
Abstract
Purpose
To evaluate corneal biomechanical properties and optic nerve head (ONH) changes following deep sclerectomy (DS) and the relation to each other.
Methods
Forty-nine eyes with primary open-angle glaucoma that underwent DS were studied. Corneal biomechanical properties were assessed using the Ocular Response Analyzer and the ONH was evaluated by Spectralis optical coherence tomography with enhanced depth imaging technology before surgery and 3 months postoperatively. Changes in corneal hysteresis (CH), corneal resistance factor (CRF), optic nerve cupping, prelaminar tissue thickness, and lamina cribrosa depth and thickness were registered. A correlation matrix and multiple linear regression models were used to determine predictors of ONH changes.
Results
At 3 months after surgery, mean corneal compensated intraocular pressure (IOPcc) significantly decreased by 27.9% (p<00.001) and mean Goldmann-correlated IOP (IOPg) decreased by 30.52% (p<00.001). Mean CH increased and CRF decreased by 18.4% and 10.1%, respectively (p<00.001). There was a significant reversal of ONH cupping mainly due to a prelaminar tissue thickening (p<00.001). Significant associations were found between ONH cupping reversal and prelaminar tissue thickening with preoperative IOPcc (p = 0.046), IOPg (p = 0.02), and CRF (p = 0.002) and with changes in IOP, CH, and CRF (p<00.001, p = 0.004, p = 0.018, respectively) after surgery.
Conclusions
Corneal hysteresis increased and CRF decreased significantly 3 months after DS. Corneal resistance factor was the single largest preoperative factor influencing cupping reversal changes. Despite the influence of preoperative variables, postoperative IOP reduction was the only independent factor influencing changes observed in the ONH after surgery.
Keywords
Introduction
The optic nerve head (ONH) and, more particularly, the lamina cribrosa (LC) are considered as the primary site of axon injury in glaucoma. The proposed mechanisms include stretching and shearing of the retinal ganglion cell axons, disruption of axoplasmic flow, and restriction in the blood supply (1–2–3). A wide range of structural modifications have been described in the peripapillary region as a response to intraocular pressure (IOP) changes concerning the LC, the prelaminar tissue (PT), and the anterior scleral canal (4–5–6–7–8). Variation in the material properties and morphology of these structures will influence their mechanical responses to pressure fluctuations (9).
Elevated IOP remains the most important known risk factor for glaucomatous optic neuropathy (10). Although some factors such as age, race, and central corneal thickness (CCT) are well-established risk factors for glaucomatous damage, new factors such as lower corneal hysteresis (CH) and corneal resistance factor (CRF) have been associated with the diagnosis (11, 12) and the progression of glaucoma (12, 13). The introduction of the ocular response analyzer (ORA) has allowed the measurement of the corneal biomechanical properties in vivo, providing indexes such as the CH and the CRF. Corneal hysteresis is the difference between the inward and outward motion applanation pressure and reflects corneal capability to absorb and remove energy. Corneal resistance factor seems to be an indicator of the total viscoelastic response representing the overall resistance of the cornea.
It has been postulated that elastic properties of the cornea might reflect the elasticity of other ocular structures such as the sclera and the LC. Since cornea and sclera are contiguous parts of the corneoscleral envelope formed from continuous extracellular matrix (14), deformability of the cornea and sclera are likely to be closely related. Thus, measures of CH and CRF could be indicative of the susceptibility of the ONH to IOP-induced biomechanical changes (15).
We hypothesize that corneal biomechanics properties could be related to ONH changes that occur after IOP reduction. To our knowledge, there are no previous reports investigating the relationship between the corneal biomechanical properties and ONH before and after glaucoma surgery. The purpose of this study was to assess the variation in corneal biomechanical properties measured by ORA and the variation in the ONH morphology (cupping depth, PT, and LC) measured by spectral-domain optical coherence tomography (SD-OCT) with enhanced depth imaging (EDI) technology before and 3 months after deep sclerectomy and to evaluate their relationship.
Methods
Participants
This prospective nonrandomized consecutive study comprised 49 eyes of 49 patients with primary open-angle glaucoma (POAG) selected for deep sclerectomy from February 2015 through January 2016. The study protocol was approved by the Ramón y Cajal Hospital Review Board. All research was performed in adherence to the principles of the Declaration of Helsinki and all patients signed written informed consent forms.
