
Abstract
Purpose
To investigate the prevalence of eyelid laxity and quantify eyelid measurements in normal and keratoconic eyes and the correlations of these findings with ophthalmic parameters and disease severity in patients with keratoconus (KC).
Methods
In a prospective case-control study, prevalence of eyelid laxity and eyelid measurements were evaluated in 53 patients with KC and the same number of matched healthy controls. The eyelid measurements were compared between the groups, as well as mean keratometry (K), central and thinnest corneal thickness (CCT and TCT), astigmatism, manifest refraction spherical equivalent (MRSE), best spectacle-corrected visual acuity (BCVA), and severity of KC according to the Keratoconus Severity Score.
Results
Prevalence of eyelid laxity was 71.7% (38 patients) in patients with KC and 20.8% (11 patients) in normal participants (p<0.001, odds ratio 9.673 [95% confidence interval 3.959 to 23.631]). Comparison of the eyelid measurements in the patients with KC with and without eyelid laxity revealed significantly higher measurements of anterior eyelid distraction test, Hertel exophthalmometry measurements, lateral canthal angle to orbital rim and tendon movement, palpebral fissure width, retraction test (lower eyelid), and vertical lid pull (upper eyelid) in patients with KC with eyelid laxity (p<0.05). No significant difference was found regarding mean K, CCT, TCT, astigmatism, MRSE, or BCVA values of the patients with KC with and without eyelid laxity (p>0.05). Moreover, severity of KC was not associated with the presence of eyelid laxity or eyelid measurements (p>0.05).
Conclusions
Higher prevalence and greater eyelid laxity were found in patients with KC compared to healthy participants. However, eyelid laxity was not associated with severity of KC.
Introduction
In eyelid laxity, the upper and/or lower lid can be easily retracted. This entity is considered the less severe form of floppy eye syndrome (FES), a combination of easily everted floppy eyelids with papillary conjunctivitis in middle-aged men (1). This concept has expanded and researchers have described this syndrome in women, younger patients, and children with various degrees of conjunctivitis (none to severe) and in nonobese patients (1, 2). Numerous publications have focused on the associations of these entities with other ocular and systemic morbidities. Ophthalmic diseases like keratoconus (KC), pellucid marginal degeneration, and blepharochalasis, as well as ocular system abnormalities like tear film abnormalities and meibomian gland dysfunction, have been reported to be associated with FES (3–4–5).
Keratoconus is the most common corneal ectatic disorder, characterized by progressive corneal protrusion and thinning (6, 7). The prevalence of KC in patients with FES varies from very few cases to almost one-third of the study population (8, 9). However, few studies have evaluated the prevalence of FES and eyelid laxity in keratoconic patients. Pihlblad and Schaefer (10) found FES or sign of eyelid laxity in all of their patients with KC. There are several clues that link KC with FES. Repeated mechanical trauma like eye rubbing, although from different etiologies, has been shown to play a role in the pathogenesis of both diseases (3, 11, 12). Moreover, certain associated diseases, such as connective tissue abnormalities, specifically Ehlers-Danlos syndrome, and genetic disorders like Down syndrome, are common between the 2 entities (13). There are data that show increased prevalence of eyelid laxity in patients with KC even in the absence of the abovementioned common features, which points to a probable unknown underlying pathophysiologic process.
In our study, we aimed to compare the prevalence of eyelid laxity in patients with KC and normal participants. Moreover, we quantified the eyelid measurements and compared them between patients with KC and normal participants. Finally, the probable associations between these measurements and ophthalmic findings as well as disease severity in patients with KC were investigated.
Methods
Study Design
This prospective case-control study, conducted in the cornea clinic of the Aja University Hospital, Tehran, Iran, in 2015, was in accordance with the tenets of the Declaration of Helsinki and was approved by the hospital's review board and ethics committee. The purpose of the study was explained to all participants and those who agreed to participate signed informed consent.
