
Abstract
Purpose
To report a case of bilateral cavernous sinus thrombosis (CST) in a patient with tacrolimus-associated posttransplant thrombotic microangiopathy.
Methods
Case report.
Results
An 8-year-old boy with a medical history of orthotopic heart transplant, posttransplant lymphoproliferative disease, and recurrent infections was hospitalized for nausea, vomiting, and diarrhea. His ocular history included accommodative esotropia, hyperopia with astigmatism, Molluscum contagiosum lid lesions, and idiopathic intracranial hypertension. Shortly after presentation, he developed increased intraocular pressure, an afferent pupillary defect, a layered hyphema, and tense proptosis of the left globe requiring an emergent canthotomy and cantholysis. Over the next month, the patient's hospital course included subdural and subarachnoid hemorrhage, temporal lobe stroke, serotonin syndrome, bilateral CST, and systemic microangiopathy. After an extensive workup, a diagnosis of tacrolimus-associated thrombotic microangiopathy was made. At this point, vision was 20/20 in the right eye and light perception in the left eye. Eight months after the canthotomy and cantholysis, the patient's vision in the left eye deteriorated to no light perception and remained so after 13 months of follow-up.
Conclusions
An idiosyncratic drug reaction should be considered in the differential diagnosis of CST, especially in a patient on calcineurin inhibitors after solid organ transplant without sinus disease or orbital cellulitis.
Introduction
Tacrolimus has been used extensively for immunosuppression in patients post organ transplantation (1). It blocks interleukin-2, resulting in suppression of T-cell proliferation. Adverse effects range from nephrotoxicity to potentially life-threatening thrombotic microangiopathy (TMA) (2). The pathophysiology of tacrolimus-associated TMA includes endothelin-1-mediated vasoconstriction, tissue hypoxia, endothelial cell damage, and vessel thrombosis via deposition of platelets and fibrin. The definitive diagnosis involves high clinical suspicion, ruling out other causes of microvascular thrombosis, and tissue biopsy (2).
Cavernous sinus thrombosis (CST) is a rare manifestation of sinus disease and may result in significant neurologic and ophthalmologic morbidity, including cranial neuropathies, stroke, pituitary insufficiency, blindness, and even death (3, 4). The gold standard for diagnosis of CST includes contrast-enhanced magnetic resonance imaging or computed tomography (CT) (4). Prompt recognition and management with sinus surgery, several weeks of broad-spectrum antibiotics, and anticoagulation in select situations results in the highest likelihood of achieving a positive outcome.
To our knowledge, we report the first case of bilateral CST secondary to tacrolimus-associated TMA.
Case report
An 8-year-old boy had a medical history including renal tubular acidosis, bilateral pulmonary emboli (positive lupus anticoagulant), orthotopic heart transplant due to acute viral cardiomyopathy at 23 months of age, posttransplant lymphoproliferative disease, Cryptosporidium enteritis, Clostridium difficile colitis, and recurrent upper respiratory infections, fevers, sinusitis, and otitis media. Family history was not relevant.
He initially presented to ophthalmology at 4 years of age, with normal vision and ocular examination, and accommodative esotropia. At age 7, he developed idiopathic intracranial hypertension and was managed with acetazolamide. At age 8, he presented with nausea, vomiting, decreased oral intake, and diarrhea, and developed pelvic/penile congestion due to microvascular venous thrombosis. He was noted to have redness in the left eye, with intraocular pressure (IOP) of 48 mm Hg, periorbital edema, and layered hyphema. The patient was started on topical cycloplegics, steroids, and IOP-lowering drops. However, within a few hours he developed rapid tense proptosis of the left eye requiring lateral canthotomy and cantholysis to decompress the orbit.
The patient's condition deteriorated, requiring intubation and transfer to the intensive care unit. Head CT showed a subdural and subarachnoid hemorrhage and rectus muscle and ophthalmic vein engorgement. Magnetic resonance imaging/magnetic resonance angiography/magnetic resonance venography were significant for petechial anterior left temporal lobe hemorrhages, old left caudate infarct, and diminished caliber of the cavernous portion of internal carotid arteries (ICA). Computed tomography angiography of the head confirmed bilateral CST and ICA narrowing and left transverse sinus and ophthalmic vein thrombosis. Sinus biopsy showed microangiopathic process thought to be secondary to tacrolimus, which resulted in drug discontinuation and initiation of high-dose steroids and intravenous immunoglobulin. Notwithstanding, he developed compartment syndrome of the left upper extremity, and despite emergent fasciotomies and thrombectomy, elbow disarticulation was performed.
