
Abstract
Purpose
To evaluate the potential efficacy and safety of primary intravitreal ranibizumab in patients with symptomatic retinal arterial macroaneurysm (RAM).
Methods
This prospective study comprised 5 eyes with RAM treated with intravitreal ranibizumab. At baseline, all patients underwent best-corrected visual acuity (BCVA) measurement, ophthalmic examination including slit-lamp biomicroscopy, and central foveal thickness (CFT) measurement using optical coherence tomography. Fluorescein angiography was also performed to confirm diagnosis. Patients were examined at 1 month after injection and monthly thereafter. Main outcome measures included changes in BCVA and CFT. Safety was assessed by ophthalmic examination and report of systemic adverse effects.
Results
There was a statistically significant difference in BCVA (p<0.001) and CFT (p<0.001) before and after the ranibizumab injection at the end of the follow-up of 13.4 ± 3.2 months. One injection appeared to be sufficient for the resolution of macular edema and absorption of hemorrhages. No observable ocular or systemic side effects were found. One patient developed foveal atrophy.
Conclusions
Intravitreal ranibizumab seems to be effective and safe for the treatment of symptomatic RAM.
Introduction
Retinal arterial macroaneurysm (RAM) is a localized fusiform or saccular vascular dilation of a retinal arteriole, usually occurring within the first 3 orders of bifurcation in the macular or postequatorial areas and at an arteriovenous crossing most commonly on a temporal vascular arcade (1). Retinal arterial macroaneurysm has a predilection for hypertensive women aged between 50 and 80 years, while dyslipidemia has been also associated with RAM (1, 2). It is usually solitary, involving only one eye in about 90% of cases (3). Although most cases are quiescent or have a benign course with spontaneous involution, not requiring any intervention, others may lead to visual loss due to complications, such as macular edema or hemorrhage (1, 2).
The treatment of RAM remains controversial and current treatment modalities did not seem to improve visual acuity. Observation is a reasonable treatment option for asymptomatic RAMs. Other treatment alternatives include direct laser photocoagulation to the RAM itself if there is foveal involvement, pneumatic displacement with tissue plasminogen activator (tPA) for submacular hemorrhage, surgical removal of associated hemorrhage with vitrectomy, and photodisruption of the internal limiting membrane or the posterior hyaloid using YAG laser to release the hemorrhage (1).
Nowadays, in the era of anti-vascular endothelial growth factor (VEGF) treatment, there have been several reports suggesting the use of intravitreal bevacizumab or ranibizumab for the treatment of RAM, showing encouraging results, but having limited follow-up time (4–5–6–7–8–9–10–11–12–13–14–15). In light of the above, the purpose of this study was to evaluate the anatomical and functional results after intravitreal ranibizumab injections for the treatment of symptomatic RAM in a long-term follow-up.
Methods
This prospective observational study comprised 5 eyes of 5 treatment-naive patients with symptomatic RAM, defined as RAM with exudative foveal manifestations, such as subretinal or intraretinal fluid, exudates, and/or hemorrhages, treated with intravitreal ranibizumab (Lucentis®; Novartis International AG, Basel, Switzerland). Exclusion criteria were any of the following: history of any intraocular surgery within 3 months before enrollment to the study, other ocular diseases that could affect visual acuity, and RAM without macular edema or hemorrhage. Written informed consent was obtained by all participants. The study was in accordance with the tenets of the Declaration of Helsinki and was approved by the institutional review board.
At baseline, all patients underwent best-corrected visual acuity (BCVA) measurement by means of Snellen charts, ophthalmic examination including slit-lamp biomicroscopy, and central foveal thickness (CFT) measurement using optical coherence tomography (OCT). Spectral-domain OCT (Heidelberg Spectralis; Heidelberg Engineering, Heidelberg, Germany) was used for all measurements. Fluorescein angiography using Spectralis was also performed to confirm diagnosis. Visual acuity was converted to logMAR scale for statistical analysis.
All patients received at least 1 intravitreal injection of 0.5 mg/0.05 mL ranibizumab, after being informed about the treatment options for RAM and about the off-label use of ranibizumab, as well as the potential risks and benefits. All the injections were performed under standard sterile conditions. Topical antibiotics were administered to all patients 4 times a day for 1 day before and for 5 days after the injection. After the first injection, patients were retreated if there was persistent fluid/hemorrhage or active RAM involving the macula on OCT at least 1 month after the previous injection or if there was visual deterioration of more than 2 lines.
Patients were examined monthly after injection until 6 months and every 3 months thereafter. At each visit, complete eye examination was performed, including BCVA measurement, funduscopy, and CFT measurement. Fluorescein angiography was performed only at the examiner's discretion and not at every postinjection evaluation. Recurrence was defined as a decrease of BCVA >2 Snellen lines, an increase in CFT >100 μm on OCT, or presence of new hemorrhage/fluid, after a previous favorable response with complete or partial resolution in previous follow-up visits.
