
Abstract
Purpose:
To compare surgical outcomes according to the distance between the preplaced suture and the muscle insertion in lateral rectus (LR) recession for exotropia.
Methods:
We retrospectively reviewed 64 patients who had undergone unilateral LR recession by one right-handed surgeon and divided the patients into 2 groups: right LR recession (R group, 26 patients) and left LR recession (L group, 38 patients). In the R group, the preplaced suture was behind the hook, far from the insertion; in the L group, the suture was in front of the hook, near the insertion. The main outcome measures were postoperative alignment and surgical success rate and the secondary outcome measure was effect/dose ratio. Surgical success was defined as an alignment between 10 prism diopters (PD) of exodeviation and 5 PD of esodeviation both at distance and at near. The effect/dose ratio was defined as the corrected angle of deviation at postoperative 6 months divided by the amount of LR recession.
Results:
The mean angle of deviation at distance showed a significant difference between the groups at postoperative 3 months (p = 0.022), but not at final follow-up (p = 0.163). There was no difference between the groups in the mean angle of deviation at near postoperatively. Surgical success was achieved in 73.1% of the R group and 71.1% of the L group at final follow-up, which was not significant (p = 0.860).
Conclusions:
The distance between the preplaced suture and the muscle insertion in LR recession did not affect the surgical success rate or the postoperative alignment at final follow-up.
Introduction
Recession of extraocular muscles is a method by which the muscle insertion is moved to a new location closer to the muscle’s origin. The surgery creates muscle slack and, thereby, effectively reduces muscle strength according to the Starling length-tension curve (1). Lateral rectus (LR) muscle recession induces correction of exotropia, whereas medial rectus muscle recession corrects esotropia (1, 2).
In conventional recession surgery of rectus muscles, the surgeon places a continuous double-armed suture through the rectus muscle after a conjunctival incision is created and the rectus muscle is hooked and cleared of anterior Tenon capsule. When this locking knot is created, the hook is placed behind the muscle, pulling the muscle for optimal exposure.
Theoretically, the surgical outcome can be influenced by the distance between the preplaced suture and the muscle insertion site. If the suture is located far from the insertion, it will reduce the extent of the planned recession, thus possibly diminishing the intended recession effect.
In this study, we compared surgical outcomes according to the distance between the preplaced suture and the muscle insertion site. For this purpose, we retrospectively compared right and left eyes for surgical success and postoperative alignment after unilateral LR recession for exotropia.
Methods
Design and patients
The medical records of 64 patients who had undergone unilateral LR recession between February 2008 and December 2013 for exotropia of 25 prism diopters (PD) or less were reviewed in this retrospective study. The minimum required follow-up period was 6 months postoperatively. Patients were excluded if they had a history of strabismus surgery, trauma, paralytic or restrictive exotropia, sensory exotropia, other ocular diseases, or systemic abnormalities. Informed consent was obtained from the patients (or from the guardians of the pediatric patients) according to a protocol approved by the institutional review board of Hallym University Medical Center.
Preoperative examinations
We reviewed the patients’ pertinent preoperative characteristics, which included onset age, age at surgery, Snellen best-corrected visual acuity (BCVA), refractive error, amblyopia, associated strabismus before surgery as vertical deviation, inferior oblique overaction, dissociated vertical deviation, and lateral incomitance. Amblyopia was defined as a difference of 2 lines or more between the 2 eyes’ BCVA on Snellen charts. Lateral incomitance was defined as a change of 10 PD or more between the exodeviation in the lateral gaze and the primary position.
Each patient was asked detailed questions about his or her disease history, as information on their onset age or any previous strabismus surgery. In order to measure the preoperative and postoperative deviation at both distance (6 m) and near (33 cm), alternating-cover testing in the primary position was performed to determine the magnitude of the vertical and horizontal angles of deviation. For a few younger or uncooperative patients, a modified Krimsky method was employed. Sensory status was evaluated by Titmus Stereotest (Stereo Optical Co.) and Worth 4-Dot test at distance in cooperative patients. Good stereopsis was defined as 100 seconds of arc or better on the Titmus Stereotest.
