
Abstract
Purpose
To compare the efficiency of brinzolamide/brimonidine fixed combination vs the dorzolamide/timolol fixed combination.
Methods
Forty-four eyes of 44 patients were divided in 2 groups treated either with dorzolamide/timolol twice a day (group A) or with brinzolamide/brimonidine twice a day (group B). Complete ophthalmic examination including Goldmann applanation tonometry was performed before treatment administration and 1, 4, 8, and 12 weeks afterwards. The intraocular pressure (IOP) was measured twice a day (morning at 9
Results
At the end of the follow-up period (12 weeks), mean morning IOP reduction was 7.0 ± 2.8 mm Hg in group A and 8.4 ± 1.9 mm Hg in group B. A significant difference was found (p = 0.0343). In contrast, mean afternoon IOP reduction was 8.6 ± 2.7 mm Hg in group A and 7.9 ± 1.6 mm Hg in group B and no significant difference was found (p = 0.3413). No significant adverse effects were observed in either group.
Conclusions
Brinzolamide/brimonidine seems to be an effective and safe alternative β-blocker free fixed combination, especially for patients with comorbidities, having its own antihypertensive profile.
Introduction
Glaucoma is the second leading cause of vision loss worldwide. It is estimated that 8.7 million people are blind due to open-angle and angle-closure glaucoma (1). Intraocular pressure (IOP) is one of the most important parameters in the diagnosis and treatment of glaucoma. Topical β-blockers such as timolol have been widely used since the 1970s and they reduce IOP by decreasing aqueous humor secretion. The precise mechanism of action is presumed to be mediated via blockade of the β2 adrenergic receptors found in the ciliary body (2). Since then, newer treatments have become available, including carbonic anhydrase inhibitors such as dorzolamide and brinzolamide, prostaglandins such as latanoprost and travoprost, and α2 adrenergic agonists such as brimonidine. As these drugs reduce IOP through different pathways, they are often given as combinations, for example, the combination of dorzolamide 2% and timolol 0.5%, which is available in a fixed single-dose preparation (Cosopt®; Merck & Co., Inc., Kenilworth, NJ), which is more effective at reducing IOP than either of its components given alone (3).
The purpose of this study is to compare the efficiency of the new brinzolamide/brimonidine fixed combination (BBFC; Simbrinza™; Alcon Laboratories, Fort Worth, TX) vs the dorzolamide/timolol fixed combination (DTFC; Cosopt®).
Methods
This was a prospective, randomized, double-masked, parallel-group study conducted at the University General Hospital of Evros during May and October 2015. The study protocol adhered to the tenets of the Declaration of Helsinki; all study participants provided written consent.
Forty-four eyes of 44 patients were recruited and randomly populated 2 study groups. Group A was treated with DTFC bid and group B with BBFC bid.
All subjects were patients with newly diagnosed primary open-angle glaucoma (POAG) or patients with POAG previously treated with other medications with a washout period of 1 month. The number of naive patients and patients previously treated with other medications was equal in both groups (Tab. I). Patients with previous eye operations or types of glaucoma other than POAG were excluded from the study. Other exclusion criteria were age <18 years, IOP >36 mm Hg at any timepoint, pregnancy, Schaffer angle grade <2 (in gonioscopy), cup-to-disc ratio >0.8, severe central visual field loss, history of chronic, recurrent, or current severe inflammatory eye disease, ocular trauma, ocular infection or inflammation, any retinal disease, any factor that could affect the compliance of the patient (illness, allergies), and any β-blocker contraindication for patients of group A.
Demographic characteristics of both groups
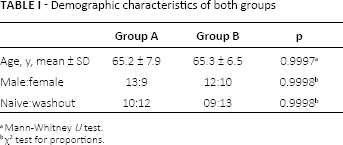
Mann-Whitney U test.
χ2 test for proportions.