The main outcome measures included changes in BCVA and CFT. Safety was assessed by ophthalmic examination. Data were analyzed using Mann-Whitney-Wilcoxon test for comparisons of BCVA and CFT pretreatment and posttreatment. A p value of <0.05 was considered significant. Statistical analysis was performed using SPSS 22.0 (SPSS, Inc., Chicago, IL, USA).
Results
The patients’ characteristics are shown in Table I. Of the 5 patients, 4 were female and 1 was male. The mean age of the patients was 73.4 ± 8.6 years. The mean follow-up time was 13.4 ± 3.2 months (range 9-17 months).
Patient characteristics
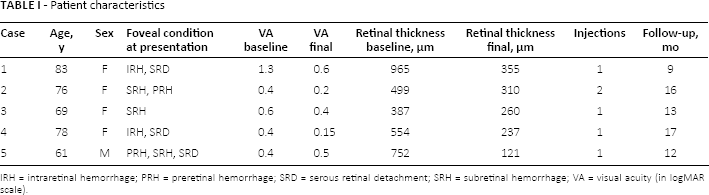
IRH = intraretinal hemorrhage; PRH = preretinal hemorrhage; SRD = serous retinal detachment; SRH = subretinal hemorrhage; VA = visual acuity (in logMAR scale).
The mean BCVA at baseline was 0.62 ± 0.39 logMAR (mean ± SD, range 0.4-1.3). At month 12, the mean BCVA was 0.36 ± 0.21 logMAR and differed significantly compared to baseline (p = 0.02), while at the end of the follow-up, the mean BCVA was 0.37 ± 0.19 logMAR (range 0.15-0.6), which differed significantly compared to baseline (p<0.001). Figure 1 shows the progression of BCVA over time.
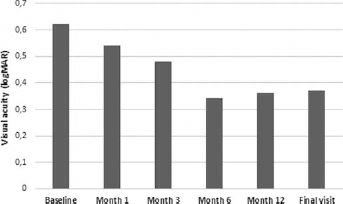
Visual acuity evolution over time.
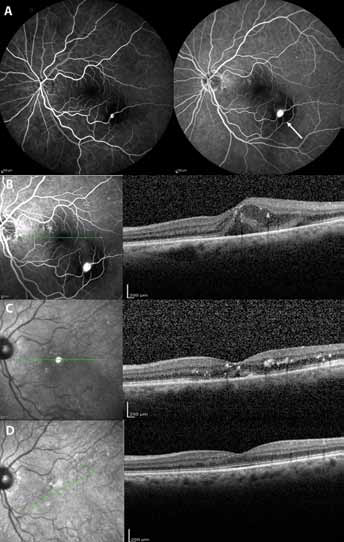
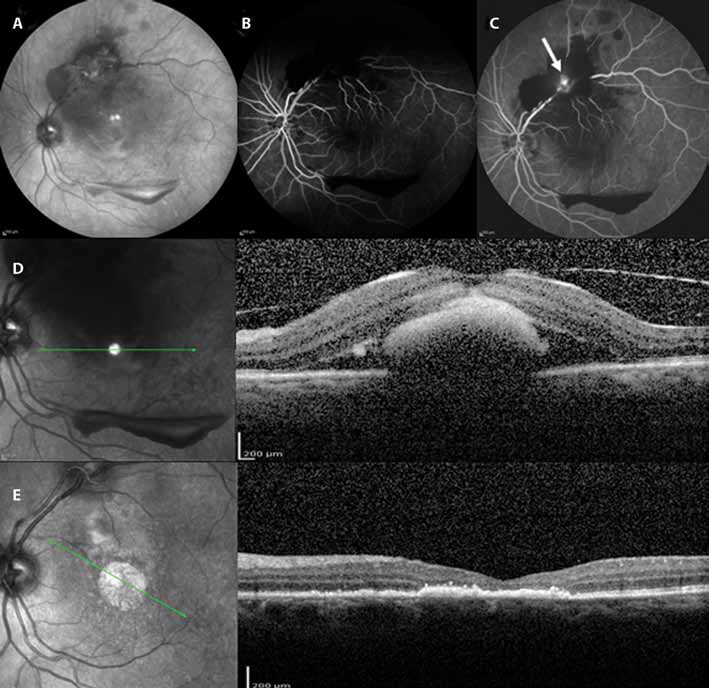
At baseline, the mean CFT was 631.4 ± 228.6 μm (mean ± SD, range 387-950 μm). At month 12, the mean CFT was 279.1 ± 102.5 μm and there was a statistically significant difference compared to baseline (p<0.001). At the end of the follow-up, the mean CFT was 256.6 ± 88.5 μm (range 121-355), which also differed significantly from baseline (p<0.001). Figure 2 depicts the progression of CFT over time. In addition, resolution of the associated preretinal, intraretinal, and subretinal hemorrhage occurred in all patients. Figures 3 and 4 show 2 cases of our study and their progression after intravitreal ranibizumab injection. All patients received a single injection, except 1 who needed an additional injection due to persistence of hemorrhage.
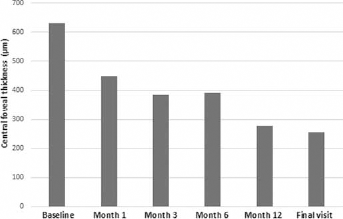
Central foveal thickness evolution over time.