Grouping and strabismus surgery
All of the surgeries were performed under general anesthesia by one right-handed surgeon (D.G.C.) at Kangnam Sacred Heart Hospital. Patients without a dominant eye underwent the surgery on unilateral eye without laterality preference. Those with a dominant eye underwent the procedure on the nondominant eye.
The surgeon sat at the superior side of the patient’s head, and the assistant was positioned at the surgeon’s right. With the patient under general anesthesia, fixation sutures, through the conjunctiva and episclera close to the limbus, at the 12 and 6 o’clock positions, were performed. After the limbal conjunctival incision, the Tenon capsule was dissected, and the LR muscle was exposed and dissected. The Jameson muscle hook (11 mm hook, 1.8 mm tip; Integra Jarit Life Sciences Corp.) was inserted behind the muscle and pulled the muscle laterally for optimal exposure. The surgeon confirmed the engagement of the whole muscle by passing a second hook below the muscle repeatedly. A double-armed 6-0 coated Vicryl suture with spatula needle (Ethicon Corp.) was used for the preplaced suture. For securing the muscle, we sutured it with 3-point fixation. A 3-mm central security knot full-thickness in the center of the muscle was placed and tied in a square knot. Then two 3-mm full-thickness locking bites were placed at each edge of the muscle.
In the right LR muscle recession (R group), it was easier for the right-handed surgeon to locate the suture behind the hook (far from the insertion) than in front of the hook (near to the insertion) (Figs. 1 [top] and 2 [top]). On the contrary, in the L group, the suture was located in front of the hook (near to the insertion) (Figs. 1 [bottom] and 2 [bottom]). As a result, in the R group relative to the L group, the preplaced suture was positioned far from its insertion, approximately 1.0 mm by caliper measurement.
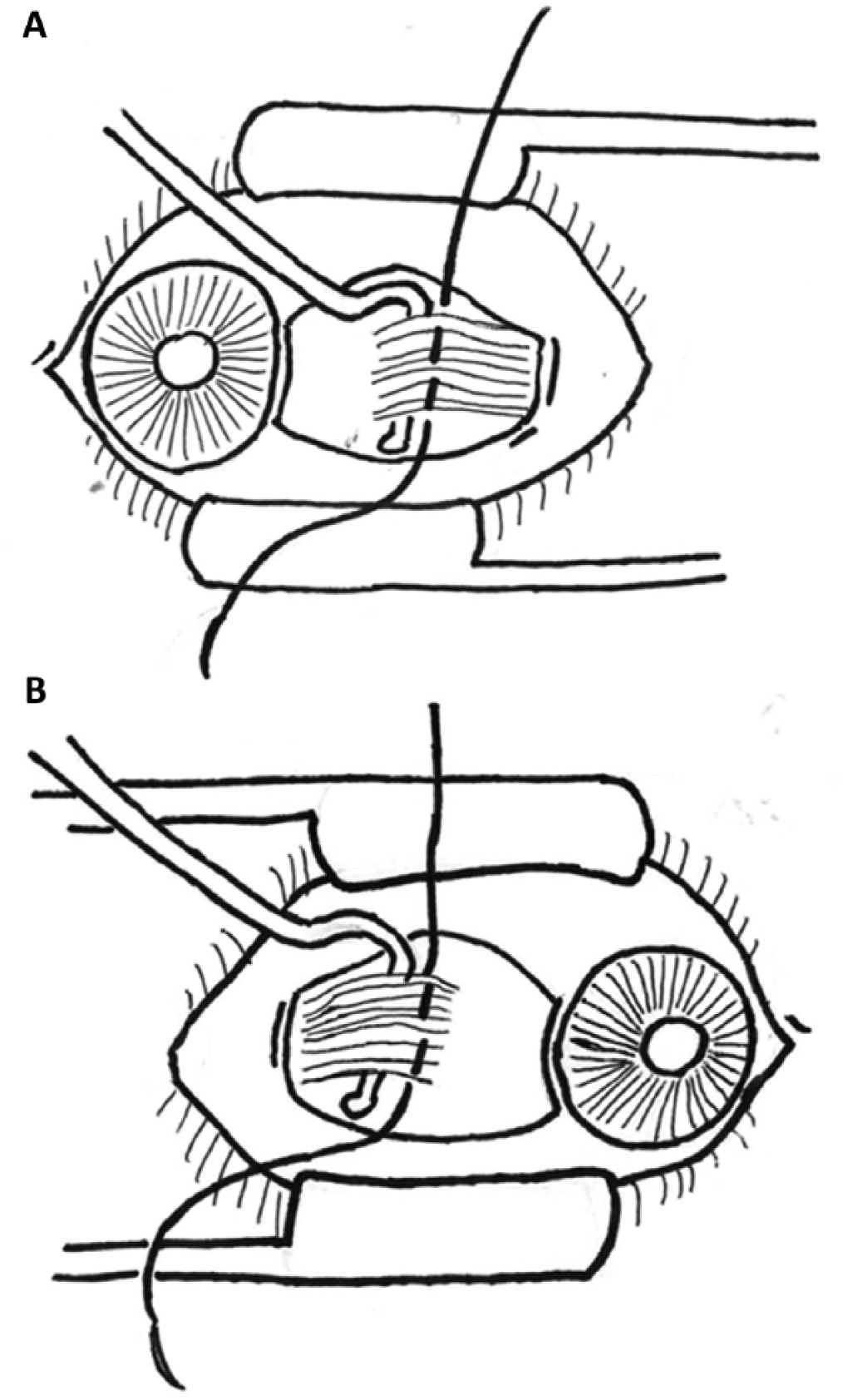
Schematic drawings of the preplaced suture through rectus muscle. (
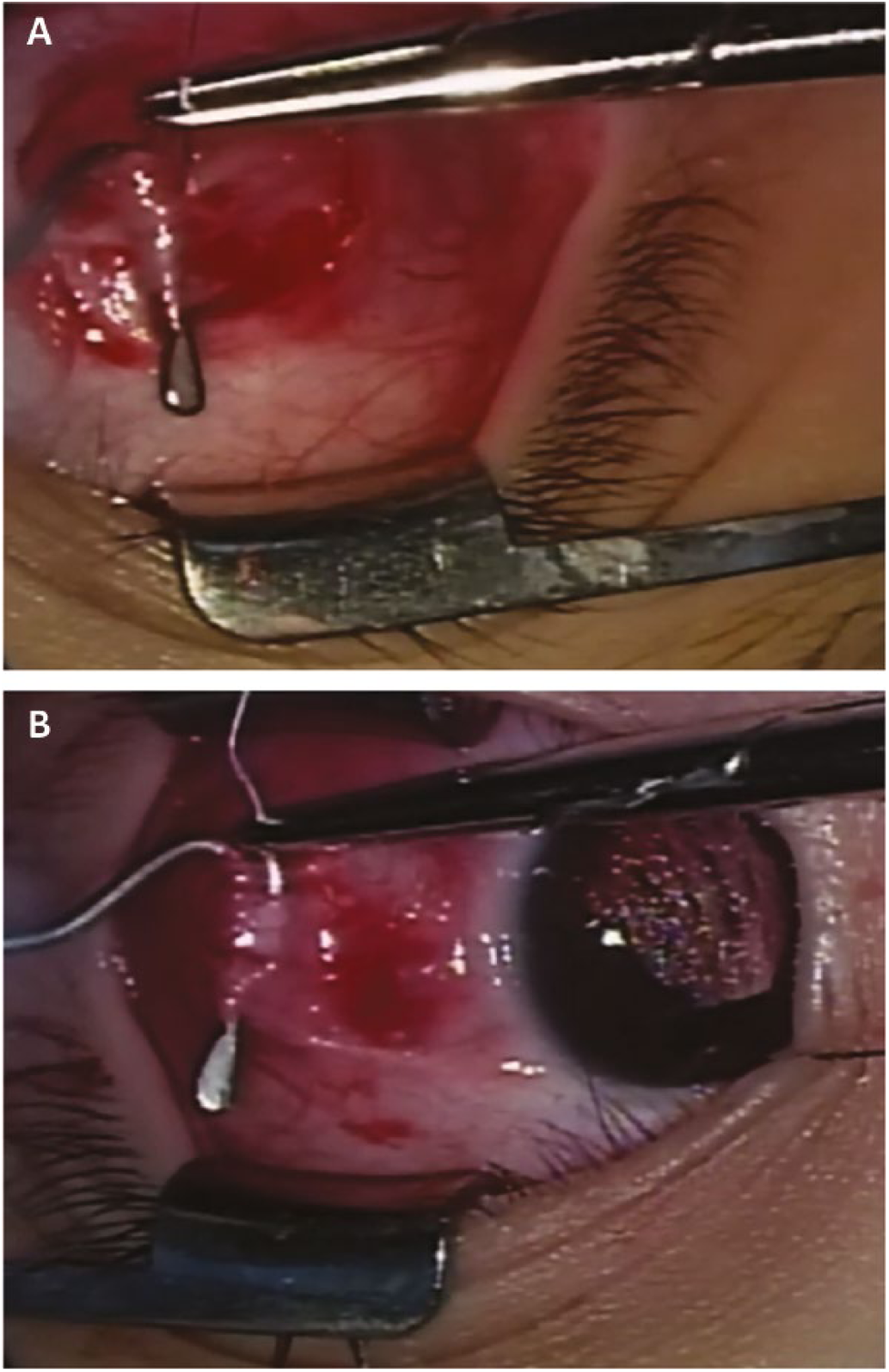
Difference of the location of the preplaced suture between right and left lateral rectus (LR) recession in actual surgical field. There was a difference in the preplaced suture position between the groups. (
The surgeon applied tension to the hook and the sutures while the muscle tendon was dissected from the sclera using tenotomy scissors, which were pressed firmly against the sclera to avoid a poor cosmetic appearance. After muscle disinsertion, the surgeon provided a mark to identify the site of reinsertion using calipers. While the assistant grasped the stump of the insertion remaining on the sclera with Castroviejo fixation forceps (Storz; Bausch & Lomb) and pulled on it, the surgeon inserted the needles through the sclera, entering the tissue at the mark and emerging slightly lateral and parallel to the limbus. The sutures were then tied and cut.
Outcome measures
The main surgical outcome measures were postoperative alignment and surgical success rate. Postoperative alignment at distance and near was measured at postoperative 1 day; 1 week; 1, 3, and 6 months; 1 and 2 years; and at final follow-up. Surgical success was defined as an alignment between 10 PD of exodeviation and 5 PD of esodeviation both at distance and at near.
As the secondary outcome measure, the effect/dose ratio was defined as the corrected angle of deviation at postoperative 6 months divided by the amount of LR recession.
Statistical analysis
All of the analyses were performed with statistical software (SPSS for Windows v 12.0.K). A Mann-Whitney U test was used to compare the preoperative characteristic data and angle of exodeviation at distance and near between the groups. A Pearson chi-square test was applied to compare the surgical success rates between the groups. A p value less than 0.05 was considered significant.
