
Abstract
Purpose
To assess the effect of panretinal laser photocoagulation on ocular pulse amplitude (OPA) in normotensive eyes with proliferative diabetic retinopathy.
Methods
Prospectively, we performed unilateral argon laser panretinal photocoagulation (PRP) in 30 patients with diabetes mellitus type II and previously untreated bilateral proliferative diabetic retinopathy. Before and 7 and 30 days after the treatment, OPA was measured using dynamic contour tonometer.
Results
Compared with the untreated contralateral eyes, laser photocoagulation led to a reduction of OPA. Ocular pulse amplitude did not significantly differ in photocoagulated eyes 7 days after the treatment, but there was a significant difference in OPA 30 days after the treatment. The decrease in OPA values was 15% 7 days after PRP and 40% 30 days after PRP.
Conclusions
Ocular pulse amplitude reduction after PRP indirectly informs us about choriocapillary closure, already reported in previous studies.
Introduction
Diabetic retinopathy is a major cause of visual loss and blindness. The gold standard treatment for proliferative diabetic retinopathy treatment is panretinal laser photocoagulation. The impact of panretinal photocoagulation (PRP) on intraocular pressure (IOP) levels has been studied before (1–2–3) but the effect of PRP on ocular pulse amplitude (OPA) has rarely been the focus of reported investigations.
We examined the effect of PRP on OPA in normotensive eyes with proliferative diabetic retinopathy.
Methods
A total of 60 eyes of 30 consecutive patients with type 2 diabetes mellitus referred to a retina specialist for proliferative diabetic retinopathy treatment were included in this prospective study, Patients were included if they had high-risk proliferative retinopathy in both eyes, which was defined according to the guidelines of the Early Treatment Diabetic Retinopathy Study (4). The study was approved by the local ethics committee and informed consent according to the Declaration of Helsinki was obtained from each subject.
Exclusion criteria included (1) previous laser treatments; (2) prior vitreoretinal surgery (vitrectomy, intravitreal triamcinolone injection) in the study eye; (3) history of any thromboembolic event (including myocardial infarction or cerebral vascular accident); (4) major surgery within the prior 6 months; (5) glaucoma under treatment or elevated IOP (above 21 mm Hg Goldmann applanation tonometry); (6) known coagulation abnormalities or current use of anticoagulant medication other than aspirin; (7) evidence of external ocular infection (conjunctivitis, keratitis, or significant blepharitis); (8) refractive error ±3.0 SD; (9) history of antihypertensive medication use.
Data, collected by interview, included detailed ocular and medical histories, with particular attention to diagnosis, duration, and treatment of diabetes. Systemic blood pressure measurements were taken 3 times, with a minimum 5-minute interval between readings (Omron M3 intellisense, automated manometer; Omron Healthcare, Kyoto, Japan), and the mean blood pressure was noted. Diabetic patients reported current medical treatment for diabetes mellitus with oral hypoglycemic agents, insulin, or a combination. Each patient received detailed complete ophthalmologic examination, including Snellen best-corrected visual acuity, applanation tonometry (Goldmann), OPA (baseline, 7 and 30 days after PRP), measurement with dynamic contour tonometry (DCT; Pascal, Ziemer Ophthalmic System AG, Port, Switzerland), slit-lamp biomicroscopy, indirect ophthalmoscopy, fundus photography (normal and red-free), and fluorescein angiography at the first visit (baseline evaluation).
Before the treatment, 7 days, and 1 month after the treatment, OPA was measured. All laser treatments and measurements were done during morning hours. Only one eye from each participant was included in the study, and the eye with worse visual acuity was chosen for laser treatment. The OPA of the untreated contralateral eye was used as control. During the study period, the other eye, which did not receive laser treatment, was carefully monitored (visual acuity checkup and dilated fundus examination were done weekly). None of the patients developed any complication that can arise from delayed laser treatment. After the study period was over, fellow eyes underwent PRP treatment.
The DCT measurements were taken after topical anesthesia (tetracaine 1.0%). During the measurement, subjects were asked to keep both eyes open, breathe quietly, and fixate into the distance behind the examiner. Since the quality of the DCT readings is classified from Q1 (optimum) to Q5 (unacceptable), we did not include Q3-Q5 measurements.
The PRP was performed with a 532-nm wavelength argon laser device (argon green laser, Integre S, 532 green retinal slit-lamp argon laser; Ellex, Adelaide, Australia), with H-R wide field fundus lens (Volk Optical, Mentor, OH, USA). The laser was used to create an effective retinal burn; approximately 1,500-2,000 burns were applied (200-500 mW, 0.2 seconds, spot size 200 μm), not exceeding the temporal retinal vessel arcades surrounding the macula. The fovea was approached for a maximum of 2 disk diameters in the temporal region and the optic disk for a maximum of a half disk diameter in the nasal region.
Methods of descriptive (arithmetical mean, SD) and analytical statistics (analysis of variance) were used to analyze the data and evaluate the significance of the difference. Value of p less than 0.05 was considered statistically significant. The data were evaluated for normality with the single-sample Kolmogorov-Smirnov test.
Results
The demographic features of all tested subjects are given in Table I. Systemic characteristics of all tested subjects are shown in Table II. The average diabetes mellitus duration was 16.7 ± 5.14 years.
