
Abstract
Purpose:
To determine the demographics, risk factors, clinical and microbiological characteristics, and treatment outcome of post-traumatic infective keratitis.
Methods:
Consecutive patients with post-traumatic infective keratitis presenting to the Ophthalmology Department of a tertiary referral hospital in Singapore between March 2012 and March 2016 were prospectively identified. A standardized data collection form was used to document patient demographics, microbiological diagnosis, antibiotic sensitivity, and pretreatment and posttreatment ocular characteristics. Any contact lens-induced keratitis was excluded from the study.
Results:
In total, 26 patients were included for analysis. The mean age was 40.0 years (SD ± 19.4) and 84.6% of the patients were male. The majority of the patients (69.2%, n = 18) had sustained work-related injury in their eyes. Gram-negative organisms were predominant isolates (75.0%, n = 12) in culture-positive corneal scrapings (n = 16). Pan-sensitive Pseudomonas aeruginosa was the commonest organism isolated among the culture-positive cases (56.2%, n = 9). Three patients (18.7%) had developed fungal keratitis and Acanthamoeba was isolated in 1 patient (6.2%) with polymicrobial keratitis. Infections resolved with medical treatment in 22 eyes (84.6%) and 4 eyes (15.3%) required therapeutic corneal transplantation.
Conclusions:
A shift of practice in post-traumatic infective keratitis should be considered in tropical countries to include Gram-negative cover. Work safety practices with vigilance in initiating treatment and education by front-line physicians such as ophthalmology and general practitioners should be reinforced.
Introduction
Infective keratitis remains one of the major causes of ocular morbidity worldwide and despite advances in treatment it poses significant challenges to ophthalmologists. It is a blinding condition characterized by an epithelial defect with inflammation of underlying stroma due to replicating organisms. The risk factors of infective keratitis include eyelid diseases, use of contact lens, poor ocular surface, and ocular trauma. Corneal involvement can vary in its extent (central cornea, peripheral cornea with or without involvement of the sclera) and depth depending on the type of organism and mechanism of infection (epithelium involvement only, stromal involvement such as ulceration and abscess formation, full-thickness involvement with subsequent cornea perforation) (1).
The visual prognosis depends on prompt diagnosis, microbiological confirmation, initiation of appropriate treatment, and location of residual cornea scar tissue. The literature on post-traumatic infective keratitis is limited to a handful of case reports and a prospective study conducted in Romania in 2005 by Stefan and Nenciu (2). However, there are several limitations to consider. First, the study only included bacterial keratitis. Stapleton and Carnt (3), Al-Dhaheri et al (4), and Upadhyay et al (5) highlighted Gram-positive bacteria as the predominant organism in non-contact lens-related disease (6). More recent case reports highlighted the increasing prevalence of fungus (7-9) as the causative organism. Second, the findings based on a single European country cannot be generalized to an Asian population with a different patient demographic and climate. Third, as the study was concluded in 2005, newer and more effective treatments may be applicable today.
In addition, infective keratitis is of socioeconomic relevance because visual rehabilitation can be protracted and patients tend to be in the working age group. In the United States (10), infective keratitis or contact lens disorders accounted for an estimated 930,000 outpatient visits and this translated into an estimated annual expenditure of $175 million USD on keratitis patients alone. Bharathi et al (11) reported corneal injury as a cause of infective keratitis in 70.88% (2,256 of 3,183) of patients in their study conducted in South India. The modifiable risk factors include awareness postinjury, the use of safety goggles, as well as the imprudent use of steroid eyedrops and the availability of newer generation of fortified antibiotic eyedrops postinjury. Nonmodifiable risk factors included male sex and mechanism of injury.
This study aims to reveal demographics, clinical characteristics, and the common organisms associated with post-traumatic infective keratitis in Singapore and to determine risk factors for poor visual prognosis.
Methods
The study included consecutive patients with post-traumatic infectious keratitis presenting to the Department of Ophthalmology, National University Hospital, Singapore, between March 2012 and March 2016. The study was conducted in accordance with the tenets of the Declaration of Helsinki and had ethics approval from the National Healthcare Group Domain Specific Review Board.
The diagnosis of infectious keratitis was made by an experienced corneal consultant (M.R.) at the National University Hospital, Singapore. We included all patients who were examined at the slit-lamp and diagnosed with infective keratitis as a result of ocular trauma. All the patients had a corneal scrape for microbiological isolation by trained ophthalmologists. Patients with an early corneal infection (ground glass reaction or increased anterior chamber activity) but too small for scraping (<1 mm) were excluded from the study. We further excluded cases of contact lens-related keratitis.
Data collection included patient demographics, occupation, precautionary steps taken, mechanism and duration of injury, examination findings on initial presentation and initial management, results of microbiological investigations such as Gram stain, fungus stain, and aerobic and anaerobic cultures, and other cultures as necessary. All suspected infectious corneal infiltrates were scraped for microbiological studies before initial treatment. Corneal smears were prepared for Gram and fungal stain with a spatula. Corneal samples were directly inoculated to blood and chocolate agar media for bacterial isolation and to Sabouraud agar media for fungal detection. Bacterial isolates were identified by Gram staining, colony characteristics, and motility testing. All bacterial isolates were tested for their antimicrobial susceptibility by standard disc diffusion method against different antibiotics. The results of the antibiotics sensitivity were recorded as resistant or sensitive. Bacterial culture was considered positive if 2 media had grown 5 or more colonies of a particular isolate or if growth in 1 media was associated with identification of the same organism in Gram stain. However, any fungal growth in 1 solid medium was considered positive. In cases of suspected Acanthamoeba keratitis, samples from corneal scrapes were subjected to direct microscopic examination, stains, and culture. Both Giemsa and calcofluor white stains were used to isolate the organism. Samples were also plated directly on non-nutrient agar media seeded with a lawn of Escherichia coli and incubated at 30°C. The samples were observed for up to 1 week to reliably prove a negative result.
