
Abstract
Purpose
Operating room (OR) time is an expensive resource that should be optimized to reduce costs. Individual preoperative risk parameters (PORS) assessment may aid in predicting cataract surgery time.
Methods
Dedicated software was developed and known risk factors for cataract surgery were integrated into it. Preoperative risk parameters were assigned to each patient in the preoperative meeting and the risk score was calculated. A total of 153 patients were divided according to a standard classification into low-risk group (PORS ≤2) and high-risk group (PORS >5). Duration of surgery for each group was compared by Student t test and linear regression analysis was used to calculate the relation between change in OR time and change in risk score.
Results
Patients in the high PORS group had longer surgery times when compared with patients in the low PORS group (37.6 vs 19.6, p<0.001). Risk scores positively correlated with surgery time (r = 0.30, p<0.001). Prediction equations for the OR time demonstrated for 2 surgeons that every increase in 1 risk point added 2.2 or 3.3 minutes to the OR time. Outliers (more than 1 standard deviation [SD] from each surgeon's surgery mean time) had more than twice the risk score of cases within 1 SD from the mean.
Conclusions
The PORS system may be a useful tool for predicting OR time based on individual patient risk and may improve OR scheduling.
Introduction
Cataract extraction is the most common operation performed in the United States (1). Accurate prediction of and control for variation in the procedure's duration may improve operating room scheduling, reduce the unit cost per surgery and waiting list times, and increase the number of operations performed (2-4). Predicting a cataract surgery's duration mainly depends on estimates for similar cases and on the surgeon's skill level (5). Prediction accuracy may be improved by applying statistical models to the assessment of surgery complexity made by the surgeon (6).
Muhtaseb et al (7) introduced a preoperative risk (PORS) assessment method based on analysis of intraoperative complications in 1441 cataract surgeries. They devised a scoring system placing patients into 1 of 4 risk groups according to anatomical and demographic parameters such as age, ametropia, previous vitrectomy, corneal scarring, pupil size, anterior chamber depth, pseudoexfoliation (PXF), cataract staging, and phacodonesis. This system enables uniform and objective risk assessment and better preparation of a patient's expectations.
As operating room (OR) time is an expensive resource that should be optimized, we aim to evaluate whether the PORS system, which predicts surgical complications, will also aid in predicting surgery time. We developed dedicated software (EyeDB) to conduct the semiautomatic calculation of a patient's PORS. In this study, we examine the feasibility of integrating the EyeDB into our daily practice and using it to predict surgery time for a patient based on individual risk and designated surgeon.
Methods
The study was conducted at the Edith Wolfson Medical Center, Holon, Israel, adhered to the tenets of the Declaration of Helsinki, and was approved by the local ethics committee. Patients were consecutively recruited from November 2013 to December 2014.
Software design
The software design was based on Agile/Lean architecture (8). We used free, open source software to create an accessible Web development environment (WampServer.com). The Web service was developed in JavaScript (client-side), PHP (server-side), and MYSQL (database). The service can be installed on a local computer and accessed on multiple operating systems (Windows, Linux, and IOS) and Web browsers (i.e., Firefox, Chrome, and Safari). The client side utilizes libraries such as JQuery and twitter bootstrap to provide an interactive and intuitive user experience. All the technologies used in this project are widely used, free, cross-platform, and actively maintained. Software design was conducted voluntarily by user interface designer (https://www.linkedin.com/in/jaclyneclarke). The software can be downloaded for free and installed easily from http://wtf.co.il/eyedb.zip. Tutorial for setting up the Wamp server and installing the EyeDB software can be found here: https://vimeo.com/102517639.
Risk scoring
The PORS were assessed at the preoperative examination for each patient. One point of risk was assigned to a patient with the following parameters: previous vitrectomy, corneal scarring, small pupil (<3 mm), shallow anterior chamber (<2.5 mm), age >88 years, high ametropia (>6 D or <-6D), posterior capsule plaque, or posterior polar cataract. Three points of risk were assigned to a patient with mature or brunescent cataract, phacodonesis, or PXF. Miscellaneous factors for increasing surgical risk were assessed and risk points were allocated as fit by the physician. For example, deep-set eyes contribute 1 risk point and α-antagonist use (risk of intraoperative floppy iris syndrome) contributes 2 risk points (Fig. 1).
