
Abstract
Purpose
To report an unusual case of bilateral choroidal folds related to multiple myeloma.
Methods
In this case report, fundus photography, fundus fluorescein angiography, fundus autofluorescence, and B-ultrasonography were used to assess posterior segment changes.
Results
A 55-year-old woman with history of multiple myeloma was found to have abnormal fundi. Clinical examination and investigations confirmed chorioretinal folds, which was considered to be related to myeloma. Close monitoring ensued for 2 years with no significant changes. Subsequently, she was treated with stem cell transplant for myeloma, which resulted in remission of her disease. She was also noted to have marked improvement of chorioretinal folds within 1 year. Visual function remained normal throughout the follow-up period.
Conclusions
Multiple myeloma can infiltrate choroidal tissue, resulting in chorioretinal folds. Stem cell transplant was associated with significant reduction in paraprotein levels and choroidal folds.
Keywords
Introduction
Multiple myeloma is a form of bone marrow cancer characterized by proliferation of malignant plasma cells that secrete monoclonal paraproteins (1). Ocular manifestations of multiple myeloma are rare, affecting various ocular structures, some of which are potentially sight-threatening (1–2–3). We describe an unusual case of chorioretinal folds formation associated with multiple myeloma in the absence of orbital tumor, which improved following stem cell transplant.
Case Report
A 55-year-old woman presented to the eye clinic following an abnormal fundus appearance noted by her optometrist. She complained of intermittent flashing lights and floaters, without any pain or discomfort. She had an ocular history of mild hypermetropia and right esotropia (convergent squint) for which she underwent right squint surgery at age 21. Her medical history included multiple myeloma, with immunoglobulin G levels of 22 g/L at the time of presentation to the eye department (reference laboratory normal range 6-15 g/L), systemic hypertension, and carcinoma of the cervix, which was treated surgically.
On examination, the patient's corrected visual acuities were 6/6 in the right eye and 6/5 in the left eye. Amsler grid revealed no metamorphopsia and color vision was full. Examination of the anterior segments was unremarkable. Funduscopy showed evidence of bilateral extensive chorioretinal folds at the macula (Fig. 1, A and B). There were no signs of active chorioretinal effusion or macular edema, nor any evidence of proptosis, thyroid orbitopathy, orbital inflammatory disease, or orbital mass.
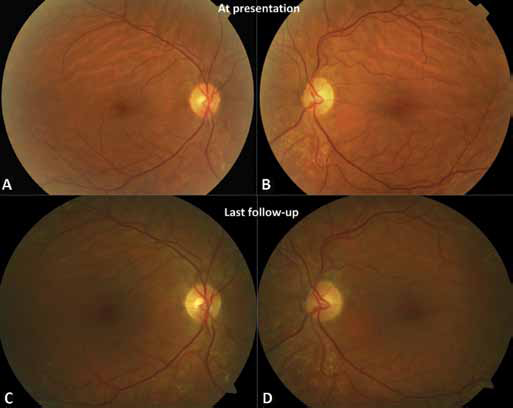
Color fundus photography. (
Fundus fluorescein angiography (FFA) (Fig. 2) at presentation clearly demonstrated bilateral chorioretinal folds without any angiographic leakage.
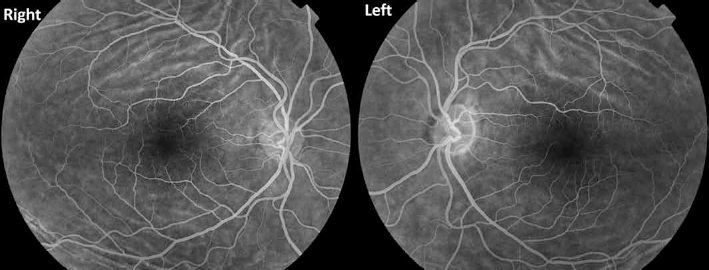
Fundus fluorescein angiography at presentation demonstrates characteristic appearance of the choroidal folds, with alternating hyperfluorescent and hypofluorescent bands (light and dark bands). The hyperfluorescent streaks correspond to the peaks of the chorioretinal folds, while the hypofluorescent bands correspond to the troughs.
A B-ultrasound scan showed thickening of the choroid and scleral wall but no evidence of choroidal effusion or other abnormalities, nor any sub-Tenon fluid around the disc to indicate posterior scleritis. Biometrical assessment (Zeiss [Oberkochen, Germany] IOLMaster) demonstrated relatively small eyes with an axial length of 20.90 mm in the right eye and 20.75 mm in the left eye.
Fundus autofluorescence showed characteristic alternating light and dark streaks (in an inverted pattern of the FFA findings) with peripapillary pigmentary mottling (Fig. 3).