Inclusion criteria were a diagnosis of POAG with reproducible visual field defects and retinal nerve fiber layer (RNFL) defects, a healthy cornea, and a fundus examination without any signs of retinopathy or optic neuropathy different from glaucomatous optic neuropathy. Exclusion criteria were the presence of any ocular pathology different from optic nerve glaucomatous damage, previous ocular surgery other than cataract extraction, intraoperative perforation of the trabeculo-Descemet membrane requiring reconversion to trabeculectomy, a postoperative IOP ≤5 mm Hg, and the occurrence of any surgical or postsurgical complication. Image quality score ≥20 was mandatory.
Patient examinations
Preoperative CCT was measured by ultrasonic pachymetry (SP-2000, Tomey Corp., Cambridge, MA) and the axial length (AL) was obtained by IOLMaster (Carl Zeiss Meditec, Jena, Germany). Visual field (VF) was performed within 2 months before surgery, using a Humphrey perimeter (Humphrey Systems, Dublin, CA, USA) Swedish Interactive Testing Algorithm (SITA) 24–2 strategy. Mean deviation (MD) was the VF parameter evaluated in the current study. All participants underwent testing with the ORA and scanning with EDI SD-OCT before and 3 months after surgery.
The ORA (Reichert Ophthalmic Instrument, Buffalo, NY) was used to measure CH, CRF, Goldmann correlated IOP (IOPg), and corneal-compensated IOP (IOPcc). Three ORA readings were taken per eye at each visit and the mean of these readings was used in the analysis according to the manufacturer's instructions, which recommends that the quality of the waveform should be assessed by identifying 2 well-defined peaks that are reasonably symmetrical and higher than the superimposed pressure curve with repeatable characteristics for multiple measurements. While it has been suggested that applying a quality cutoff for the waveform score may be unnecessary (16), we excluded eyes with a very low best waveform score (<3.5) based on manufacturer advice and other normative data (17).
Image acquisition OCT protocol and measurements
The optic disc was evaluated using Spectralis OCT (Heidelberg Engineering GmbH, Heidelberg, Germany) and the EDI technique obtained through undilated pupils. The OCT device was set to image a 15 × 10 degree vertical rectangle centered on the optic disc. Thirteen cross-section scans were obtained, which were 120 µm apart. One vertical scan that was the closest to the ONH center and did not include any main vessels was selected from the preoperative images and the same scan was analyzed in postsurgical examination with the follow-up protocol allowing the evaluation of changes at the same location. The details of this measurement method have been described previously (4).
All the measurements were carried out by the same masked observer (L.D.-A.). The observer was masked both to the patient's characteristics and the time of the image (preoperative or postoperative). To evaluate intraobserver reproducibility, 15 randomly selected scans were remeasured by the same observer, and the intraclass correlation coefficient was calculated.
Surgical Technique
All surgical procedures were performed by one of the authors (G.R., F.J.M.-N., P.C.-L.) who used a standard surgical procedure as previously published (18).
Statistical analyses
SPSS software version 20.0 (SPSS, Inc., Chicago, IL, USA) was used for all analyses. The quantitative information was expressed as mean and standard deviation. One-sample Kolmogorov-Smirnov test was used to verify normal test distribution. The preoperative and postoperative changes in corneal and ONH parameters were compared using the paired t test analyses. Mann-Whitney U test was used to compare the heterogeneity between the sample of patients undergoing deep sclerectomy with the sample of patients undergoing deep sclerectomy combined with phacoemulsification. The preoperative and postoperative changes in corneal and ONH parameters in these 2 samples were compared applying the Wilcoxon signed-rank test. Pearson correlation analyses were performed to evaluate the association between corneal and ONH parameters and also to adjust the changes found in the cornea and in the ONH to other factors such as age, MD, CCT, and AL. A correlation matrix and then a stepwise regression procedure were performed to determine the subset of regression variables to be used in the final multiple regression model. A p value <00.05 was considered the level of significance.
Results
The study initially involved 57 eyes of 57 patients. Eight eyes were excluded due to low image quality (n = 5 eyes) and intraoperative perforation of the trabeculo-Descemet membrane (n = 3 eyes), leaving a final sample of 49 eyes of 49 patients.
The study population consisted of 25 men and 24 women with a mean age of 73.5 ± 8.2 years. Twenty-three eyes (46.9%) underwent isolated deep sclerectomy (DS) and 26 eyes (53.1%) DS combined with phacoemulsification (PDS) (Tab. I).