Study population
In total, 53 patients with KC and 53 healthy participants who were between 18 and 60 years old were enrolled in this study. The KC and the control group were matched in terms of age, sex, body mass index (BMI), and obstructive sleep apnea due to known confounder effect of these parameters on eyelid laxity (4, 14, 15). The diagnosis of KC was based on slit-lamp biomicroscopic signs such as Vogt striae, Fleischer ring, corneal thinning, and scissoring reflex on retinoscopy, as well as topographic imaging and anterior or posterior corneal elevation findings by means of Pentacam (Oculus Optikgerate GmbH, Wetzlar, Germany) such as inferior-superior asymmetry, inferior localized steepening, and skewing of the steepest radial axes above and below the horizontal meridian. Those participants who were attended for refractive surgery who were not diagnosed with or suspicious for KC according to the slit-lamp examinations and topographic images were enrolled as the healthy control group. Participants with a history of ocular trauma; ocular or lid surgery; corneal cross-linking; any concurrent ophthalmic disorders such as glaucoma, dry eye, or corneal infections; connective tissue or autoimmune disorders; Down syndrome; atopy, thyroid disease, myasthenia gravis, or craniofacial abnormalities; contact lens wearers, those with history of extensive eye rubbing, and pregnant or nursing women were not enrolled in the study.
Diagnosis of eyelid laxity
All examinations were performed by one experienced ophthalmologist (A.J.). Patients with KC were divided into 2 groups of patients with KC with and without eyelid laxity. The presence of upper eyelid laxity was determined by the lid distraction test, in which measurements greater than 7 mm were considered positive. Lower eyelid laxity was determined by the snap-back test. Lower eyelid laxity was considered as positive when a 2- to 5-second delay for the lower lid to return to its state or persistent separation needing to a blink to return to the normal state was observed. In both upper and lower eyelid laxity, within normal limits were considered as negative.
Data collection
Only one eye of each participant that fulfilled the inclusion criteria was randomly selected and examined. Patients with KC and normal participants underwent eyelid laxity measurements, including vertical lid pull test on the upper and lower eyelids, anterior eyelid distraction test, lower eyelid retraction test, distraction test of the medial canthal tendon (MCT) and lateral canthal tendon of the lower eyelids, lateral canthal tendon angle to orbital rim, height of the upper eyelid crease, palpebral height and width, margin reflex distances (MRD1 and MRD2), levator function, tarsal height measured after eyelid eversion, and exophthalmos with a Hertel exophthalmometer (Oculus, Wetzlar, Germany). Moreover, for each patient with KC, mean keratometry (mean K), central and thinnest corneal thickness (CCT and TCT), and astigmatism based on Pentacam images, manifest refraction spherical equivalent (MRSE), and best spectacle-corrected visual acuity (BCVA) were recorded. Severity of KC was graded according to the Keratoconus Severity Score (KSS) proposed by McMahon et al (16, 17).
Statistical Analysis
Statistical analysis was performed using IBM SPSS statistics software (version 22, IBM, Armonk, NY). Data are presented as number (%) or mean ± SD. Since the data were not normality distributed (Kolmogorov-Smirnov test), the chi-square test and the Mann-Whitney U test or Kruskal-Wallis H test were used to analyze categorical and continuous variables, respectively. The Spearman correlation test was performed to evaluate the relationship of eyelid measurements with ophthalmic parameters. Power calculation analysis revealed that with a probability of type 1 error (α) of 0.05 and effect size (β) of 0.5, 53 patients have 80% power to detect the difference between both groups. A p value less than 0.05 was considered statistically significant.
