
Abstract
Purpose
To use multimodal imaging to evaluate the prevalence of reticular pseudodrusen (RPD) in eyes with newly presenting neovascular age-related macular degeneration (nAMD) in a UK population and explore associations with RPD and angiographic subtypes of nAMD.
Methods
A retrospective review of all spectral-domain optical coherence tomography, color fundus photographs, red-free and blue channel images, and fundus fluorescein angiograms of 202 consecutive patients who presented to a rapid access macular clinic over a 4-year period was performed. All images were graded by at least 2 ophthalmologists for the presence of RPD and choroidal neovascular membrane (CNV) subtypes.
Results
A total of 231 consecutive eyes were studied, of which 131 (56.7%) were in women. Of these, 51 eyes with CNV (22.1%) had identifiable RPD, with one or more imaging methods in that eye. A total of 30.3% of patients with newly presenting CNV in either or both eyes had identifiable RPD. The RPD were bilateral in 85.4% of patients and were identified more commonly in women than men (72.5% vs 27.5%), a difference that reached statistical significance (p = 0.011). No association between RPD and any particular CNV subtype was demonstrated, including for retinal angiomatous proliferations (RAP).
Conclusions
Reticular pseudodrusen have a high prevalence in eyes presenting with nAMD (22.1%), although at rates much lower than that of conventional drusen. They are largely a bilateral finding, occurring more frequently in women. Unlike other previous reports, we found no difference in their occurrence between the different subtypes of CNV including RAPs.
Introduction
Across industrialized countries, age-related macular degeneration (AMD) is the most frequent cause of visual loss in older individuals (1-3). The earlier stage changes in AMD are referred to as age-related maculopathy (ARM). Visual impairment may result from the later stages of AMD, which manifests as either geographic atrophy (GA) or exudative/neovascular disease, which implies the presence of a choroidal neovascular membrane (CNV) (4). Previous classification systems developed for epidemiologic studies and clinical trials utilized color fundus photography as their single imaging modality (4-6). These classification systems were based primarily on the assessment of drusen and their margins (distinct or indistinct), and their size and substance (hard or soft), along with number, distribution, and confluence, as well as the association of pigmentary changes. The association between drusen and GA or CNV has long been established and was first reported by Gass in 1973 (7). These yellow sub–retinal pigment epithelial lesions have become recognized as the hallmark of age-related maculopathy. The presence of drusen (along with areas of focal hypopigmentation or hyperpigmentation) has come to signify an increased risk of progression to the more advanced stages of AMD and the associated potential for visual loss (8, 9).
A new phenotypic description within the spectrum of the already diverse ARM was added in 1990 with a publication by Mimoun et al (10), who described a particular yellowish pattern in the fundus of patients with AMD that was more visible using red-free or blue light fundus photography. They termed the pattern les pseudodrusen visibles en luminere bleue (pseudodrusen visible with blue light) (10). The importance of this newly described fundus finding became clear in 1995 when Arnold et al (11) observed that two-thirds of eyes with pseudodrusen had or developed CNV. It became evident that reticular pseudodrusen (RPD) had clinical features and prognosis that were different from those of conventional drusen. Several publications have since revealed a high prevalence of RPD in eyes with AMD (12-19).
There are limited data available on the prevalence of RPD within large population-based epidemiologic studies (20, 21). One reason for this is the previous misclassification of RPD as forms of soft drusen, along with difficulties in their clear identification without the use of multimodal imaging. Furthermore, RPD were not specifically included in the international classification system for AMD (4). Therefore, when present, they would not have been differentiated from soft drusen using this international grading system (4). The Beaver Dam Eye Study (BDES) by Klein et al (5) recorded this phenotype as a separate entity named reticular drusen using mydriatic color stereoscopic photography. The reported prevalence and 15-year cumulative incidence in the over 43 age group were 0.7% and 3%, respectively, in the BDES (21). The prevalence increased with age and is as high as 6.6% in the age range 75-86 years (21). In the BDES, eyes with RPD were twice as likely to progress to AMD compared to those with soft drusen. Reticular pseudodrusen also conferred a higher risk of developing visual impairment. The actual prevalence of RPD within the community eyes and eyes presenting with AMD may have been underestimated in some previous studies that utilized color fundus photography alone in their grading. Newer imaging modalities such as spectral-domain optical coherence tomography (SD-OCT), near-infrared reflectance (IR), fundus autofluorescence, and confocal scanning laser ophthalmoscopy have led to improvements in the diagnosis of RPD (18, 22-26). The higher sensitivity and specificity of some of these imaging modalities has led to the assessment of RPD being based on multimodal imaging in the more recent publications. A limited number of previous publications available on the subject suggested a higher prevalence of RPD in eyes with retinal angiomatous proliferations (RAP), a particular neovascular AMD (nAMD) phenotype (12).