Case notes were reviewed for subsequent follow-up visits to record final visual acuity, time taken to resolve the infection, and subsequent management if required. Data analysis was performed with Statistical Package for Social Sciences (SPSS, version 18.0).
Results
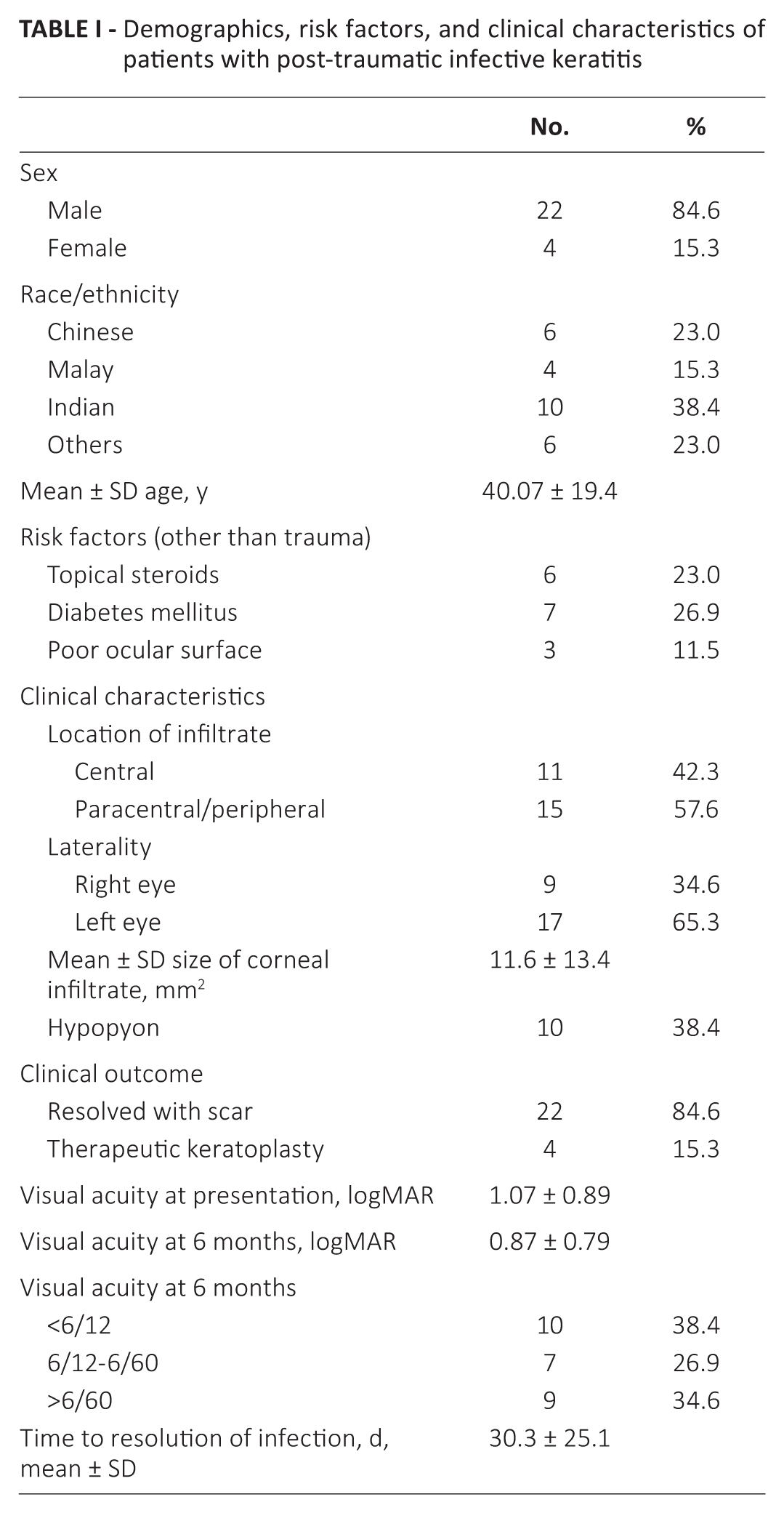
In total, 26 consecutive patients with post-traumatic infective keratitis were included in this study. The average age of the patients was 40.0 ± 19.4 years and the majority of the patients were male (84.6%, n = 22). Risk factors associated with impaired wound healing such as diabetes mellitus (26.9%, n = 7) and poor ocular surface (11.5%, n = 3) were sought in these patients but were found only to make up a small proportion of the total population. Six (23.0%) patients used topical steroids prior to presentation. The average size of the corneal infiltrate was 11.6 ± 13.4 mm2. More lesions were located paracentrally and peripherally (57.6%, n = 15) than in central cornea (42.3%, n = 11) and hypopyon was present in 10 eyes (38.4%) (Tab. I).