Results
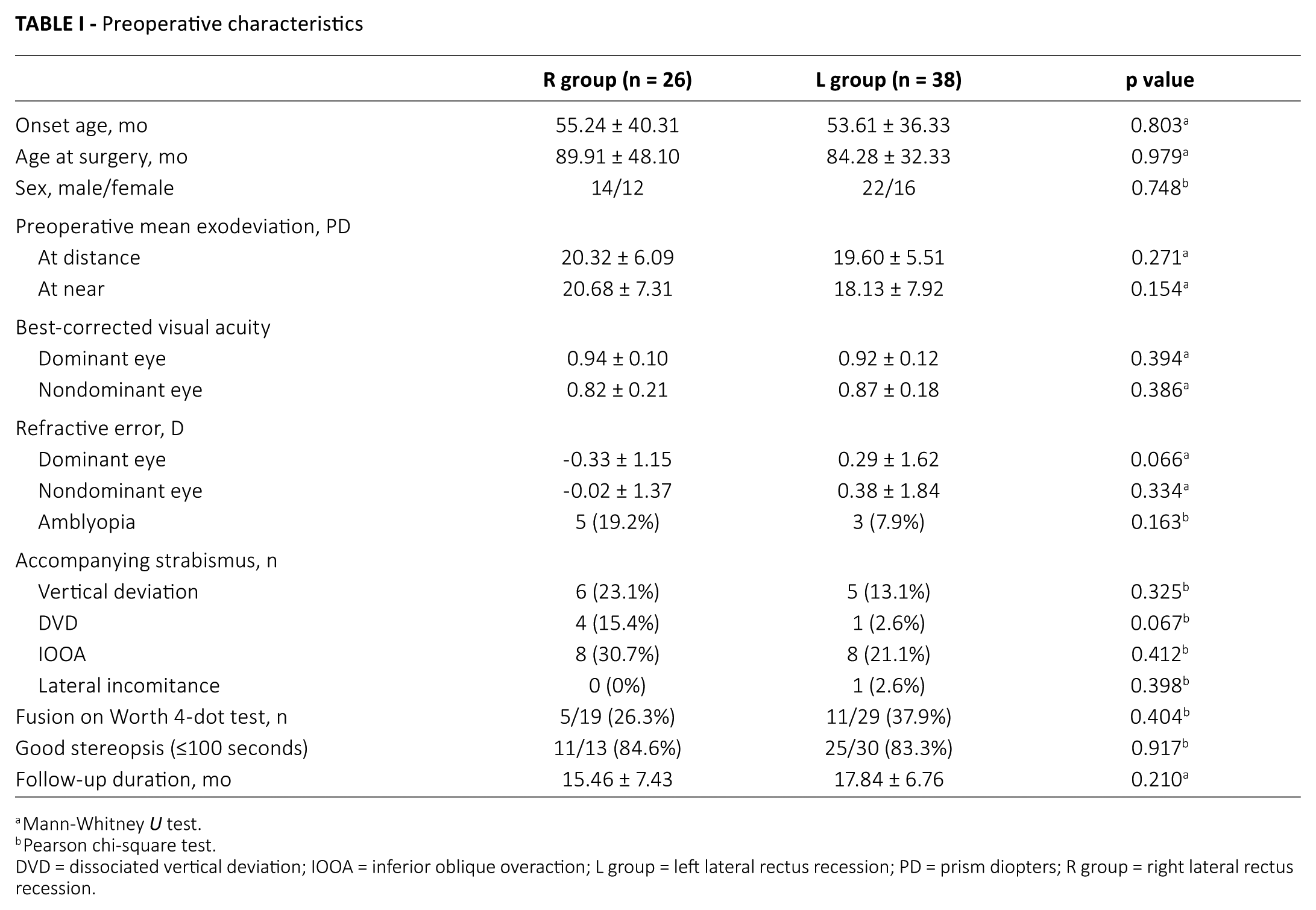
This retrospective study included 66 patients who had undergone unilateral LR recession. The patients were divided into 2 groups: right LR recession (R group, 26 patients) and left LR recession (L group, 38 patients).The mean age at surgery was 89.91 ± 48.10 months in the R group and 84.28 ± 32.33 months in the L group (p = 0.979). The mean follow-up duration was 15.46 ± 7.43 months in the R group and 17.84 ± 6.76 months in the L group (p = 0.210). There was no difference between the groups in sex, BCVA, refractive error, accompanying strabismus, good stereopsis, fusion on Worth 4-Dot test, or follow-up duration. The patient characteristics compiled in the preoperative evaluation are provided in Table I.