We performed a retrospective review of all consecutive cases of newly diagnosed nAMD in our center in order to assess the association with RPD. We also assessed the different CNV lesion subtypes for any association with RPD.
Methods
A retrospective review of all SD-OCT, color fundus photographs (CFP), and fundus fluorescein angiograms (FFA) of 202 consecutive patients who presented to a rapid access macular clinic in Kings Mill Hospital, Sutton-in-Ashfield, UK, over a 4-year period (February 2009 to February 2013) was performed. Inclusion criteria were all patients over 50 years of age with active CNV in at least one eye during the period of interest. Exclusion criteria were patients who had either no SD-OCT or CFP/FFA available for analysis or those in whom one or more imaging modality was deemed ungradable. Patients with bilateral CNV were not excluded. Patients with CNV secondary to angioid streaks or chorioretinitis were excluded. No patients were excluded on the basis of their best-corrected visual acuity. A small number may have had previous treatment with photodynamic therapy or intravitreal injections of anti–vascular endothelial growth factor (anti-VEGF) agents at 6 months or more previously. These were included as new cases of CNV. The refractive status of patients was not known, and as such, a small number of individuals may have been myopic but were not specifically excluded from the analysis.
Color fundus photographs were taken using the Topcon TRC-50DX, Type IA retinal camera (Topcon, Tokyo, Japan) combined with an attached Nikon D7000 16.2-megapixel camera. The operator was an experienced ophthalmic photographer. Bilateral 35° mydriatic nonstereoscopic photographs of field 2 (centered on the fovea) were reviewed using the IMAGEnet i-base system (Topcon). The standard FFA protocol included 35° images of the transit phase, mid phase, and late phase up to 10 minutes. Images were all reviewed nonstereoscopically. The SD-OCT images were acquired using the 3D OCT-1000 instrument (Topcon). The field of view used was a 6 mm × 6 mm area, centered on the fovea. A raster scan consisting of a total of 128 frames, each consisting of 512 axial scans, was performed for each patient within this field. All 128 frames within each raster scan were individually reviewed for each patient for the presence of RPD covering a large macular area.
All retinal images were graded by at least 2 ophthalmologists with appropriate experience in AMD image grading (C.W., M.P., A.L., or W.M.K.A.). Side by side grading with open discussion was used. The graders were blind to any patient clinical information such as history or visual acuity. If there was disagreement between the 2 grading ophthalmologists, then immediate open adjudication would take place. If agreement could not be reached or the 2 ophthalmologists were not 90% confident of their assigned grade, then adjudication by a third ophthalmologist would occur. All SD-OCT images were reviewed without reference to the CFP and vice versa. With CFP, RPD were considered present if there was a definite reticular pattern of round or oval yellow-white lesions that joined to form an ill-defined network of broad, interlacing ribbons. An example is shown in Figure 1. The CFP was initially graded without digital alteration and subsequently graded with adjustment to the red-free and the blue channels of the fundus photograph (to enhance pseudodrusen visualization) using the IMAGEnet i-base program as illustrated in Figure 2. Although the actual histologic localization of the lesions is controversial (11, 27), RPD were considered present on SD-OCT by the definite presence of 5 or more discrete hyperreflective collections in the subretinal space that were sufficient to alter the contour of the presumed inner segment–outer segment junction (23) as shown in Figure 3.
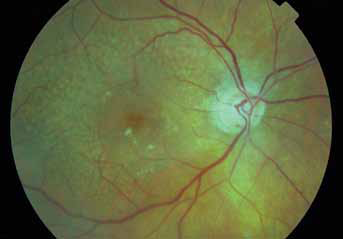
Color fundus photograph demonstrates reticular pseudodrusen. There are multiple round and oval yellow-white lesions that join to form an ill-defined network of broad, interlacing ribbons.