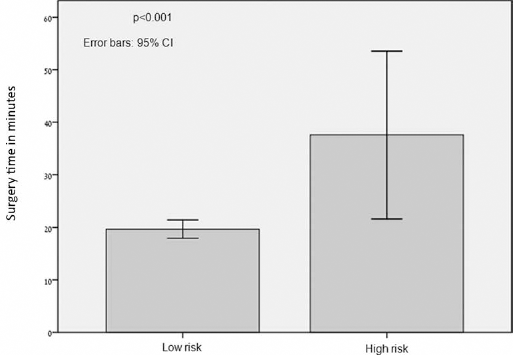
Surgery time by risk group. CI = confidence interval.
Risk score was calculated by accumulation of all risk points and patients were divided into low-risk group (PORS ≤2) and high-risk group (PORS >5). This categorization is based on intraoperative complications rate (low risk [4.3%] vs high risk [32.0%]) (7).
Surgery time
Operating room time was calculated as the time between first corneal incisions and undraping of patient at the end of surgery. Operating time was recorded by a nurse, unaware of this study. Surgery time was retrospectively queried from computerized files of randomly selected patients. Surgeries where resident teaching occurred were excluded.
Statistical analyses
Correlations between OR time and clinical parameters were evaluated by Spearman rank correlation coefficient. Linear regression analysis was used to calculate the change in OR time from the change in the risk score. Comparisons between risk groups were conducted by Student t test. p Values <0.05 were considered significant. All statistical calculations were performed using SPSS for Windows, version 15.
Results
Using the EyeDB, we calculated the PORS for 178 patients undergoing cataract surgery. Analyses were conducted on 150 surgeries after 28 teaching cases were excluded. Demographic data are summarized in Table I. Patients in the high-risk group were older (81.3 vs 73.1 years, p = 0.008) and had longer surgery (37.6 vs 19.6 minutes, p<0.001) (Fig. 1).
Patient demographics
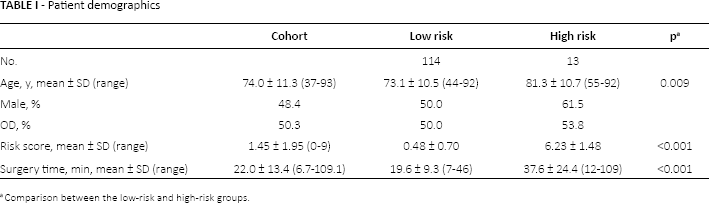
Comparison between the low-risk and high-risk groups.
Although surgeries were conducted by 9 different surgeons (supplementary Fig. 1, available online at www.eur-j-ophthalmol.com), regression analysis showed that risk scores for all patients were positively correlated with surgery time (r = 0.30, p<0.001).
In order to further control for variance in surgeon skills, we calculated the mean surgery time for each surgeon and identified cases more than 1 SD from each surgeon's mean time. These cases (n = 18) representing the outliers for each surgeon's mean surgical time had more than twice the risk score of cases within 1 SD from the mean (3.16 vs 1.22, p<0.001).
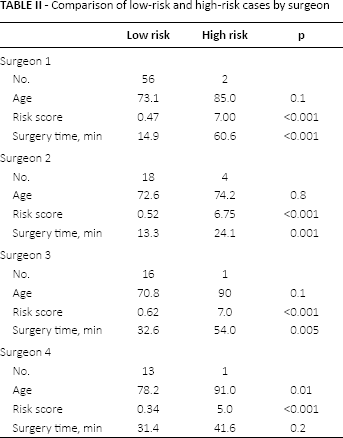
In addition, we compared surgery length of the high-risk patients to the low-risk patients for the 4 surgeons with the larger number of cases (n = 70, n = 27, n = 19, n = 18). A difference of 61.0 minutes (p<0.001), 24.4 minutes (p<0.001), 12.3 minutes (p<0.001), and 18.0 minutes (p<0.001) could be demonstrated between high-risk and low-risk patients (Tab. II). Regression analysis for each surgeon demonstrated that PORS accounted for significant variability in OR time for 2 surgeons (29% and 51%) and a prediction equation for the OR time could be calculated for each surgeon (every increase in 1 risk point added 2.2 or 3.3 minutes to the OR time, respectively). For the 2 other surgeons, PORS accounted for a nonsignificant 5% (p = 0.07) and 3% (p = 0.46) of the variability in OR time (Tab. III). We observed complications in 4 cases (Tab. IV). These cases had a mean PORS of 3.2 and included 2 high-risk patients and 1 low-risk patient.
