
Abstract
Purpose
To evaluate the psychological impact and depression prevalence in patients with Stargardt disease.
Methods
We conducted a case-control study including 39 patients with Stargardt disease and 32 age- and sex-matched healthy controls. All participants underwent a complete ophthalmologic examination and completed the Patient Health Questionnaire-9 (PHQ-9) and the Zung Depression Inventory questionnaire. Results were analyzed using IBM SPSS 22.0 software.
Results
The patient group consisted of 19 men and 20 women with mean age of 36.9 ± 5.4 years and control group of 19 men and 13 women with mean age of 42.5 ± 10.1 years. The mean values of PHQ-9 and Zung scores for patients and healthy individuals were 10.9 ± 4.9, 46.7 ± 11.1, 6.7 ± 5.4, and 41.1 ± 8.5, respectively. There were statistically significant differences between the 2 groups in PHQ-9 scores (independent samples t test: p = 0.001), but not in Zung scores (Mann-Whitney test: p = 0.053). The PHQ-9 and Zung scores appeared to be moderately but significantly correlated (Pearson coefficient 0.44, p<0.0001). In addition, PHQ-9 score seems to be raised along with age, whereas both scores are low when best-corrected visual acuity is high.
Conclusions
Patients with Stargardt disease exhibited more depressive symptoms compared to healthy individuals according mainly to PHQ-9 scores. Moderate depression was significantly correlated visual function decline.
Introduction
Stargardt disease is the most common juvenile macular dystrophy, with a prevalence of 1:10,000, mostly inherited by autosomal recessive trait. Symptoms typically appear in the first or second decade of life, including rapid, irreversible, bilateral, central vision loss; visual acuity in many cases may be lower than 20/200 (1, 2). Poor vision affects patients’ quality of life and numerous previous studies reveal high prevalence of depression among visually impaired patients (3-6). However, the correlation among vision loss, visual acuity, and depression remains controversial. Hayman et al (7) stated that visual function is associated with depression, but visual acuity is not, in contrast with Branch et al (8), who supported that positive correlation between visual acuity and severity of depression exists in visually impaired patients.
Depression has a great impact on both the patient and the family, is a major risk factor for suicidal behavior, and is costly in terms of days lost and medication cost; thus, it is important to detect and correlate depression symptoms and severity with visual function in vulnerable cohorts, such as visually impaired patients (9-11). The purpose of this study is to assess potential correlation between depression and visual impairment in patients with Stargardt disease, by using specific questionnaires, and to compare them with a group of healthy, unrelated controls without ophthalmic diseases who underwent the same procedure.
Methods
This study included 39 patients with Stargardt disease and 35 age- and sex-matched unaffected healthy controls. All patients were diagnosed with Stargardt disease for at least 20 years before the questionnaires were performed. At presentation, diagnosis was confirmed based on family history, fundus examination, and electroretinography recordings according to the International Society for Clinical Electrophysiology of Vision. Patients were recruited from the Greek Society of Retinopathies, a nonprofit organization for low-vision patients, including patients with Stargardt disease. All patients were examined at the Laboratory of Electrophysiology, 1st Department of Ophthalmology, University of Athens, Greece. The purpose and procedure of this study was explained and written consent was obtained from all participants. The protocol used was approved by the ethics committee of the University Hospital.
All participants underwent a thorough ophthalmic examination. Best-corrected visual acuity (BCVA) was assessed using Snellen charts and scores were converted in a logarithm of the minimum angle of resolution scale for statistical purposes. Anterior segment was examined using slit-lamp and dilated funduscopy using 78D stereoscopic fundus lenses was performed. Spectral-domain optical coherence tomography and fundus autofluorescence examination were used in order to confirm diagnosis and evaluate the extent of Stargardt disease (12, 13). Patients and controls completed the Zung Depression Inventory questionnaire and the Patient Health Questionnaire-9 (PHQ-9). The patients took the questionnaires for the first time in the context of this study.
The Zung Depression Inventory is a 20-question self-rating scale concerning emotional, behavioral, cognitive, and somatic depression symptoms. The questionnaire was developed according to the most commonly found depression diagnostic criteria during patients’ interviews. Subjects rate each item according to how frequently they felt each during the preceding week, rating (1) for none of the time or infrequently to (4) for most of the time or all the time. Summing scores for all individual items gives a total score ranging from 20 to 80. The following classification is suggested by the author: subjects with a score below 49 are considered normal, those scoring between 50 and 59 are considered to have mild depression, those scoring between 60 and 69 are considered to have moderate to marked depression, and those scoring 70 and above are considered to have severe depression (14-16).