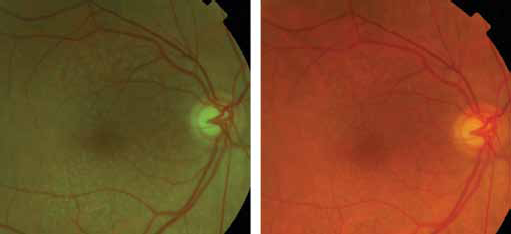
Color fundus photograph demonstrates enhanced visualization of reticular pseudodrusen after digital alteration to the red-free channel using the IMAGEnet iBase program.
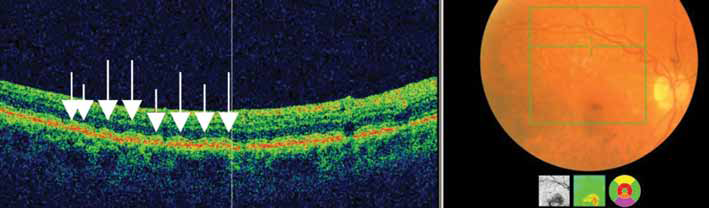
Spectral-domain optical coherence tomography demonstrates discrete hyperreflective collections in the subretinal space giving a saw-tooth appearance.
The FFA of CNV lesions were graded using the Modified Photocoagulation Study grading protocol that was utilized in the Treatment of AMD with Photodynamic Therapy and Verteporfin in Photodynamic Therapy studies (28, 29). Classic CNV was identified as an area of uniform and early (less than 30 seconds) hyperfluorescence that showed leakage throughout the mid and late phases. Occult CNV was identified by areas of increasing stippled hyperfluorescence that appeared in the mid and late phases of the FFA with a leak or a late leak of undetermined origin. The FFA images were graded as classic, predominantly classic, minimally classic, occult, peripapillary CNV, no CNV, or other pathology. Choroidal neovascularization was considered present on fluorescein angiography if classic or occult leakage was detected. In addition to the above grading, images were assessed for the presence of a RAP as described by Yannuzzi et al (30).
Eyes with newly presenting nAMD were divided into those with and without RPD. The 2 groups were compared for sex, age, laterality of eye involved, and bilateral presentation using the Fisher exact test. The χ2 test was used to assess the association of CNV subtypes with RPD. For RAP, the Fisher exact test was used. All images of contralateral eyes (when available and gradable) of patients presenting with nAMD were also reviewed and graded using the methods described above.
All applicable institutional and governmental regulations were followed during this research.
Results
Our study cohort was composed of 202 consecutive patients presenting with nAMD. Twenty-nine individuals (14.4% of patients) presented with bilateral active CNV, whereas the other 173 had unilateral CNV. As such, a total of 231 consecutive eyes were studied, of which 131 (56.7%) were in women. The mean age at presentation was 80.4 years with standard deviation (SD) 7.6 years. A total of 51 eyes with CNV (22.1%) had identifiable RPD with one or more imaging method in that eye. Overall, 30.3% of patients with newly presenting CNV in either or both eyes had identifiable RPD. Where contralateral gradable images were available, RPD was a bilateral finding in 85.4% of patients. Reticular pseudodrusen were identified more commonly in the eyes of women than men (72.5% vs 27.5%), a difference that reached statistical significance (p = 0.011). No significant difference was noted between eyes with and without RPD with regard to age or eye involved (Tab. I). Of the 29 patients (58 eyes) presenting with bilateral active CNV, 12 eyes (20.7%) had RPD. In the 173 eyes presenting with new onset of unilateral CNV, 39 (22.5%) had RPD. No association was found between the presence of RPD and bilateral presentation with active CNV (p = 0.852). No association of RPD with CNV subtype was found. The association of RPD with the different FFA types of CNV is summarized in Table II, and shows that there is no particular association of RPD with any particular CNV subtype. Similarly, the presence of RAPs with RPD is summarized in Table III and indicates no statistically significant association (p = 0.688).
Comparison of characteristics in patients with or without reticular pseudodrusen in the ipsilateral eye with newly presenting nAMD
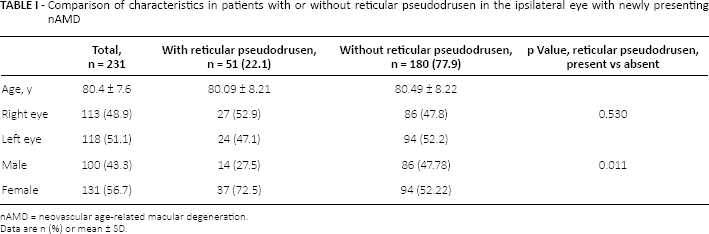
nAMD = neovascular age-related macular degeneration.