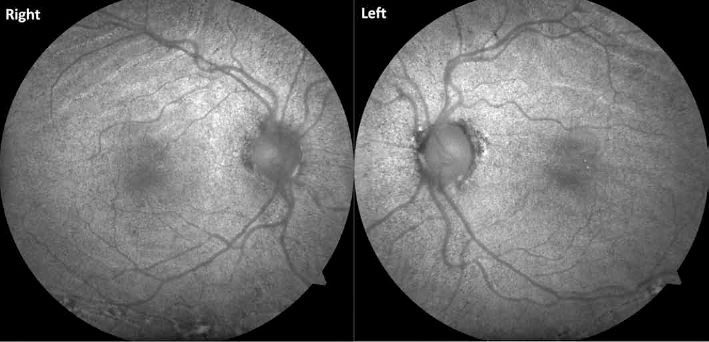
Fundus autofluorescence shows alternating light and dark bands (inverted pattern of the fundus fluorescein angiography findings) as well as pigmentary mottling in the posterior pole, with accentuation around the optic disc.
At that stage, our main differential diagnosis included choroidal infiltration by immunoglobulins, a resolved choroidal effusion secondary to myeloma-related oncotic changes, hypermetropia-related choroidal folds, or uveal effusion syndrome.
The patient was closely monitored by an ophthalmologist and hematologist. Two years following initial presentation, she received stem cell transplant from a sibling to treat multiple myeloma, which had an excellent outcome with very low paraprotein levels detected and satisfactory blood results.
Within a year after stem cell transplant, funduscopy showed marked reduction of chorioretinal folds in both eyes (Fig. 1, C and D), which has remained stable. Optical coherence tomography also found minimal residual folds. During this period, the patient's disease was well-controlled with very low paraprotein levels detected. The rest of her blood results were satisfactory.
Discussion
Chorioretinal folds describe the appearance of inner choroid, Bruch membrane, and retinal pigment epithelium in a ripple form. There are several explanations for the development of chorioretinal folds, including swelling of the choroid that forces the Bruch membrane into folds and the stress-strain relationship between the sclera and the choroid (4).
This is a relatively uncommon clinical sign that should prompt further careful assessment and investigation due to its association with many serious pathologies including systemic or orbital malignancy, infections, or immunologic disorder. The causes of chorioretinal folds include idiopathic (associated with acquired hyperopia), high hyperopia, thyroid eye disease, posterior scleritis, orbital tumors, choroidal tumors, uveal effusion syndrome, uveitis, papilledema, scleral buckling surgery, hypotony, and age-related macular degeneration (4). Patients with chorioretinal folds may be asymptomatic, or they may present with photopsia, metamorphopsia, or acquired hypermetropia.
Myeloma is known to cause ocular manifestations, which are predominantly related to the deposition of abnormal monoclonal gammaglobulins in various structures such as cornea (crystalline deposits), uveal tissue, or retina (2). Retinal findings encompass discrete retinal hemorrhages, flame-shaped hemorrhages, nerve fiber layer infarcts, and serous or exudative retinal detachments (2, 5). In addition, the hyperviscosity syndrome associated with myeloma may predispose to retinal vascular occlusion (2, 6).
Orbital involvement may manifest with progressive proptosis, restriction of ocular motility, ophthalmoplegia, and visual impairment caused by plasmacytomas arising in the soft tissues surrounding the orbit (2, 7). There have also been reports of chorioretinal folds due to mass effect of orbital plasmacytomas on the globe (2, 7).
The marked improvement of the chorioretinal folds following stem cell transplant was in favor of an immunoglobulin-related maculopathy (due to choroidal infiltration) as the main cause of chorioretinal folds, rather than hypermetropia alone. The pathogenesis is likely to be due to a diffuse infiltration of the uveal tissue by plasma cell aggregates combined with deposition of the monoclonal immunoglobulins within choroid, resulting in thickening and consequent folding of the choroid, a manifestation that subsequently attenuated following amelioration of the systemic disease. Uveal plasma cell aggregates have been documented in the histopathologic reports of intraocular plasmacytomas (1, 8). This case also represents the first report of choroidal folds related to multiple myeloma in the absence of orbital mass (plasmacytoma).
In summary, it is vital to elucidate the etiology of chorioretinal folds. Further investigation such as imaging should be considered to rule out orbital and systemic neoplastic or inflammatory process when the cause is unknown. Multiple myeloma may be associated with choroidal folds due either to mass effect or direct uveal tissue infiltration. Stem cell transplant led to significant reduction in paraprotein levels and choroidal folds.
Footnotes
Financial support: No financial support was received for this submission.
Conflict of interest: None of the authors has conflict of interest with this submission.