The PHQ-9 is the depression module that scores each of the 9 criteria of the Diagnostic and Statistical Manual of Mental Disorders-IV (DSM-IV) (17). It can be used to detect depression symptoms in the high-risk population and monitor the severity of depression (18). The questionnaire consists of 9 items assessing the patient's emotional condition over the past 2 weeks. These items include (1) anhedonia, (2) depressed mood, (3) insomnia or hypersomnia, (4) fatigue or loss of energy, (5) appetite disturbances, (6) guilt or worthlessness, (7) diminished ability to think or concentrate, (8) psychomotor agitation or retardation, and (9) suicidal thoughts. Answers are rated 0 for not at all to 3 for nearly every day. Summing answer scores of all 9 items gives a total score that ranges from 0 to 27, with higher scores indicating presence of more severe symptomatology. According to the score, the classification suggested by Kroenke et al (19) is as follows: minimal (PHQ-9 score 0-4), mild (PHQ-9 score 5-9), moderate (PHQ-9 score 10-14), and moderately severe/severe (PHQ-9 score ≥15) depressive symptoms (19). Validity of the PHQ-9 as a useful depression detection tool has been assessed and well-established by studies using large population samples over the past decades (20, 21).
The statistical program IBM SPSS Statistics 22.0 (Armonk, NY, USA) was used for the analysis. Descriptive analysis of all parameters, including age, sex, BCVA, and PHQ-9 and Zung scores, was carried out. Box plots are presented for the quantitative variables. Nonparametric Kolmogorov-Smirnov analysis was used to check the normal distribution of all variables. The possible sex differences between healthy individuals and patients were estimated using the chi-square test. Independent samples t test and Mann-Whitney test were applied to identify possible differences in age, BCVA, and PHQ-9 and Zung scores between 2 groups (Mann-Whitney test was used when there was no indication of normal distribution either after Kolmogorov-Smirnov analysis or after Levene test for equality of variances). Finally, the age, BCVA, and PHQ-9 and Zung scores were correlated using Pearson and Spearman coefficients.
Results
Demographics
A total of 39 patients with Stargardt disease and 32 healthy unrelated controls were recruited in this study. The patient group consisted of 19 men and 20 women with mean age of 36.9 ± 5.4 years, ranging from 25 to 45 years. The control group consisted of 19 men and 13 women with mean age of 42.5 ± 10.1 years. Both groups’ demographic characteristics, including mean age, BCVA, and PHQ-9 and Zung scores, are presented in Table I and Figures 1-4. According to Kolmogorov-Smirnov analysis, sex, BCVA, and PHQ-9 and Zung scores exhibit normal distribution (p = 0.635, p = 0.200, p = 0.176, and p = 0.200, respectively), whereas age does not (p = 0.013). There are no differences in sex (chi-square test, p = 0.370) or age (Mann-Whitney test, p = 0.070) distribution between the 2 groups. The mean values of PHQ-9 and Zung scores in patients with Stargardt disease classify them as moderately depressive or normal.
Demographics and clinical data of patients and controls
BCVA = best-corrected visual acuity; logMAR = logarithm of the minimum angle of resolution; PHQ-9 = Patient Health Questionnaire-9.
Values are mean ± SD.
Box plot. The mean values of participants’ age (in years) for each group separately. The mean, the minimum, and the maximum values of the age are presented for each group.
Box plot. The mean values of participants’ best-corrected visual acuity (BCVA) (in logarithm of the minimum angle of resolution [logMAR]) for each group separately. The mean, the minimum, and the maximum values of BCVA are presented for patients’ group, while BCVA is constant in healthy individuals’ group for both eyes.
Box plot. The mean values of participants’ Patient Health Questionnaire-9 (PHQ-9) scores for both groups separately. The mean, the minimum, and the maximum values of the score are presented for each group.
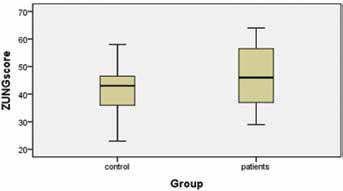
Box plot. The mean values of participants’ Zung scores for both groups separately. The mean, the minimum, and the maximum values of the score are presented for each group.
Assessment of BCVA and PHQ-9 and Zung scores
The BCVA differed between the 2 groups as expected (Mann-Whitney test, p<0.0001), even if we evaluate BCVA separately for each eye (Mann-Whitney test, p<0.0001 for right and left eyes). There are also statistically significant differences between the 2 groups in PHQ-9 scores (independent samples t test, p = 0.001), but the differences in Zung scores are not statistically significant (Mann-Whitney test, p = 0.053). The PHQ-9 and Zung scores seem to be moderately but significantly and positively correlated (Pearson coefficient 0.44, p<0.0001). Moreover, age presents moderate and positive correlation with the PHQ-9 score (Spearman coefficient 0.46, p<0.0001) but not with the Zung score (Spearman coefficient 0.13, p = 0.293). Finally, BCVA is significantly, positively, and moderately correlated with both PHQ-9 and Zung scores (Pearson coefficient 0.62, p<0.0001 and Pearson coefficient 0.57, p<0.0001, respectively).