Demographics, risk factors, and clinical characteristics of patients with post-traumatic infective keratitis
Work-related injury was the predominant nature of injury in this study. As many as 18 eyes (69.2%) were involved in a work-related injury, of which 10 patients (55.5%) had sustained ocular injury from grinding work alone. Of particular note was the proportion of participants who had utilized work safety equipment in those with work-related injury. Fifty percent (n = 9) of patients with work-related injury did not use any safety goggles (Tab. II). Eight out of 18 (44.4%) participants had visited a general practitioner. Six of these participants were prescribed a combination of antibiotic and steroid eyedrops (neomycin sulfate 0.5%, dexamethasone sodium phosphate, 0.1%). Ten patients (55.5%) with work-related injury were also noted to have had previous corneal injury as evidenced by preexisting corneal scar in the same or fellow eye on presentation.
Nature of injury related to infective keratitis
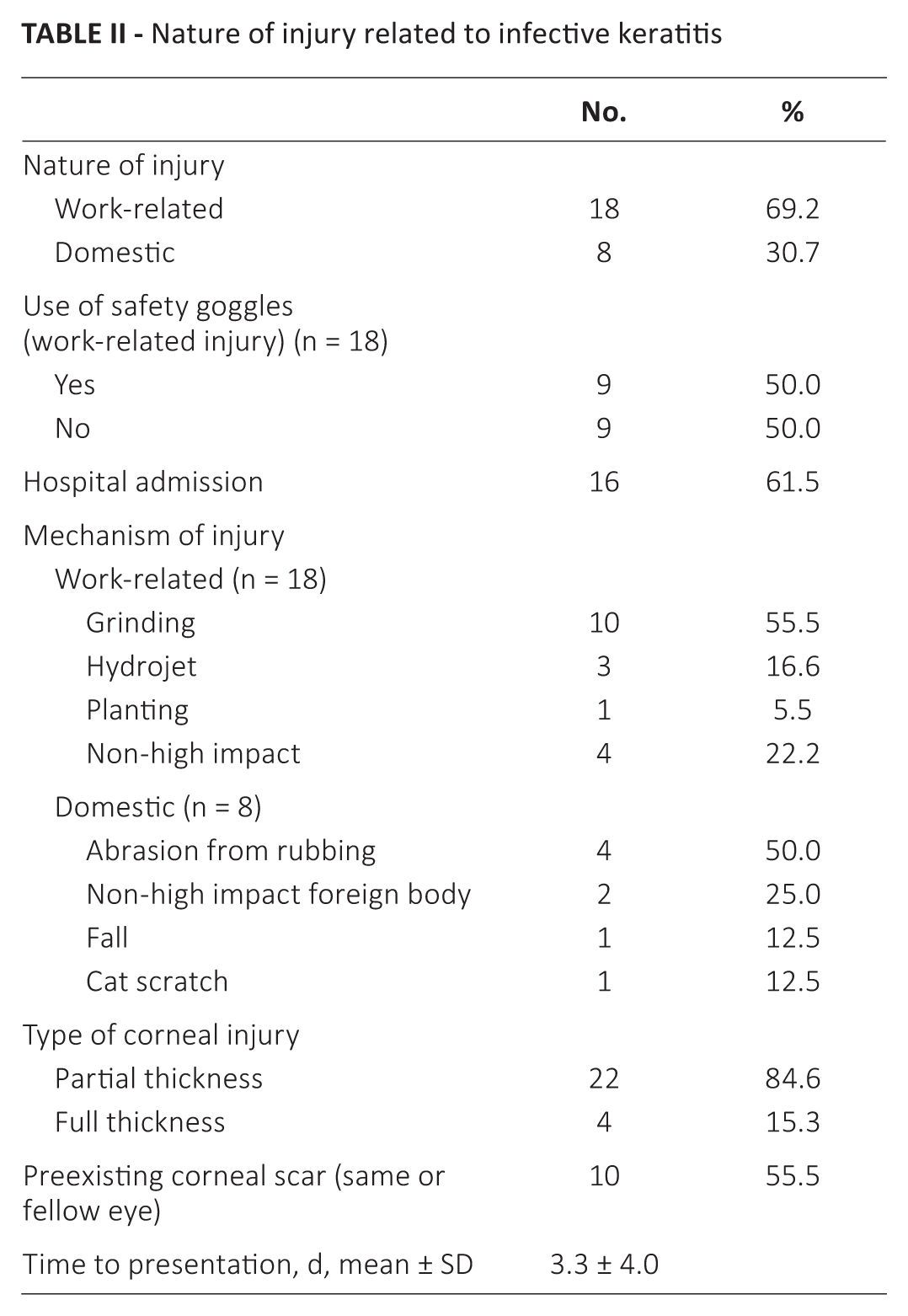
The average duration of symptom onset to hospital presentation was 3.3 (±4.0) days. The commonest presenting symptoms were eye redness with pain and visual loss in all participants. A total of 22 out of 26 (84.6%) participants had partial-thickness corneal injury, with 4 (15.3%) presenting with an open-globe injury (Tab. II).