Data are n (%) or mean ± SD.
Fluorescein angiographic subtypes of neovascular age-related macular degeneration with and without reticular pseudodrusen
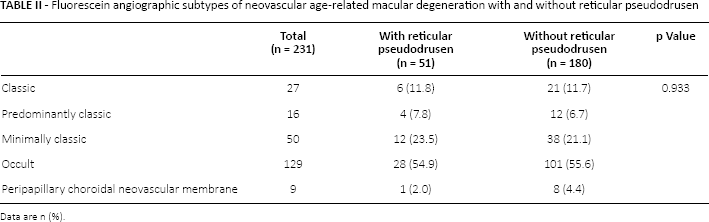
Data are n (%).
Contingency table for RAP with and without reticular pseudodrusen
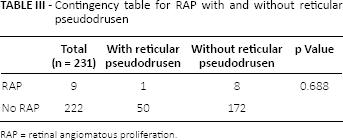
RAP = retinal angiomatous proliferation.
Images for 124 contralateral eyes to that with the CNV (unilateral) were available for analysis after exclusions. Excluded were 58 eyes of 29 patients presenting with bilateral active CNVs, 16 contralateral eyes that had disciform scars (end-stage CNV) that confounded adequate analysis, and another 33 contralateral eyes because the FFA, OCT, or CFP were ungradable or not available. Thirty-nine of the 124 available contralateral eyes (31.5%) had RPD, with an average age of 80.64 years (SD 8.73). A total of 32 contralateral eyes had GA (25.8%), with 13 of these (33.3%) having RPD present. Nineteen contralateral eyes without RPD had GA. The association of GA and RPD did not reach statistical significance (p = 0.268).
In the 155 eyes (67.1%) with newly presenting CNV, there was identifiable drusen of ≥63 µm within the Early Treatment Diabetic Retinopathy Study (ETDRS) grid. The prevalence of such drusen increased to 96.1% in eyes with RPD. In addition, 12.6% of eyes with newly presenting CNV had confluent drusen.
In individuals with detectable RPD in either eye, 48.6% had GA, active CNV, or a disciform scar in the contralateral eye. This occurrence was similar for individuals without RPD (44.7%).
The different imaging methods used in our study revealed different abilities to identify RPD. Of the 51 total eyes with CNV that had identifiable RPD with one or more imaging method, RPD were identified in 66.7%, 78.4%, and 90.2% using SD-OCT, color fundus photography, and red-free and/or the blue channel of color fundus photography, respectively.
Discussion
Reticular pseudodrusen is recognized as part of the AMD spectrum (12-19). The previously published rates of the occurrence of RPD in newly diagnosed nAMD vary among the different studies from 14% to 24% (12, 31). In the present study, the prevalence of RPD in consecutive cases of newly presenting nAMD was high (22.1%). Cohen et al (12) evaluated images from a population in France (similar to that in our study) using color, red-free, and blue light fundus photography, and reported an almost identical rate of 24% of RPD. Ueda-Arakawa et al (31) demonstrated that within a Japanese population with newly presenting nAMD, the prevalence of RPD was lower at 14%. These differences could be explained by the different imaging modalities used as well as the inconsistency of grading definitions. The Japanese study, for instance, would only grade RPD as definitiely present if identified on 2 or more imaging modalities whereas the Cohen study and the present one used presence on 1 or more imaging modality. The 2014 study reported by Hogg et al (19) suggested that RPD were best visualized by IR imaging, which was not used in the present study. Ethnicity, sex, or age distributions of the various populations may also play a role in the prevalence of RPD. Reticular pseudodrusen are in the mainstay a bilateral finding, with 63% of cases identified in the BDES having them in both eyes (20). In a 3-year prospective study, Pumariega et al (15) demonstrated that patients with unilateral CNV and large soft drusen in the fellow eye at baseline had a higher rate of progression to CNV if RPD were present as opposed to absent (44.7% vs 26.6%, p = 0.002) (15). The higher rate of RPD prevalence reported across prospective studies likely reflects the known tendency for RPD to fade with the development of CNV (15, 27). It is possible that some of the patients in our study may well have had RPD prior to the development of their CNV, which subsequently regressed or was obscured by the developing CNV or its consequences such as hemorrhage gliosis or fluid accumulation. This would be more likely for large membranes at presentation. This difficulty in RPD identification and grading in eyes with active nAMD may explain why the prevalence of RPD was higher when available contralateral eyes were reviewed within our cohort (31.5% vs 22.1%).