Patient demographics and clinical characteristics
DS = nonpenetrating deep sclerectomy; MD = mean deviation; PDS = nonpenetrating deep sclerectomy combined with phacoemulsification.
All patients were treated with 2 or more ocular antihypertensive drugs before surgery: 9 of them with 2 drugs (18.4%), 34 (69.4%) with 3 drugs, and 6 (12.2%) with 4 drugs.
Overall, at 3 months after surgery, there was a statistically significant decrease in the mean IOPcc (27.9%, p<00.001), IOPg (30.5%, p<00.001), and CRF (10.1%, p<00.0001). In contrast, we found a significant CH increase (18.4%, p<00.001) (Tab. II).
Comparison of IOPcc, IOPg, CH, and CRF values measured by ORA and ONH excavation, prelaminar tissue thickness, LC position, LC thickness, and BMO measured by EDI-OCT before and after surgery showing global results and subgroups according to the type of intervention (nonpenetrating deep sclerectomy alone or combined with phacoemulsification)
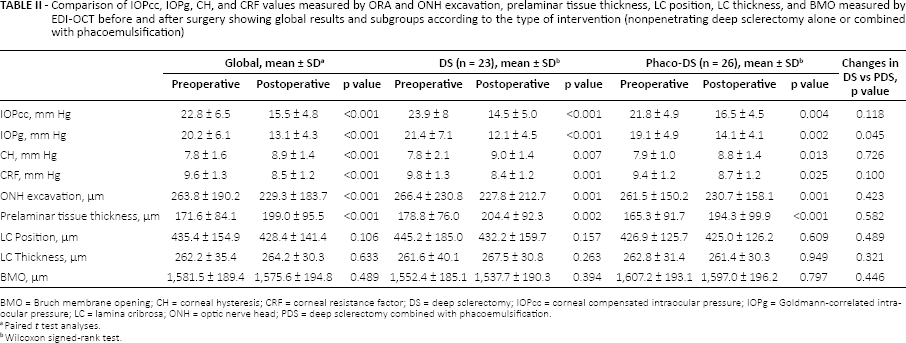
BMO = Bruch membrane opening; CH = corneal hysteresis; CRF = corneal resistance factor; DS = deep sclerectomy; IOPcc = corneal compensated intraocular pressure; IOPg = Goldmann-correlated intraocular pressure; LC = lamina cribrosa; ONH = optic nerve head; PDS = deep sclerectomy combined with phacoemulsification.
Paired t test analyses.
Wilcoxon signed-rank test.
Regarding ONH parameters, the mean cup depth showed a statistically significant decrease (p<00.001) while the PT significantly thickened (p<00.001). No significant changes were observed in the LC position, LC thickness, or Bruch membrane opening (BMO) diameter (p = 0.106, 0.633, 0.489) (Tab. II).
The postoperative changes observed in corneal biomechanical properties were higher in patients who underwent DS compared to PDS but differences were not significant. No significant changes were observed in ONH measurements between the groups.
Significant correlations between corneal biomechanical properties and ONH changes were observed. Preoperative IOPcc, IOPg, and CRF were positively correlated with cupping reversal (0.287, p = 0.046; 0.331, p = 0.02: 0.433, p = 0.002) and with PT thickening (0.283, p = 0.049; 0.324, p = 0.023; 0.420, p = 0.003). In addition, both IOPcc and IOPg reduction and CH and CRF changes were significantly associated with cupping reversal (0.509, p<00.001; 0.524, p<00.001; 0.402, p = 0.004; 0.336, p = 0.018, respectively) and with PT thickening (0.525, p<00.001; 0.525, p<00.001; 0.308, p = 0.031; 0.366, p = 0.010, respectively). The preoperative CCT and the LC thickening were also positively correlated after surgery (0.301, p = 0.047).
Mean preoperative AL was significantly correlated with preoperative LC thickness (-0.459, p = 0.012) and with the anterior displacement of the LC at 3 months after surgery (0.377, p = 0.044). LC movement after surgery was inversely correlated with age (-0.478, p = 0.001).
No significant correlation was found between MD in perimetry and corneal biomechanics or ONH parameters.