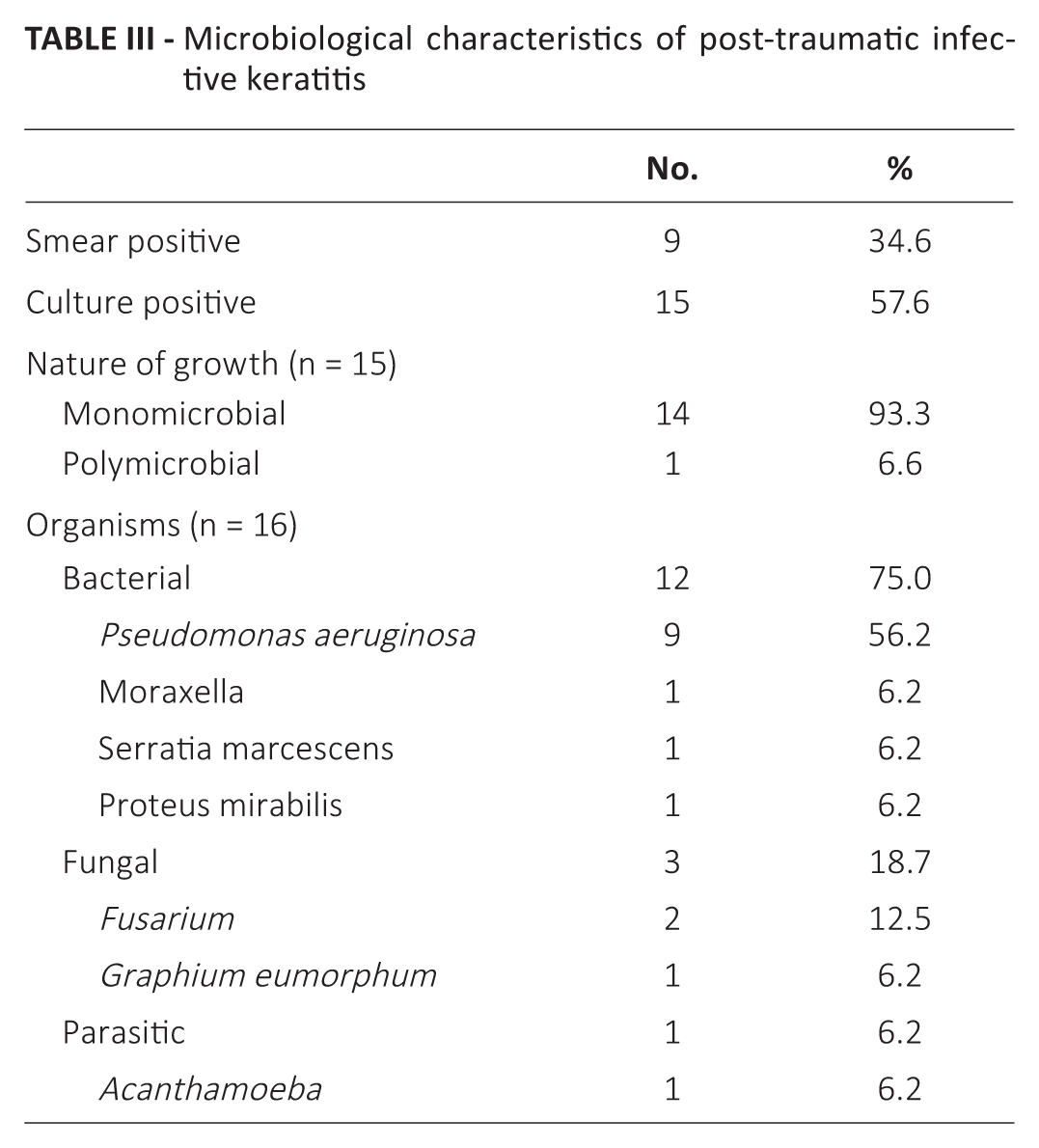
The rate of smear and culture positivity in this study was 34.6% (n = 9) and 57.6% (n = 15), respectively. Most culture-positive scrapes were found to be single organism related, of which Gram-negative organisms were predominant with no documented Gram-positive growth. One eye had developed polymicrobial infection. Pseudomonas aeruginosa was the commonest organism (n = 9), while Moraxella (n = 1), Serratia marcescens (n = 1), and Proteus mirabilis (n = 1) were the other Gram-negative organisms isolated in this study. Fungal keratitis was detected in 3 patients. Two patients had grown Fusarium while Graphium eumorphum was isolated in the third patient. Graphium eumorphum, an unusual filamentous fungus from the Scedosporium family, was isolated in Sabouraud agar medium, while the fungal stain was negative in this case Acanthamoeba and P aeruginosa were isolated in the patient with polymicrobial keratitis (Tab. III). All Gram-negative organisms were sensitive to ceftazidime, gentamicin, piperacillin, and ciprofloxacin.
Microbiological characteristics of post-traumatic infective keratitis
All participants were initially treated with broad-spectrum topical antibiotics comprising fortified cefazolin (50 mg/mL, 5%) and gentamicin (14 mg/mL, 1.4%) along with topical cycloplegics. The broad-spectrum antibiotics were eventually changed to monotherapy with topical ciprofloxacin (Ciloxan 0.3%, Alcon Laboratories UK) once adequate clinical response was obtained. Patients with open globe injury received additional systemic antibiotics. All the patients with fungal keratitis were treated with topical natamycin (5%), which is the first line of treatment for filamentous fungi. The patient with Acanthamoeba keratitis was treated with topical hexamidine (0.1%) and chlorhexidine (0.02%) along with cycloplegics. Infections resolved with corneal scar after medical treatment in 22 eyes (84.6%) (Tab. I).