Demographics
Systemic characteristics of tested subjects
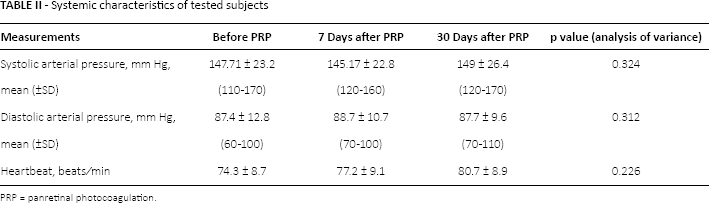
PRP = panretinal photocoagulation.
Compared with the untreated contralateral eyes, PRP led to a reduction of OPA. The OPA did not significantly differ in PRP eyes 7 days after the treatment (15% decrease, p = 0.231), but there was a significant difference in OPA measured 30 days after the treatment (40% decrease, p value <0.01, results shown in Table III).
Intergroup comparison of OPA between tested and control eyes
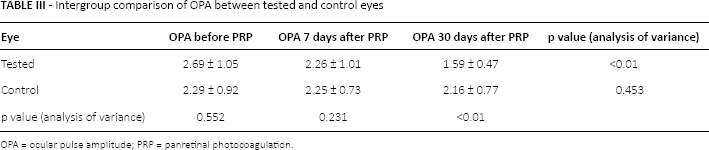
OPA = ocular pulse amplitude; PRP = panretinal photocoagulation.
In the control eyes group, there was no significant difference in OPA values (p = 0.453; Tab. III).
Discussion
Since the 1970s, PRP has remained the gold standard treatment for diabetic retinopathy and other causes of retinal ischemia (5).
Panretinal photocoagulation reduces or eliminates the production of the vasoproliferative stimulus by the peripheral retina, possibly by decreasing the total amount of retina surface available for angiogenic factor producing (6). The anatomical and functional changes that result from photocoagulation may improve the oxygen supply to the retina, possibly by the following mechanism: the decreased area of retinal tissue leads to improved oxygenation and a reduction in the levels of anti-vascular endothelial growth factor. Also, a reduction in levels of anti-vascular endothelial growth factor may be important in reducing the risk of new vessels forming (7, 8). The inner retinal PO2 (partial oxygen pressure) increases after photocoagulation (9) and in that way PRP relieves hypoxia in the inner retina, which leads to reduction in or stopping of diabetic retinopathy progression. Thermal changes cause denaturation of proteins in the tissue that is treated directly, but also in neighboring tissue.
One of the complications of PRP is transient IOP elevation (10). Many investigators have reported a transient IOP elevation during the first few hours after PRP; one reported a decrease within the first 6 months (11, 12), but other studies report reduction of choroidal blood flow and significant decrease in IOP, pulse amplitude, pulse volume, and pulsatile ocular blood flow (12–13–14). Transfer of thermal energy during argon laser PRP can cause an inflammatory cascade that can lead to ciliochoroidal effusions and detachments with anterior rotation of the ciliary body, forward shifting of the lens-iris diaphragm, and narrowing of the anterior chamber angle with the potential for angle-closure glaucoma (15). Therefore, IOP spikes during the acute post-PRP period should be treated with cycloplegics as well as topical and systemic antiglaucoma medications. This possible complication can be avoided by giving fewer than 1,000 laser burns in a single session, and using a power less than 1 watt, whenever possible. These steps were taken in our study, and none of the participants in our study experienced post-PRP IOP rise.
The OPA changes after PRP in normotensive eyes with proliferative diabetic retinopathy were the focus of our study. Ocular pulse amplitude represents the difference between the highest and lowest IOP values measured during single continuous measurement. Ocular pulse amplitude is regarded as an additional vascular parameter determined by many ocular and systemic factors: IOP value, axial length, sex, left ventricular ejection time, pulse, time of day, the nocturnal blood pressure response, pulse pressure, age, even the corneal thickness and refractive error. As OPA represents an indicator of choroidal circulation, it can give us indirect information on vascular status of optic disc in patients with glaucoma, but also on general blood flow of the eye.
In a study performed by Yulek et al (16), OPA levels increased in the early period after PRP, but the tested patients were not matched for systemic hypertension, and the antihypertensive treatment was not included in selecting process, so the results were not evaluated in light of systemic hemodynamics.
The results of our study are consistent with the results of a study done by Schmitt et al (17), but the results on our limited sample size show almost 15% OPA decrease 1 week after PRP (which was not statistically significant), and as much as 40% OPA reduction 30 days after PRP. Schmitt et al noted less OPA decrease, but with a different technology, since they used oculo-oscillo-dynamography for their recording. We compared the OPA in eyes treated with PRP versus the fellow eye of those patients, in the same stage of the disease, thus avoiding the systemic variables that can interfere with these measurements, since they are theoretically equal in the same patients.
Longer term follow-up of PRP patients would show further OPA changes and possibly indirectly confirm the thesis of choriocapillaries closure after PRP described in previous studies (18).
Footnotes
Financial support: No financial support was received for this submission.
Conflict of interest: None of the authors has conflict of interest with this submission.