Discussion
In this study, we evaluated PHQ-9 and Zung scores, which were conducted among 39 patients with Stargardt disease and 32 healthy age- and sex-matched individuals. The differences in mean values of PHQ-9 score were statistically significant between the 2 groups, while the Zung score differences were marginal. The PHQ-9 and Zung scores were obviously increased in parallel. In addition, PHQ-9 score seemed to be raised along with age, whereas both scores were low when BCVA was high. Patients with Stargardt disease exhibited more depressive symptoms compared to healthy individuals. However, the mean values of PHQ-9 and Zung scores in patients with Stargardt disease classified them as moderately depressive or normal.
The impact of low vision on mental health and quality of life has been identified even in patients with mild vision impairment. The Depression Anxiety Stress Scales (DASS) and Low Vision Quality of Life Questionnaires (LVQoL) were used to estimate the effect of low vision (BCVA for distance vision: OD 6/48 and OS 6/38, BCVA for near vision at 20 cm: OD N24 and OS N16) in a patient with tractional retinal detachment secondary to diabetic retinopathy (22). Low vision aids, psychological support, and occupational therapy were offered to the patient, who underwent the tests 3 months later. Although visual acuity, subjective refraction, and visual field status were unchanged, both tests were significantly improved (DASS stress level: from extremely severe [score 34] to normal [score 14], DASS depression level: from extremely severe [score 38] to normal [score 18], and LVQoL: from moderate [score = 43] to normal [score = 98]) (22).
A recent cross-sectional study included 162 patients with visual acuity less than 6/12 in order to appreciate the relation between vision-specific distress and depressive symptoms (23). The Impact of Vision Impairment Questionnaire and the PHQ-9 were used along with vision-specific functioning, social support, and Coping Strategy Indicator, which refers to the ability to deal with any condition. Poor vision-specific functioning, low confidence in managing social interactions, and depressive symptoms were determined as risk factors for vision-specific distress (23). In addition, this distress was strongly correlated to patients’ depression (23). The importance of physical and social functioning as well as vision rehabilitation can prevent depressive symptoms and ameliorate quality of life (24-27). Students with low vision attending special schools exhibit worse adaptive behavior compared to students in mainstream schools (28).
All patients with visual problems should be identified early. In addition, they should be educated for low vision aids and practical strategies in order to strengthen their self-confidence and daily autonomy (29-31). Many patients deny receiving any treatment due to depression, which therefore should be diagnosed early (32). Difficulties in reading, driving, and recognizing faces deteriorate the quality of life of patients with Stargardt disease, favoring the depressive feelings (33). Visual dysfunction can be present in patients with depressive and anxiety symptoms, even if it is not consistent with the severity of eye lesions and the general health status, highlighting the demand for visual rehabilitation and social and psychological support (34-36). Moreover, patients aged 65 years and older experiencing low vision problems exhibit higher incidence of physical and mental comorbidities compared to individuals of similar age without optical dysfunction (37). Ophthalmologists, optometrists, and other professionals should be aware of mental and social effects of low vision, in order to identify relative problems and refer patients with visual dysfunction for mental support (38). The Geriatric Depression Scale can assess depressive symptoms presenting in elderly individuals with low vision, if these measurements are evaluated in parallel with visual acuity and disability (39, 40).
Mental treatment and support should never be discontinued, keeping in mind that the mood of these patients varies according to their visual acuity, disease severity, as well as autonomy in daily activities and interpersonal relationships (41). However, specific features such as a history of a depressive, dysthymic, or panic disorder, severe depression and anxiety at baseline, or reduced adaptation to visual dysfunction can make patient management difficult (42). Overall, professionals should participate in training programs considering low vision rehabilitation as well as diagnosis and management of depression in patients with visual loss (43). The care of blind people can burden professionals psychologically, and they also may need mental support (43, 44).
In our study, patients with Stargardt disease exhibited more depressive symptoms compared with healthy individuals and these symptoms appeared to be increased in parallel with the decline of visual function. However, the mean values of PHQ-9 and Zung scores in these patients classify them as moderately depressive or normal. The restriction of our study was the number of participants. Thus we aim to include more individuals in this study in order to define the possible physiologic impact of low vision in patients with Stargardt disease (45). Ophthalmologists and vision professionals should be educated to identify depressive symptoms and encourage patients to receive mental support and low vision aids. In addition, early detection could decrease suicidal behavior of the patients as well as medication cost (46-48).
Footnotes
Financial support: No financial support was received for this submission.
Conflict of interest: None of the authors has conflict of interest with this submission.