Complete ophthalmic examination including Goldmann applanation tonometry was performed before treatment administration and 1, 4, 8, and 12 weeks afterwards. The IOP was measured twice a day (9
Data were collected and analyzed using MedCalc 15.0 (MedCalc Software, Ostend, Belgium). Data normality was tested using Shapiro-Wilk test and parametric and nonparametric tests were applied accordingly. p Values below 0.05 were considered statistically significant.
Results
Demographics
Each group consisted of 22 patients. One eye of each patient was included in the study. Mean age was 65.2 ± 7.9 years in group A and 65.3 ± 6.5 years in group B; no significant difference was observed (Mann-Whitney U test, p = 0.9997). Male to Female ratio was 13:9 and 12:10 in groups A and B, respectively; no significant difference was observed (χ2 for proportions, p = 0.9998).
Morning IOPs
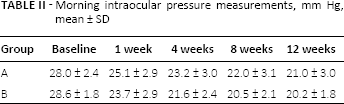
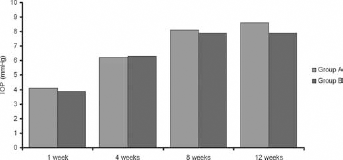
Baseline morning IOP was 28.0 ± 2.4 mm Hg in group A and 28.6 ± 1.8 mm Hg in group B; no significant difference was observed (unpaired t test, p = 0.3536). At the end of the follow-up period (12 weeks), mean morning IOP in group A was 21.0 ± 3.0 mm Hg and in group B 20.2 ± 1.8 mm Hg and the mean IOP reduction was 7.0 ± 2.8 mm Hg in group A and 8.4 ± 1.9 mm Hg in group B. A significant difference was observed (Mann-Whitney test, p = 0.0343). Detailed status of the morning IOP and IOP reduction in both groups is depicted in Tables II and III and in Figures 1 and 2.
Morning intraocular pressure measurements, mm Hg, mean ± SD
Morning intraocular pressure (IOP) reduction compared to baseline IOP, mm Hg, mean ± SD
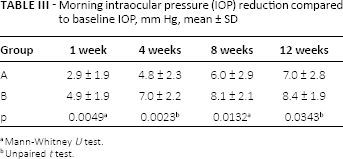
Mann-Whitney U test.
Unpaired t test.
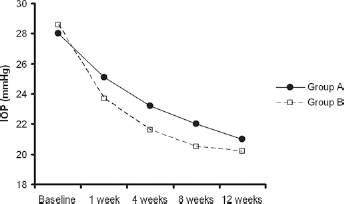
Changes of the morning intraocular pressure (IOP) in both groups over time.
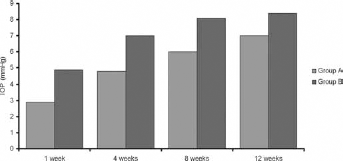
Morning intraocular pressure (IOP) reduction in both groups.
Afternoon IOPs
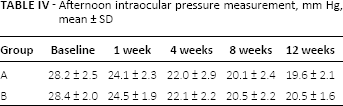
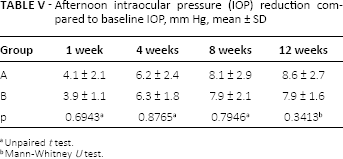
Baseline afternoon IOP was 28.2 ± 2.5 mm Hg in group A and 28.4 ± 2.0 mm Hg in group B; no significant difference was observed (Mann-Whitney test, p = 0.9798). At the end of the follow-up period (12 weeks), mean afternoon IOP in group A was 19.6 ± 2.1 mm Hg and in group B 20.5 ± 1.6 mm Hg and the mean IOP reduction was 8.6 ± 2.7 mm Hg in group A and 7.9 ± 1.6 mm Hg in group B. No significant difference was observed (Mann-Whitney test, p = 0.3413). Detailed status of the afternoon IOP and IOP reduction in both groups is depicted in Tables IV and V and in Figures 3 and 4.
Afternoon intraocular pressure measurement, mm Hg, mean ± SD
Afternoon intraocular pressure (IOP) reduction compared to baseline IOP, mm Hg, mean ± SD
Unpaired t test.
