective for acute endophthalmitis following cataract surgery, the rate of blindness remains high; therefore, it is important to use the findings presented in the literature and herein to prevent the occurrence of endophthalmitis.
Author contributions
Jingjing Zhang carried out the clinical study and literature search, participated in the statistical analysis, and drafted the manuscript. Fangju Han conceived the study and participated in its design, carried out the clinical study, and helped to draft the manuscript. Xiangjuan Zhai participated in the design of the study and performed the statistical analysis. All authors read and approved the final manuscript.
Footnotes
Acknowledgment
The authors thank Medjaden Bioscience Limited for assisting in the preparation of this manuscript.
Financial support: No financial support was received for this submission.
Conflict of interest: None of the authors has conflict of interest with this submission.