Comparison of low-risk and high-risk cases by surgeon
The effect of risk score on the length of cataract surgery for 2 individual surgeons
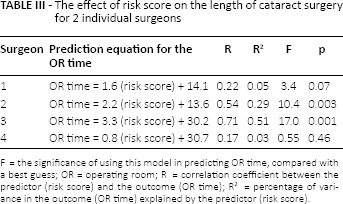
F = the significance of using this model in predicting OR time, compared with a best guess; OR = operating room; R = correlation coefficient between the predictor (risk score) and the outcome (OR time); R2 = percentage of variance in the outcome (OR time) explained by the predictor (risk score).
Complications
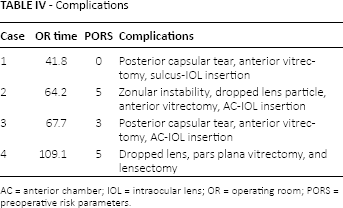
AC = anterior chamber; IOL = intraocular lens; OR = operating room; PORS = preoperative risk parameters.
Discussion
In this study, we implemented a stratifying risk system to assign preoperative risk to each patient and to calculate OR time using dedicated software. Although the PORS was initially applied to predict complications during cataract surgery, using the PORS may also allow better prediction of operating time as patients in the high-risk group had significantly longer surgeries. This work adds to the observation of Wright et al (9) that an experienced ophthalmic surgeon can predict, with high accuracy, the OR time based on case complexity. In addition, similar to the observation by Strum et al (10), we also noticed that surgeon skill predominated in determining OR time. Using the PORS, we were able to calculate the effect of every risk point on OR time for a specific surgeon, raising the possibility of using this tool for individual OR planning.
We have shown the feasibility of implementing dedicated software that could aid in improving operation time scheduling. The software is free to download and can assist individual surgeons with scheduling with a few steps of configuration.
Operating room time is a critical resource that generates high costs for a medical center (11). Therefore, optimally allocating OR time and planning for staff can maximize OR efficiency (12). As previously estimated, 1 minute of cataract surgery costs $11.24 (13); prediction of OR time may lead to improvement in surgical throughput (number of cases per unit time), reduced hospital cost, and improved patient care and satisfaction (14). Moreover, high-risk patients with pulmonary or orthopedic disorders could consider general anesthesia for longer surgery periods.
For 2 surgeons in our center, the PORS significantly contributed to the variability of OR time (29% and 51%), almost achieved a significant prediction for the third surgeon (p = 0.07), and was not helpful in prediction for the fourth surgeon. This may be due to the small number of cases but also to an inherent limitation of the PORS system, as risks are not fully characterized. For example, PXF on the pupil margin with dilated pupil diameter of 8 mm will receive 3 risk points but may not increase OR time as much as an extensive PXF on the lens capsule with zonular instability, which will receive the same number of risk points. Further amendments to the PORS system could be further incorporated in order to fine-tune this system. As demonstrated in Table IV, complications and longer OR time also were observed in not-high-risk patients, suggesting that the PORS cannot predict exactly how long each case will take. Hoverer, results from this study may serve as a basis for designing a surgery scheduling system based on the clinical skill of a given surgeon and patient individual risk.
In conclusion, this study examined predictors for cataract surgery time. Our results can be considered in surgery planning and preparation in order to allocate OR time considering cases with higher PORS.
Footnotes
Financial support: No financial support was received for this submission.
Conflict of interest: None of the authors has conflict of interest with this submission.