Mann-Whitney U test.
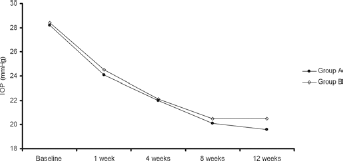
Changes of the afternoon intraocular pressure (IOP) in both groups over time.
Afternoon intraocular pressure (IOP) reduction in both groups.
No differences in conjunctival hyperemia, ocular stinging, soreness or irritation, or foreign body sensation (9.1% of patients [2 individuals] in each group) were observed between the 2 groups.
Discussion
In the current study, we compared 2 fixed combinations of carbonic anhydrase inhibitor (CAI) with a β-blocker (Cosopt®) and an α2 adrenergic agonist (Simbrinza™). Both of these drugs offer the same hypotensive effect in the morning and afternoon. The IOP reduction in the morning was 7.0 ± 2.8 mm Hg for the dorzolamide/timolol group and 8.4 ± 1.9 mm Hg for the brinzolamide/brimonidine group. The IOP in the afternoon was reduced by 8.6 ± 2.7 mm Hg in group A and 7.9 ± 1.6 mm Hg in group B.
The presence of brimonidine instead of timolol in the fixed combination does not affect its efficacy, although the β-blocker has been shown to have a higher hypotensive profile compared to the α2 agonist (4, 5). This can be explained by the dual mode of action of brimonidine, which acts on both aqueous production and the facilitation of the uveoscleral outflow (6). It seems that brimonidine has a powerful additive effect when compared with the brinzolamide, which complements its action and outweighs brimonidine's lower hypotensive effect when used as monotherapy.
The hypothesis of the additive effects of the 2 constituents of Simbrinza™ is supported by the fact that Simbrinza™ has a lower concentration of benzalkonium chloride (0.03 mg/mL) than Cosopt® (0.075 mg/mL). Benzalkonium chloride (BAC) increases drug penetration through corneal epithelium by breaking cell-cell junction between the epithelial cells (7). However, its use has been associated with increased incidence of ophthalmic surface disease in glaucoma patients (7, 8) and impacts adversely on quality of life (9). The lower concentration of BAC in the Simbrinza™ formulation can potentially have fewer ocular side effects without compromising its potency as these side effects are dose-dependent (10).
Our study did not reveal any differences in the frequency of side effects between dorzolamide/timolol and brinzolamide/brimonidine fixed combinations. This can be attributed to the small number of patients included in each group.
Another advantage of the brinzolamide/brimonidine combination is the absence of the side effects that can be caused by β-blockers. In fact, it is the only fixed combination marketed that does not contain a β-blocker. β-Blockers can cause or exacerbate previous pulmonary and heart disorders and are contraindicated in these patients. Up to 60% of patients needing antiglaucoma topical treatment can be excluded from being prescribed a β-blocker (11). Consequently, the brinzolamide/brimonidine formulation offers the benefits of a fixed combination to a large number of patients previously excluded from such a medication. These benefits include reduced exposure to preservatives, washing out of the second medication if no adequate time is allowed between drops, reduced frequency of symptoms related to ophthalmic surface disease, and fewer drop instillations with a similar hypotensive profile (12).
To our knowledge, this is the first study that compares 2 different fixed combinations both containing an CAI inhibitor. The brinzolamide/brimonidine formulation is the only non-β-blocker fixed combination available in the market. Our study has shown similar hypotensive effect and safety profile as the fixed formulation of dorzolamide/timolol. The limitations include the small number of patients in each group and the fact that IOP was measured at 2 specific timepoints (morning and afternoon) and we did not perform a 24-hour phasing. If the sample size was larger, the dorzolamide/timolol fixed combination would possibly be significantly more potent in the afternoon times; however, the preliminary results of our study show that Simbrinza™ seems to be an effective and safe alternative β-blocker-free fixed combination.
Footnotes
Financial support: No financial support was received for this submission.
Conflict of interest: None of the authors has conflict of interest with this submission.