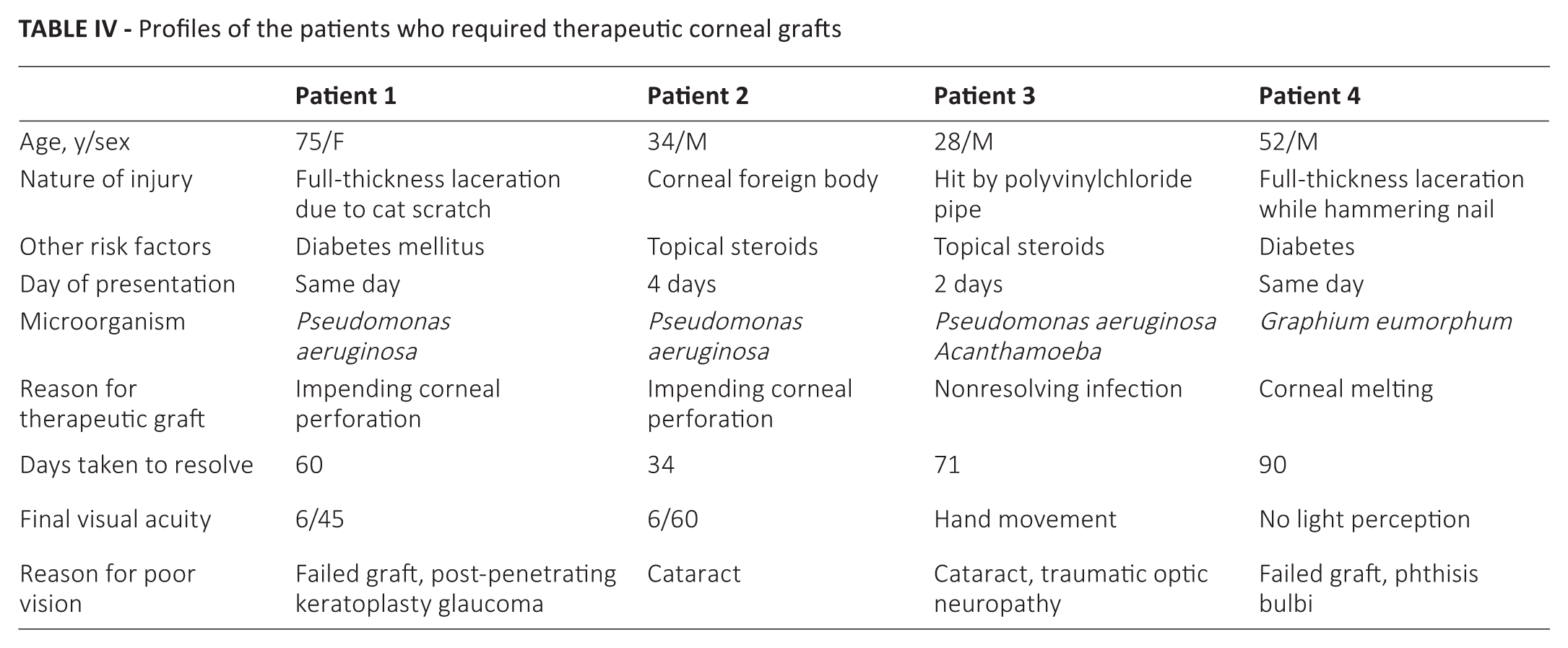
Four patients (15.3%) required therapeutic corneal transplantation due to impending corneal perforation (n = 2), corneal melting (n = 1), or nonresolving corneal infection (n = 1). Two of these patients had sustained full-thickness corneal laceration and incidentally both of them were also diabetic. The other 2 patients were relatively young and one of them used topical steroids following corneal foreign body removal. The fourth patient was hit by a polyvinylchloride pipe and developed polymicrobial infection with Acanthamoeba and P aeruginosa (Tab. IV). At 6 months posttreatment, 38.4% (n = 10) of patients had visual acuity better than 6/12, while 34.6% (n = 9) of eyes had poor visual outcome (>6/60) (Tab. I).
Profiles of the patients who required therapeutic corneal grafts
Discussion
The high proportion of individuals presenting to the general practitioner postinjury highlights the role of the primary care physician in the management of traumatic infective keratitis. However, it is disconcerting to note a large proportion of these patients having been prescribed steroid-antibiotics combination eyedrops, revealing the knowledge gap between the front-line physicians and resulting in a delay and complicating appropriate clinical management.
Although microbiological investigations have been shown to have only a moderate sensitivity of 50% in infective keratitis, results in this study showed culture positivity of 57.6%, which may account for the severity in these patients (1). This makes clinical diagnosis of infective keratitis imperative for the commencement of empirical antimicrobial treatment.