Preoperative characteristics
Mann-Whitney U test.
Pearson chi-square test.
DVD = dissociated vertical deviation; IOOA = inferior oblique overaction; L group = left lateral rectus recession; PD = prism diopters; R group = right lateral rectus recession.
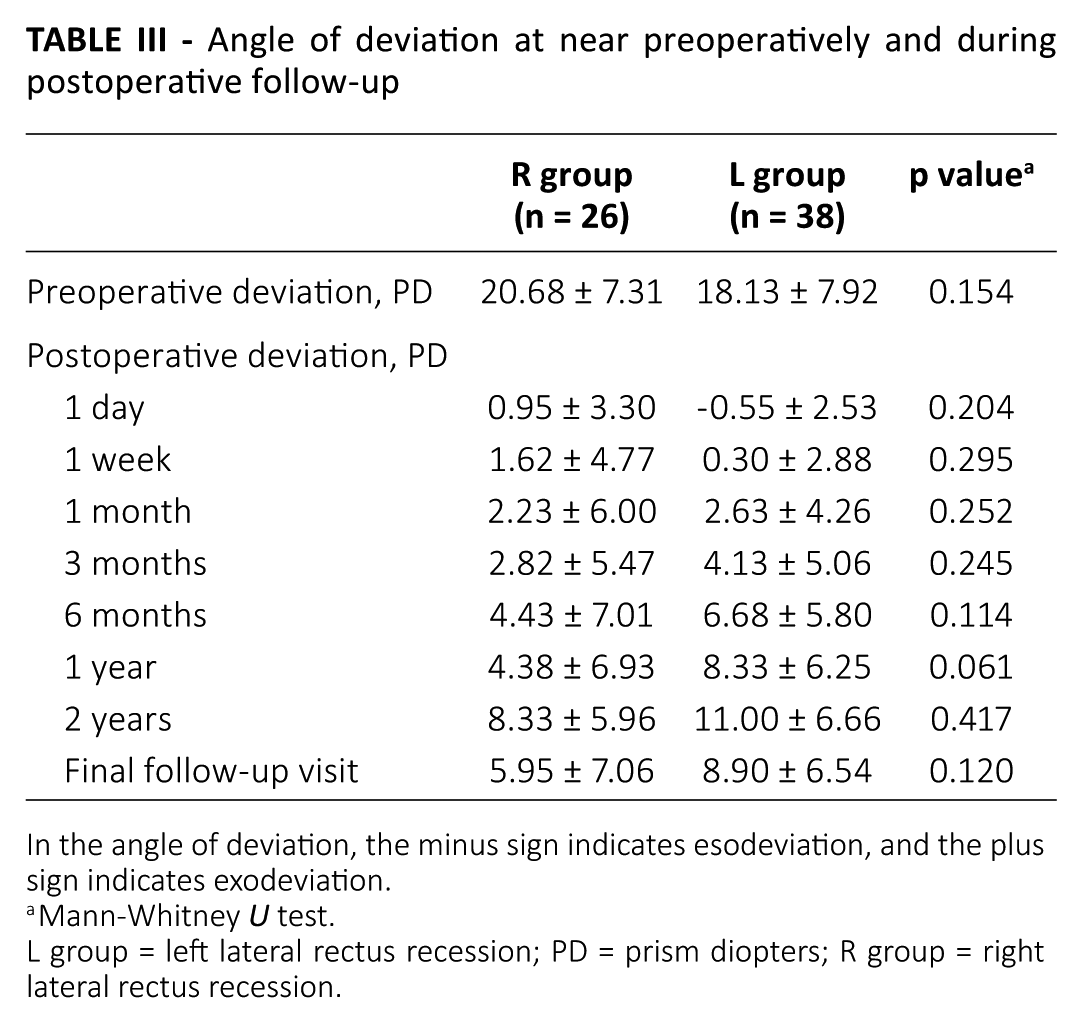
The mean angles of deviation at distance preoperatively and at the postoperative follow-up period are compared in Table II. The mean preoperative angles at distance were 20.32 ± 6.09 PD in the R group and 19.60 ± 5.51 PD in the L group (p = 0.271). The mean angles of exodeviation at postoperative 1 day were -0.69 ± 3.03 PD (esodeviation) in the R group and -0.55 ± 2.53 PD in the L group (p = 0.771). There was a significant difference in mean angle of deviation at postoperative 3 months (p = 0.022): the L group became more exotropic relative to the R group. However, there was no significant difference between the 2 groups at final follow-up (5.92 ± 7.06 PD in the R group, 7.86 ± 5.82 PD in the L group; p = 0.163). There was no significant difference between the groups in mean exodeviation at near, preoperatively or postoperatively (Tab. III).