One month after the canthotomy and cantholysis, the patient had 20/20 vision in the right eye and light perception (LP) vision in the left eye. Fundus examination showed acute on chronic disc edema in the right eye with vessel tortuosity and peripapillary hemorrhages (Fig. 1A). Lumbar puncture revealed an opening pressure of 44 cm water, while neuroimaging did not reveal any recent strokes or sinus thrombosis/stenosis. The dose of acetazolamide was subsequently increased. A few weeks later, the lateral canthus was repaired, and the patient was discharged to a physical rehabilitation facility.
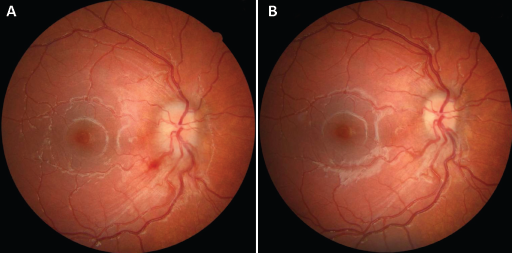
Fundus photographs of the right eye. (
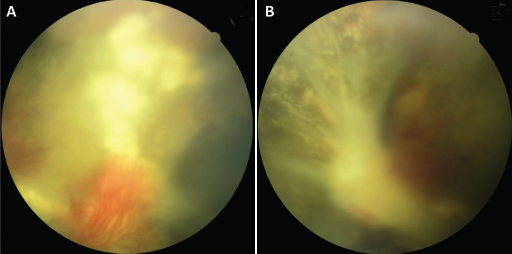
At last follow-up, the patient's vision was 20/20 in the right eye with decrease in optic nerve edema and resolution of intraretinal hemorrhages (Fig. 1B). Vision in the left eye was no LP (NLP) with examination significant for a dense cataract, disc neovascularization, and retinal folds (Fig. 2).
(
Discussion
Transplant-associated TMA develops secondary to infections, malignancy, autoimmune diseases, and medications (5). Based on analysis of 21 cases of tacrolimus-associated TMA, Trimarchi et al (2) showed the incidence to be 1%-4.7%, time to diagnosis 9.3 months, higher frequency in females, poor association with medication trough levels, mean age of 47 years, and 81% with kidney allografts. On the contrary, our patient was a young boy who underwent cardiac transplantation. His underlying predisposition to hypercoagulability may have exacerbated the systemic manifestations of tacrolimus-associated TMA. Our patient's persistent pancytopenia and recent stroke made the management of this rare clinical entity even more challenging as he was unable to be anticoagulated. Although the precise role of anticoagulation in patients with CST is not yet defined, it may decrease the rate of clot propagation as well as mortality (6).
Ocular manifestations of CST include ptosis, proptosis, periorbital sensory loss, exposure keratopathy, decreased pupillary response, ophthalmoplegia, decreased vision, and blindness (7). Frank et al (8) identified 9 cases of CST in children secondary to sinusitis. The majority had ophthalmoplegia and decreased vision, all 9 required sinus surgery, several needed an orbitotomy for abscess drainage, and 1 underwent bilateral exenteration. While an aggregate analysis of 52 cases of pediatric CST reported a morbidity rate of 25% and mortality rate of 8% (4), others have reported no permanent sequelae (9).
No LP vision is not uncommon in patients with CST and can occur secondary to orbital venous congestion, retinal ischemia, and optic neuropathy (8, 10). Several of these likely contributed to NLP vision in our patient. In addition, our patient had a critical narrowing of the ICA, which predisposed him to a significant ischemic insult. Although reversible ICA narrowing has been described previously (4), this phenomenon was not observed on our patient's imaging.
We report the first case in the literature of bilateral CST secondary to tacrolimus-associated TMA. Although our patient survived, he had myriad systemic sequelae including vision loss. An idiosyncratic drug reaction should be considered in the differential diagnosis of CST, especially in a patient on calcineurin inhibitors after solid organ transplant without sinus disease or orbital cellulitis.
Footnotes
Financial support: No financial support was received for this submission.
Conflict of interest: None of the authors has conflict of interest with this submission.