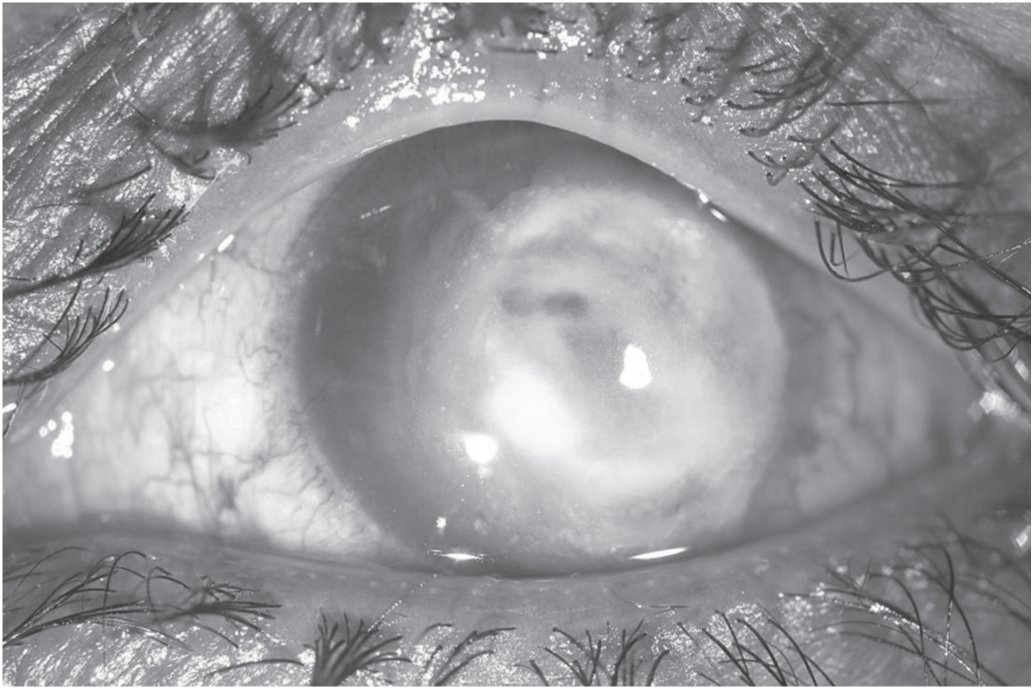
Of particular interest is the prevalence of Gram-negative organisms isolated in culture-positive cases, where Gram-positive organisms were previously thought to be the commonest causative organism (2, 4). This is in contrast to findings previously reported by Hagan et al (12) and Stefan and Nenciu (2) in more temperate climates and another study in tropical Malaysia. However, these were performed on all types of microbial keratitis regardless of etiology (13-16). In our study, no Gram-positive organisms were isolated in culture-positive eyes. Pseudomonas aeruginosa was the commonest Gram-negative organism isolated (Figs. 1 and 2).
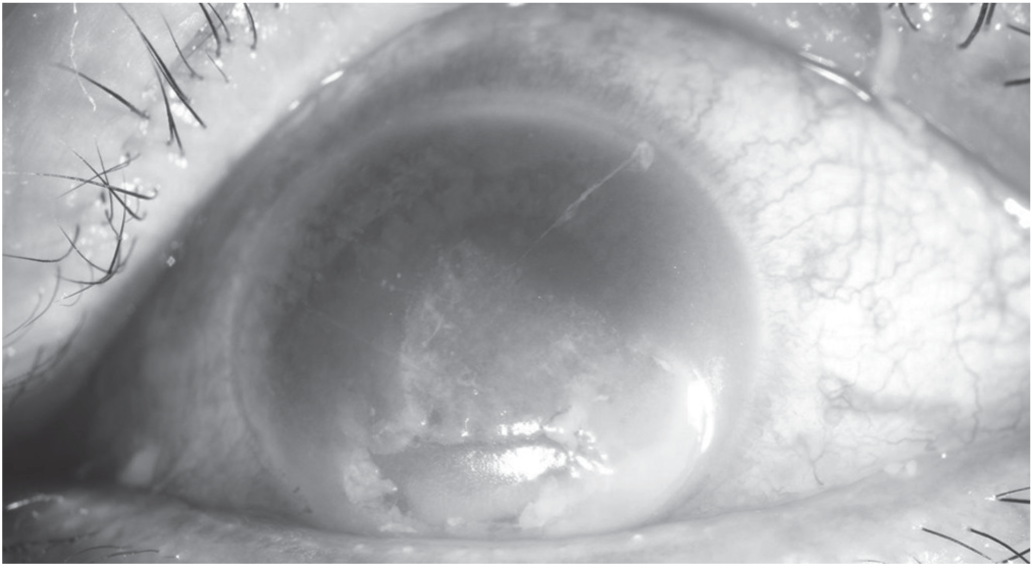
Pseudomonas keratitis following a corneal abrasion.