Angle of deviation at distance preoperatively and during postoperative follow-up
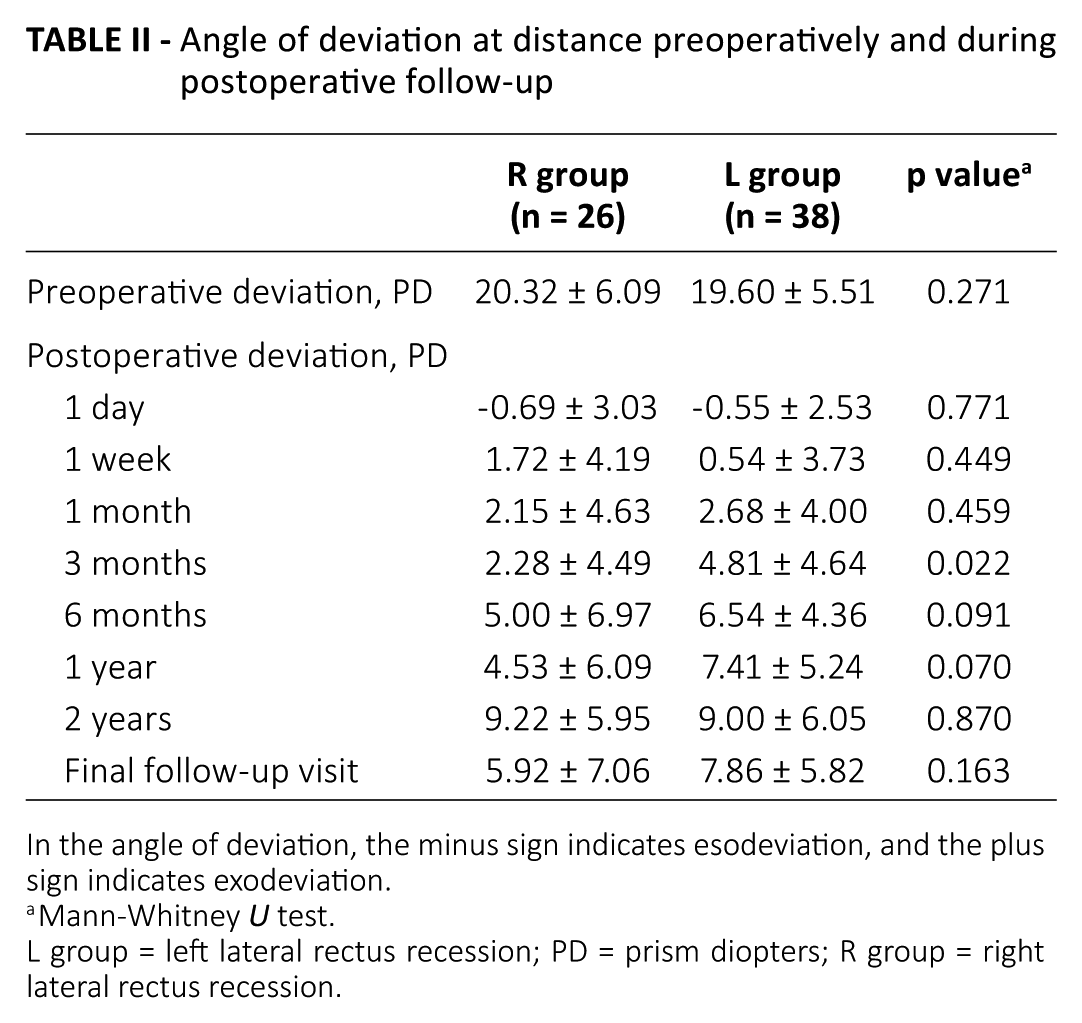
In the angle of deviation, the minus sign indicates esodeviation, and the plus sign indicates exodeviation.