Results
Demographics and primary characteristics of the study groups
Of the 106 total patients enrolled in the study, 53 had KC and 53 were normal. The analysis revealed that both groups were well-matched. The mean ± SD age of the KC and the normal group was 33.5 ± 5.8 and 34.0 ± 5.8 years, respectively (p = 0.644). There were 28 men (52.8%) and 25 women (47.2%) in the KC and normal groups (p = 1.000). The mean BMI of the KC and the control group was 27.4 ± 3.4 and 26.6 ± 3.3, respectively (p = 0.219). There were 15 (28.3%) patients with mild KC, 27 (50.9%) patients with moderate KC, and 11 (20.8%) patients with severe KC.
Prevalence of eyelid laxity
Prevalence of eyelid laxity was 71.7% in the patients with KC (38 patients) and 20.8% in the normal participants (11 patients). There was a statistically significant difference in the prevalence of eyelid laxity in the KC and the normal group (p<0.001) with odds ratio of 9.673 (95% confidence interval 3.959 to 23.631).
Comparison of the eyelid laxity measurement in patients with KC and normal participants
In the KC group, there were 38 patients (71.7%) with eyelid laxity and 15 patients (28.3%) without eyelid laxity. Comparison of the demographics and eyelid measurements in the patients with KC with and without eyelid laxity and the healthy control group is demonstrated in Table I. No significant differences were found between the study groups regarding age, sex, and BMI (p>0.05, all comparisons). Anterior eyelid distraction test and Hertel exophthalmometry measurement, lateral canthal angle to orbital rim and tendon movement, MCT lateral distraction test, palpebral fissure width, lower eyelid retraction test measurement, and upper eyelid vertical pull were significantly higher in the patients with KC with eyelid laxity than the patients with KC without eyelid laxity (p<0.05). Comparison of the eyelid measurements in the patients with KC with eyelid laxity and the normal group revealed statistically significant differences in all parameters except Hertel exophthalmometer value (Tab. I). On the other hand, comparison of the eyelid measurements in the patients with KC without eyelid laxity and the normal group revealed statistically significant differences only in the values of lateral canthal tendon movement and upper and lower eyelid vertical lid pull test (Tab. I).
Comparison of the demographics and eyelid measurements in patients with keratoconus with and without eyelid laxity and normal participants
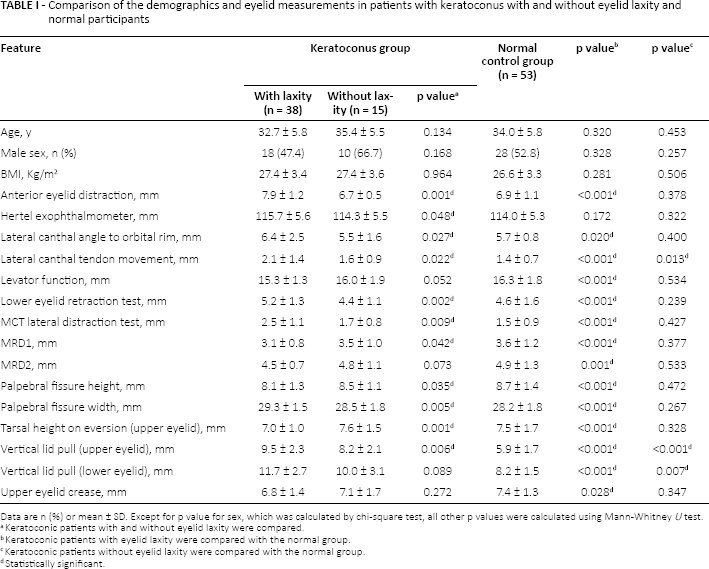
Data are n (%) or mean ± SD. Except for p value for sex, which was calculated by chi-square test, all other p values were calculated using Mann-Whitney U test.
Keratoconic patients with and without eyelid laxity were compared.
Keratoconic patients with eyelid laxity were compared with the normal group.
Keratoconic patients without eyelid laxity were compared with the normal group.
Statistically significant.