(
(
No observable ocular side effects were found, such as inflammation, infection, increased intraocular pressure, retinal tear, or detachment. It is noteworthy that one patient showed diffuse retinal pigment epithelium atrophy after treatment, despite complete RAM obliteration and resolution of hemorrhage.
Discussion
The principal message of this case series is that intravitreal ranibizumab can offer favorable anatomical and functional results in treatment-naive patients with symptomatic RAM, showing significant decrease of CFT and absorption of hemorrhage, as well as significant increase in visual acuity.
The management of RAM remains controversial. Retinal arterial macroaneurysm is considered to be a benign condition, which may resolve spontaneously, presenting functional recovery. However, exudative RAM causes visual impairment when the fovea is committed by macular edema, serous retinal detachment, or hard exudates. In addition, the chronicity of exudation or hemorrhage lead to progressive damage of photoreceptors with permanent visual disturbance (16). Therefore, in cases of symptomatic RAM with foveal involvement, early intervention is recommended to avoid irreversible functional loss.
Laser photocoagulation is the most common treatment modality for RAM. Nevertheless, the various complications of the technique, such as choroidal neovascularization, fibrosis, enlargement of laser scar, increase of retinal exudation, and possible retinal traction, have limited the use of laser (17). Since the visual prognosis of untreated subretinal hemorrhage due to RAM can be very poor, other treatment alternatives have been used for RAM, such as tPA and/or vitrectomy in cases of submacular hemorrhage, or YAG laser disruption of the posterior hyaloid to release the hemorrhage (1).
Intravitreal anti-VEGF injections are more recent therapeutic alternatives, being shown to reduce vascular permeability, normalize central retinal thickness, and lead to visual stabilization or slight improvement (1, 4–5–6–7–8–9–10–11–12–13–14–15). In our case series, intravitreal ranibizumab was found to improve visual acuity from 0.62 to 0.37 logMAR and provide anatomical recovery by decreasing macular edema from 631.4 to 256.6 μm at the long-term follow-up of 13.4 ± 3.2 months, as well as promoting the absorption of hemorrhages.
The mechanism though which ranibizumab seems to be effective in the treatment of RAM is not known, but it is hypothesized to be associated with the pathogenesis of RAM. Age causes changes in the arterioles, as intimal collagen replaces smooth muscle fibers and the arterial wall becomes less elastic, leading to susceptibility of the vessels to dilation from elevated hydrostatic pressure (18). Additionally, focal embolic damage to arterial walls is thought to cause RAM. As a result, localized ischemia and VEGF upregulation leads to VEGF-associated increased permeability and dilation of the artery, causing macular edema and hard exudates (1).
Anti-VEGF can prevent the formation of abnormal blood vessels and counteract VEGF-induced vascular permeability (4). The resolution of macular edema and exudation after anti-VEGF injection in RAM can be attributed to 2 potential mechanisms. First, intravitreal ranibizumab blocks the angiogenic and vasopermeability effects of VEGF (19). Vascular endothelial growth factor stimulates endothelial production of nitric oxide, a vasodilator, while anti-VEGF reduces nitric oxide, leading to vasoconstriction, reducing macular edema independent of the effect on vascular permeability (12). Second, VEGF is known to be associated with activation of coagulation cascade (20). Inhibition of VEGF by ranibizumab may break down the balance between the coagulation and fibrinolysis processes, promoting clearing of the various retinal hemorrhages (1). In any case, it remains uncertain if these effects of anti-VEGF could affect the RAM per se.
It is also worthy to note that patients with hemorrhagic RAM have a better visual prognosis than patients with exudative RAM, and the poorest outcomes are observed when macular edema and exudates persist for several months (21). In fact, subretinal hemorrhage causes damage to the overlying retina and subretinal blood can be toxic, especially in the macular area. The outer retinal toxicity associated with subretinal hemorrhage is presumably caused by 3 factors: a mechanical barrier effect that prevents metabolic exchange between the retinal pigment epithelium and outer retina, iron-related toxicity, and fibrin-mediated retinal damage (4, 22). Hemorrhage from RAM, unlike exudation, is a one-time event that commonly leads to fibrosis and occlusion of RAM. In our case series, one patient developed atrophy after treatment with subsequent irreversible decrease in visual acuity, but this phenomenon could be potentially due to the natural course of the disease rather than due to the effect of intravitreal ranibizumab.
A potential limitation of this study is the small number of patients. It is nonrandomized and there is a lack of control group. However, our sample has a long-term follow-up and it is a prospective study.
In conclusion, our study suggests that intravitreal ranibizumab is well-tolerated in patients with symptomatic RAM, and provides a significant improvement in BCVA as well as a decrease in CRT on OCT. These favorable and promising results support the need for further studies to evaluate the safety and efficacy of intravitreal ranibizumab for this clinical entity.
Footnotes
Financial support: No financial support was received for this submission.
Conflict of interest: None of the authors has conflict of interest with this submission.