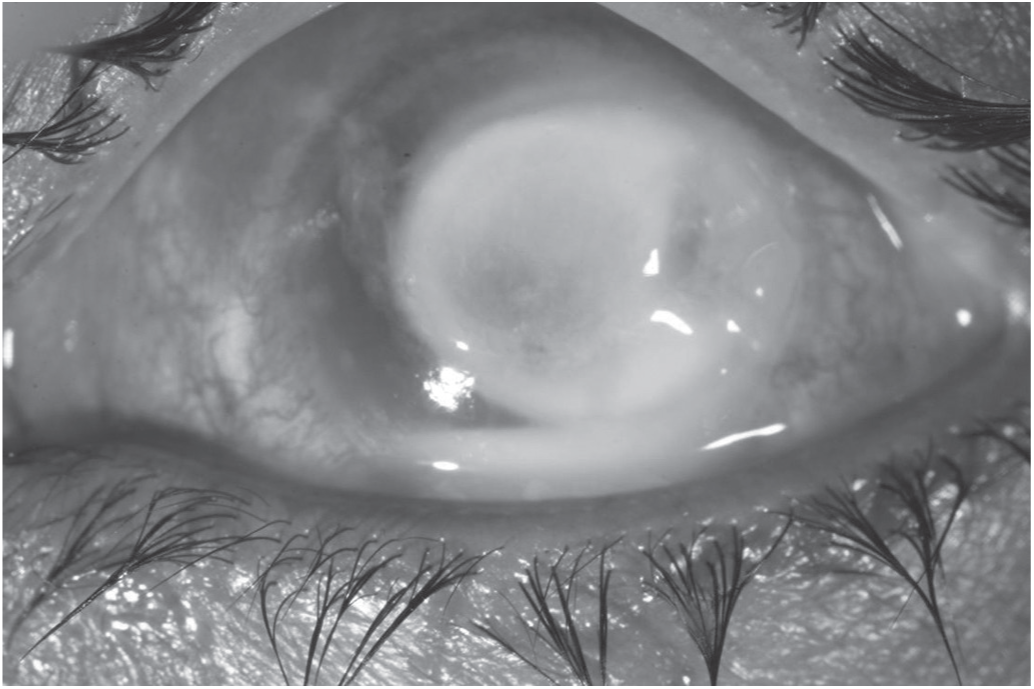
Pseudomonas keratitis with impending corneal perforation that required therapeutic corneal transplantation.
The prevalence of Gram-negative organisms in culture-positive post-traumatic infective keratitis should provide a paradigm shift of practice of treatment towards a choice of antibiotic that will be able to provide adequate bacterial coverage especially in tropical climates. A high index of suspicion for atypical growth of organisms such as fungal species in those with poorly healing infective keratitis should be considered.
In a case series investigating endophthalmitis associated with microbial keratitis by Scott et al (6), 13 (92.9%) of 14 patients with endophthalmitis had documented keratitis before the diagnosis of endophthalmitis was made. In this study, 7 of 14 (50%) eyes had Gram-negative organisms, followed by Staphylococcus aureus, streptococcal species, and fungi. This suggested urgency in prompt institution of appropriate treatment in view of the tendency of Gram-negative organisms to cause devastating infections. In our series, 2 patients with Pseudomonas keratitis needed urgent therapeutic keratoplasty due to impending corneal perforation (Fig. 2). Although the organism was pan-sensitive, these patients had presented relatively late to our clinic. This reconfirms the urgency of starting appropriate antibiotics.
In addition, Fusarium spp. was isolated in 2 eyes, of which one was in a previously well patient who had sustained a low-impact foreign body injury, which had then dislodged while the patient was walking, and the second a corneal abrasion after rubbing the eye on the background of poor health and immunity with poorly controlled diabetes mellitus, supporting our hypothesis that fungal-related keratitis occurs in tropical and humid climates and should also incite a high index of suspicion in those with poorly healing infections (Fig. 3). The third patient with fungal keratitis, who also has diabetes, had sustained a full-thickness corneal laceration while hammering a nail. He developed an unusual fungal keratitis with G eumorphum following repair of corneal laceration. This is an extremely rare form of keratitis and only one case has been reported previously in the literature (17). This patient eventually needed therapeutic corneal transplantation with poor visual outcome because of nonresolving infection (Fig. 4). Appropriate institution of treatment with good visual outcomes can still occur, with the former 2 patients retaining a subjective vision of 6/9 at 6 months posttreatment.
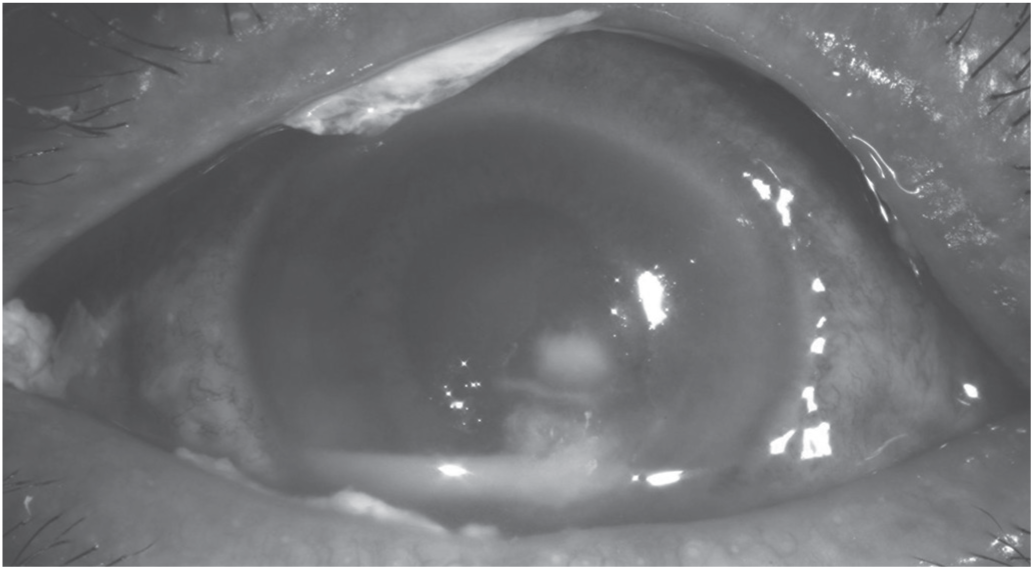
Fungal keratitis (Fusarium) following corneal abrasion.