In the present study, the proportion of women with newly diagnosed nAMD in the RPD group was higher than men (72.5% vs 27.5%); this sex difference reached statistical significance (p = 0.011). This finding is consistent with that from previous reports (11, 12, 18, 20), although, to our knowledge, this is the first time such a difference has reached a statistically significant level within a population of newly incident nAMD. Arnold et al (11) found that 87% of patients with RPD were women, while Klein et al (21) demonstrated that the prevalence of RPD was 2.5 times higher in women than men. In the older Australian population, Joachim et al (20) demonstrated that after adjusting for age, the 15-year cumulative incidence of RPD was twice as likely in women than men (5.6% [95% confidence interval (CI) 5.59-5.61] vs 2.2% [95% CI 2.19-2.21]). Our findings further confirm the increased prevalence of RPD among women with nAMD. We found no difference between the ages of persons with or without RPD in our study. Others have suggested that patients with nAMD and RPD were likely to be older than those without (12, 31); however, none of these studies has shown the difference to be statistically significant.
There are few publications that have investigated the association between RPD and the various subtypes of newly presenting CNV (12, 15, 31). Cohen et al (12) reported a higher prevalence of RAPs in individuals with RPD (29.1%) than those without (7.8%), although the authors specifically cautioned against the interpretation of this finding, given the small number of patients included in the study. This association was repeated when Ueda-Arakawa et al (31) demonstrated a prevalence of RPD of 83.3% in patients with newly presenting RAP. In contrast, they also demonstrated that RPD were rarely found in patients presenting with polypoidal choroidal vasculopathy. Sawa et al (32) demonstrated that reticular speudodrusen were a risk factor for bilateral RAP. We found no association with RAP or other types of CNV in the present study. There may be several possible reasons for this. One potential explanation could be that our exclusion of images that were deemed ungradable and/or eyes that had no appropriate early frames on the FFA could have had a large proportion of RAPs.
Another common finding from existing literature is that drusen and other features of ARM are usually present in eyes with RPD (11, 12, 33). In our study, conventional drusen ≥63 µm were present within the EDTRS grid in 67.1% of all patients who presented with new-onset CNV. In those in whom RPD were present, the prevalence of drusen increased to 96.1%.
In keeping with the first report by Mimoun et al (10), we found that RPD are best visualized using the red-free and the blue channel of the color photograph when altered digitally with imaging software. Our detection rate with SD-OCT was significantly lower than that reported by others, with Ueda-Arakawa et al (22) recently reporting a sensitivity of 94.6%. Other groups have published rates that are more in keeping with ours, albeit in the contralateral eye of patients presenting with nAMD (19). Possible explanations for this could include the larger field of the 35° color photograph when compared to the 6 mm × 6 mm field of the SD-OCT raster scan used in this study. Many of the central macular OCT subretinal drusenoiud deposits (SDD) may have been obscured by any active CNV, rendering them visible only with a larger field colour photograph. It is interesting to note that in our study SD-OCT had a better ability to detect SDD in the contralateral eyes with no active CNV, with a detection rate comparable to that of color photography (71.9%). Our study demonstrated that failure to digitally enhance colour photographs (by analyzing red-free and blur channels) routinely will result in up to 11.8% of RPD being overlooked by color photography alone. Spectral-domain OCT imaging revealed 4 extra cases (7.8%) of RPD in eyes with active CNV that were not visualized with color photography or red-free/blue channel enhancement, emphasizing the need for the utilization of multimodal imaging.
The main limitation of this study is the unavailability of IR imaging. However, the combination of blue light and OCT would have mitigated against this. It is also possible that the CNV may have obscured some of the RPD.
In conclusion, the present study confirms findings from previous studies that RPD have a high prevalence in eyes presenting with nAMD (22.1%), although at rates much lower than the prevalence of typical conventional drusen. The contralateral eyes with no nAMD have an even higher prevalence of RPD (31.5%), reflecting the difficulty in drusen grading in the presence of CNV. Our study confirms that RPD are largely a bilateral finding and occur more frequently in women. Unlike some previous reports, we found no difference in their occurence between the different subtypes of CNV including RAPs.
Footnotes
Financial support: Supported by a research grant from the Macular Society UK.
Conflict of interest: None of the authors has conflicts of interest with this submission.