In the univariate analysis, higher preoperative IOPg and CRF and greater changes in IOPg, CH, and CRF after surgery were significantly associated with larger reduction of ONH cupping and greater increase in PT thickness. Stepwise regression analysis identified the changes in IOP as the only independent variable influencing changes in ONH cupping after surgery. Multivariate regression showed that changes in ONH cupping could be expressed using the following equation: changes in ONH cupping = 6.41 + 3.96 i IOPg change (R2 = 0.275, p<00.001).
Stepwise regression analysis of preoperative factors significantly correlated with the cupping reversal after surgery identified preoperative CRF as the single largest preoperative factor influencing ONH changes after surgery (R2 = 0.188, p = 0.002) (Fig. 1).
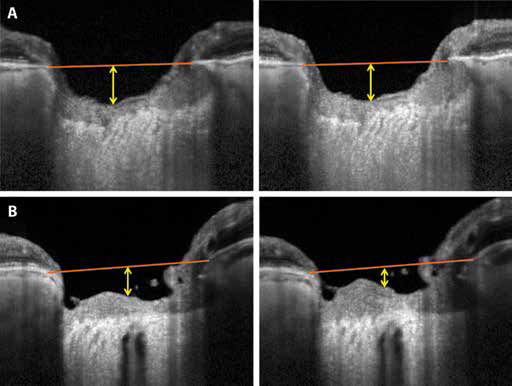
Representation of the postoperative optic nerve head (ONH) changes depending on the preoperative corneal resistance factor (CRF). Images were obtained preoperatively (A1, B1) and 3 months after deep sclerectomy (A2, B2). The orange line represents the reference line connecting Bruch membrane opening. The yellow line represents ONH cupping. (
Discussion
Corneal biomechanical property changes after glaucoma surgery have been described previously (19, 20). The CH increase and the CRF decrease observed in our study corroborate the results reported by Iordanidou et al (19) after DS. A decrease in both biomechanical corneal properties has been also reported in the early postoperative period after cataract surgery (20–21–22–23–24). We did not find any significant difference between DS and PDS 3 months after glaucoma surgery, suggesting that filtering surgery contributes to the changes to a greater extent than phacoemulsification incision. Furthermore, topical drugs, mainly prostaglandins (PG), may modify corneal biomechanical properties (25). In the current study, 38 (77.6%) patients were treated by topical prostaglandin analogues before surgery. Because they were used in conjunction with other topical drugs and several changes were made in the therapies prior to surgery, it is not possible to determine the true impact that each drug had on corneal properties. Nevertheless, as a CH increase has been reported after PG treatment, the expected effect after medication cessation would be a CH decrease. In contrast, in the current study, we found a significant CH increase after surgery, so our results are not directly related to PG therapy.
Similar to previous studies (4, 26), we found a significant optic nerve cupping reversal after glaucoma surgery mainly due to PT thickening with limited variation in LC position. The IOP reduction was determined as the main independent factor influencing changes in ONH after surgery.
It has been postulated that the elastic properties of the cornea may reflect the elasticity of other ocular structures such as the sclera or the LC (27, 28) and the corneal biomechanical properties might reflect the vulnerability of the ONH to glaucoma damage (29). Based on this hypothesis, some authors have reported a higher CH, CCT and CRF associated with an increased deformation of the optic nerve surface and a greater LC displacement during transient elevations of IOP (15, 30). A positive correlation between CH and anterior displacement of the LC has been described recently after medical IOP reduction (31). In our study, we demonstrated that CRF significantly correlates with PT thickening after surgical IOP reduction. Eyes having greater preoperative CRF were significantly associated with greater cupping reversal (p = 0.002) and PT thickening (p = 0.003) after DS. In fact, in the current study, CRF was identified as the most influential preoperative variable in ONH changes observed. We speculate that corneas with a higher CRF may reflect a greater resistance of the prelaminar tissue to chronic exposure to high IOP, allowing greater tissue decompression after IOP reduction. In contrast, patients with lower CRF might have larger destruction in the supporting tissue with regard to ocular hypertension, resulting in a negative impact in the cupping compliance and reversibility after IOP reduction. Different mechanisms have been proposed to explain the PT thickening after IOP reduction, including a shift of axonal fluid from the peripapillary RNFL downstream into the prelaminar neural tissues, a relocation of fluid that had been pushed downstream through the LC at higher IOP levels and subsequently redistributed into the prelaminar axons at lower IOP, and some increase in axoplasmic transport blockade within the LC by the relative constriction of the laminar pores after the taut lamina relaxes (32). Therefore, an alternative explanation might indicate that the PT thickening would be a reflection of the macrostructural and/or microstructural modifications that take place in the LC after IOP reduction, although our study has not been able to identify those changes. Conflicting results regarding LC displacement can be explained by the choroidal thickening after IOP reduction observed previously (33). The LC depth is commonly measured from the BMO level. If the choroid is thicker, this distance would be overestimated and therefore the postoperative choroidal thickening would increase the LC depth measured from the BMO plane. In contrast, the use of the anterior scleral opening as reference level to evaluate peripheral LC insertion using swept source OCT (SS-OCT) can avoid these measurement errors, although it is difficult as the laminar insertion points into the sclera are often obscured by shadows of the blood vessels (34). In addition, the IOP variation not only exerts a direct effect over the ONH in the sagittal plane inducing the anteroposterior displacement of the LC, but also exerts an indirect effect over the sclera inducing expansion or contraction of the scleral canal, which also affects the LC configuration (7). A higher CCT was also significantly associated with a greater LC thickening, supporting the relationship between the cornea and the LC in our study.