Comparison of the presence of eyelid laxity with ophthalmic parameters and KC severity
Comparison of the presence of eyelid laxity with ophthalmic parameters in the patients with KC is summarized in Table II. As shown, no significant differences were found regarding mean K, CCT, TCT, astigmatism, MRSE, or BCVA values of the patients with KC with and without eyelid laxity (p>0.05). Moreover, severity of KC according to the KSS classification was not significantly associated with the presence or absence of eyelid laxity (p = 0.152) (Tab. III).
Comparison of the presence or absence of eyelid laxity with ophthalmic parameters in patients with keratoconus
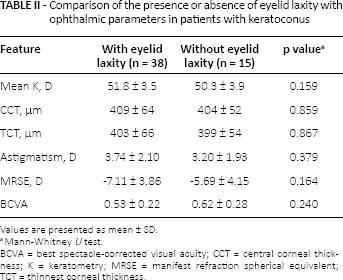
Values are presented as mean ± SD.
Mann-Whitney U test.
BCVA = best spectacle-corrected visual acuity; CCT = central corneal thickness; K = keratometry; MRSE = manifest refraction spherical equivalent; TCT = thinnest corneal thickness.
Distribution of keratoconus severity according to the presence of eyelid laxity
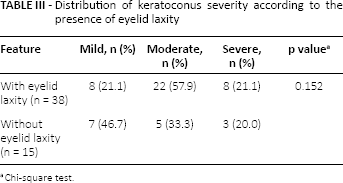
Chi-square test.
Correlation between eyelid measurements and ophthalmic parameters in patients with KC
The analysis of correlation between eyelid measurements and ophthalmic parameters (mean K, CCT, TCT, astigmatism, MRSE, and BCVA) in the patients with KC revealed statistically significant weak negative correlations between tarsal height measured after eyelid eversion with mean K (r = -0.287, p = 0.037), lower eyelid retraction test with CCT (r = -0.296, p = 0.032), and TCT (r = -0.285, p = 0.038), and Hertel exophthalmometry measurement with CCT (r = -0.329, p = 0.016) and TCT (r = -0.276, p = 0.045). Moreover, there were statistically significant weak correlations between palpebral height and MRSE (r = -0.284, p = 0.033), MRD1 with TCT (r = 0.281, p = 0.041), and MRSE (r = -0.282, p = 0.041).
Subgroup analysis in the patients with KC with eyelid laxity revealed statistically significant weak negative correlations between MCT lateral distraction test and CCT (r = -0.347, p = 0.033), lower eyelid retraction test with CCT (r = -0.341, p = 0.036) and TCT (r = -0.327, p = 0.045), and upper eyelid tarsal height on eversion with mean K (r = -0.367, p = 0.023). Moreover, there were statistically significant weak positive correlations between upper eyelid tarsal height on eversion with TCT (r = 0.351, p = 0.030), and BCVA (r = 0.371, p = 0.022). In the patients without eyelid laxity, there were statistically significant correlations between the measurements of the anterior eyelid distraction test and TCT (r = -0.583, p = 0.022), between the measurements of MCT lateral distraction test with the mean K (r = -0.624, p = 0.013), MRSE (r = 0.652, p = 0.008), and BCVA (r = 0.654, p = 0.008), and between palpebral fissure height with mean K (r = -0.605, p = 0.017), MRSE (r = 0.618, p = 0.014), and BCVA (r = 0.594, p = 0.019).
Comparison of eyelid measurements with KC severity
Comparison of eyelid measurements in all patients with disease severity according to the KSS classification revealed no significant association (p>0.05, all comparisons). Further detailed analysis and intergroup comparisons did not demonstrate any significant difference between subgroups of the KC severity (p>0.05, all comparisons). Moreover, the eyelid measurements were not significantly associated with KC severity, either in the patients with KC with eyelid laxity or in the patients with KC without eyelid laxity (p>0.05, all comparisons).