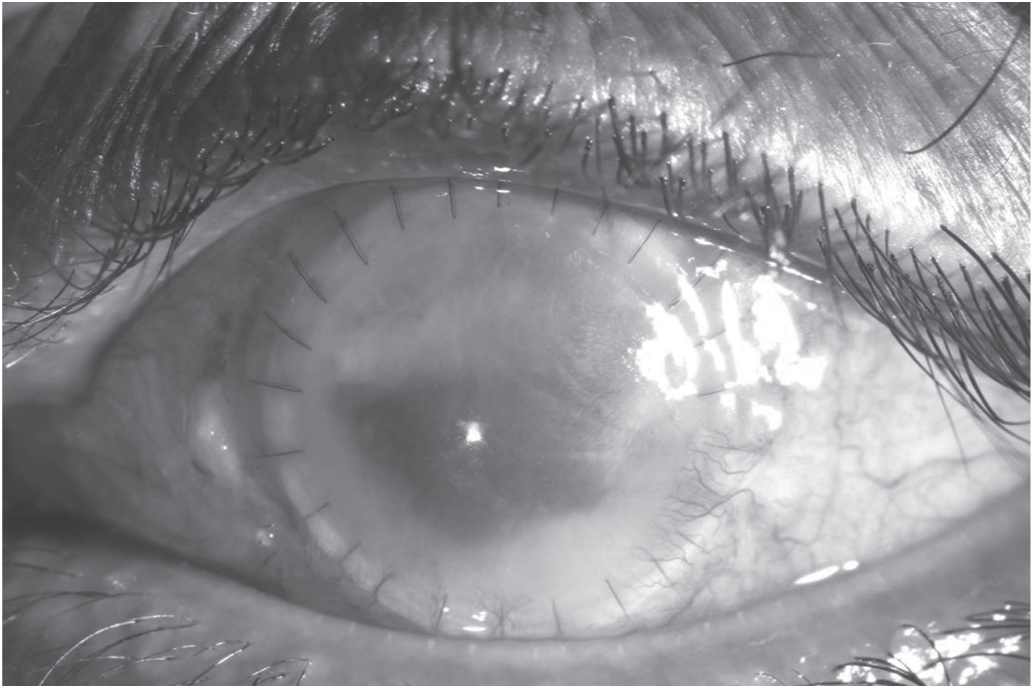
Therapeutic keratoplasty in a patient with nonresolving Graphium eumorphum infection following repaired corneal laceration.
It is alarming to note that both Pseudomonas and Acanthamoeba were also isolated in a patient who had been prescribed a combination antibiotic-steroid eyedrop following an eye injury (Fig. 5). It is vital to transfer relevant knowledge from the ophthalmologist to the general practitioner with awareness and appropriate restraint in prescribing steroid eyedrops after a traumatic eye injury.
Polymicrobial infection with Acanthamoeba and Pseudomonas aeruginosa after use of topical steroid following an injury.
It is a concern that despite prompt presentation to the ophthalmology service after eye injury, there is significant ocular morbidity, with a majority of these participants requiring intensive treatment with hospital admission and poor vision outcomes (34.6%) at 6 months. In addition, a large proportion of those with work-related injuries had poor outcomes, which suggests the importance of safety precautions in the workplace with appropriate protective eyewear as well as education on early detection. Only 50% of patients with work-related injury had used safety goggles in this study. Safety goggles are available in various designs and are usually made of strong polycarbonates. While most protective eyewear is generic, protective eyewear can be custom-designed with corrected refractive powers incorporated. Generally these goggles have a fastener that extends around the head that facilitates stronger attachment with the skin around the eye. Some sophisticated designs have a ventilation system to prevent fogging while in use. If used properly, no particles or chemicals should reach the eye. Our study showed that eye injuries are not uncommon even in those who wear safety goggles. It has been hypothesized that incorrect or inadequate eyewear is a major contributing factor. The majority of incidents occur when foreign bodies or chemicals seep through the sides of the eyewear. These workers may have used protective goggles that did not cover the eye completely or goggles that had cracks or other unsafe characteristics.
Inadequate work safety practices and vigilance postinjury were the major issues among participants, although an awareness to seek prompt medical advice was noted. In addition, a high proportion of individuals with industrial-related injuries and poor visual outcomes make appropriate education and awareness urgent. The primary care physician has an equally important role to play as the attending ophthalmologist in ensuring that appropriate preventive and treatment practices are performed and this study aims to prompt additional vigilance and conscientious care in the prevention of significant visual morbidity.
Our study showed that post-traumatic infective keratitis was associated with a wide range of organisms, including atypical ones. The visual prognosis was relatively poor and risk factors include the type of organism, the severity of the initial injury, and the use of antibiotic-steroid eyedrops.
Footnotes
Disclosures
Financial support: No financial support was received for this submission.
Conflict of interest: None of the authors has conflict of interest with this submission.