The mean preoperative AL was negatively correlated with the preoperative LC thickness (-0.459, p = 0.012) in accordance with previous studies (35). In addition, a larger anterior displacement of the LC was observed in patients with higher AL (0.377, p = 0.044), data not previously described, probably in connection with the greater ease of movement related to a thinner LC.
Our study has some limitations. First, postoperative follow-up includes only 1 postoperative evaluation at 3 months. Second, although the posterior surface of the LC was visible in most of the images, precise delineation of this border was more difficult compared to the anterior border, in accordance with previous articles (36, 37). To achieve more reliable delineations, only high-quality images were included and the posterior LC edge was determined not only considering the B-scan selected, but also examining the neighboring B-scans. The intraclass correlation coefficient for measurement of the ONH excavation and location of the anterior and posterior surfaces of the LC were 0.998, 0.995, and 0.878, respectively. Third, the laminar structures were assessed on one vertical scan selected at the center of the ONH, while the remaining peripheral scans were not evaluated, mainly because the prelaminar tissue and the LC were not clearly visible in the peripheral scans. Although information from periphery is not collected, the selected scan is representative of the structural changes. Given the posteriorly bowed nature of the LC, the reversal of the LC may occur largely in the central region, allowing us to observe the main changes that occur with IOP variations in a more evident way. Fourth, the integrity of the cornea and the sclera are compromised after DS. It has been postulated that elastic and resistance properties of the cornea might reflect the elasticity of other ocular structures such as the sclera; this might cause changes in the CH and in the CRF. Based on results from our study, it is not possible to distinguish which changes were related to the sclera changes and which were due to other factors. To clarify this point, a comparative study between deep sclerectomy and another noninvasive technique such as laser trabeculoplasty would be desirable. Fifth, patients included in our study were all previously treated with 2 or more topical antihypertensive medications, thereby it is impossible to determine the actual impact of each drug on corneal biomechanics. Sixth, we have not evaluated axial length along the follow-up. In contrast to trabeculectomy, there are scarce data about axial length changes after deep sclerectomy, but the reported change was small (-0.15 mm) (38). In the current study, no restrictions were made in relation to AL and MD, so we include a wide variability of AL and MD range. Lately, overall near 50% of eyes included had a severe glaucoma (MD over -12 dB) and 79.6% of patients were over 70 years old. Older patients and more advanced glaucoma are associated with specific corneal and ONH properties and promote less capability of reversible changes compared with mild and moderate glaucoma in younger patients; consequently the extrapolation of our data to these populations is not possible.
The strengths of this study include its prospective design and being the first study evaluating the relationship between the ONH and the corneal biomechanical properties after glaucoma surgery.
In conclusion, significant changes in both corneal and ONH biomechanical properties were observed after IOP reduction in DS. A significant correlation between ONH cupping reversal and preoperative CRF values was observed, the magnitude of IOP reduction being the most significant factor influencing ONH biomechanical changes.
Further studies with larger size and longer follow-up including a wide range of ages and glaucomatous damage are required.
Footnotes
Acknowledgments
Laura Díez-Álvarez received a grant from Jesús de Gangoiti Barrera Foundation to perform this study. The Foundation has no proprietary or commercial interest in any of the material discussed in this article.
Financial support: No financial support was received for this submission.
Conflict of interest: None of the authors has conflict of interest with this submission.