Discussion
Based on our findings, the prevalence of eyelid laxity was significantly higher in patients with KC compared to our normal controls. We observed that 71.1% of our patients with KC had eyelid laxity; this rate in our matched control groups was only a little more than 20%. Pihlblad and Schaefer (10) reported that although only one of their keratoconic patients (out of 15) fulfilled the criteria of FES, the other 14 patients all had eyelid laxity. Although there are several studies that emphasize the association between obesity and eyelid laxity (3, 4, 18), we could not find any significant difference in BMI of our patients with KC with and without eyelid laxity. Age and sex of the patients with and without eyelid laxity were not significantly different.
Among all evaluated eyelid measures, blepharoptosis and eyelash ptosis indices, Hertel exophthalmometry measurement, lateral canthal angle to orbital rim and tendon movement, MCT lateral distraction test, palpebral fissure width, lower eyelid retraction test measurement, and upper eyelid vertical pull measurement were significantly higher in the patients with KC with eyelid laxity. The lack of previous studies evaluating these measurements in patients with KC and the normal population has made the comparison of our findings with the literature difficult. Pihlblad and Schaefer (10) showed increased values in vertical pull test of the upper and lower eyelid, MCT laxity, palpebral width, exophthalmometry measures, and tarsus consistency in patients with KC with eyelid laxity vs the matched normal group.
Eyelid laxity in our patients with KC was not associated with keratometric or clinical findings of the disease. Whether eyelid laxity can aggravate the signs and symptoms of its associated morbidities and diseases is conflicting. Nevertheless, objective assessments revealed decreased tear break-up time, increased corneal staining, decreased Schirmer test score, increased meibomian gland dropout, increased eyelid vascularity, and more abnormal meibum quality in patients with eyelid laxity (19). In another study, scientists reported a 2.23-fold risk of severe ocular surface symptoms in their patients who had any grade of eye laxity (20). In our study, we could not find any significant association between the presence or absence of eye laxity as well as eyelid measurements and severity of KC based on the KSS classification.
In accordance with several other studies in the literature (3, 10), we could show an association between KC and eyelid laxity. Besides clinical and epidemiologic data, there are histopathologic investigations that can support this link between these entities. Several different hypotheses have been brought up by scientists to explain the underlying pathophysiology of eyelid laxity. One of the most convincing theories has accented the role of matrix metalloproteinase (MMP) enzymes in the pathogenesis of this disease. Based on this theory, a mechanical trauma triggers inflammation in the tissue of the eyelid, and the inflammatory cascades and the consequent cytokines and immunomodulators lead to induction of certain MMPs, specifically MMP-7 and MMP-9, which are responsible for degradation and ultrastructural changes of elastin (21). There is also histopathologic evidence for the role of MMPs in the pathogenesis of KC. In an interesting study, Balasubramanian and associates (22) showed an increased ratio of MMP/tissue inhibitor of metalloproteinase in keratoconic tissues compared with normal controls. There is also evidence that points to a pure increase of MMPs in KC (23). These investigations, although providing valuable data regarding the underlying pathogenesis of these diseases, do not seem to be enough for compiling the whole underlying scenario, and further studies, especially animal studies for simulating the hypothesized conditions and investigating the outcomes, are justified.
Study limitations
The major limitation of this study is the small number of patients with KC and healthy participants. Second, the current study was conducted at a university-based hospital setting; therefore, the examined participants may have more disease burden than patients in community-based practices, and patients with mild or undiagnosed disease may not be treated at a university-based hospital. Another limitation is that all the eyelid measurements were performed by only one observer, which could limit the intraobserver repeatability of the findings. Further studies with larger populations and multiple observers may help overcome this problem.
In conclusion, we found higher prevalence and greater eyelid laxity in patients with KC compared to healthy populations. However, eyelid laxity was not associated with severity of KC. It seems that there is a common related etiologic vulnerability in both disorders. These findings may help eye care practitioners to be aware of this association.
Footnotes
Financial support: No financial support was received for this submission.
Conflict of interest: None of the authors has conflict of interest with this submission.