Mann-Whitney U test.
L group = left lateral rectus recession; PD = prism diopters; R group = right lateral rectus recession.
Angle of deviation at near preoperatively and during postoperative follow-up
In the angle of deviation, the minus sign indicates esodeviation, and the plus sign indicates exodeviation.
Mann-Whitney U test.
L group = left lateral rectus recession; PD = prism diopters; R group = right lateral rectus recession.
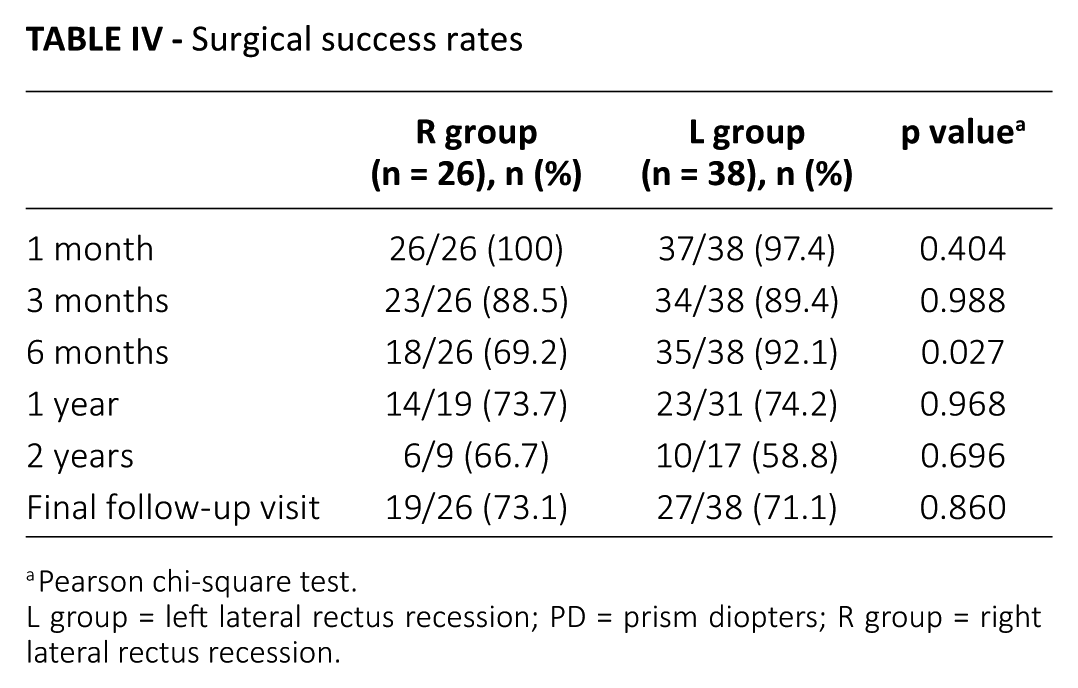
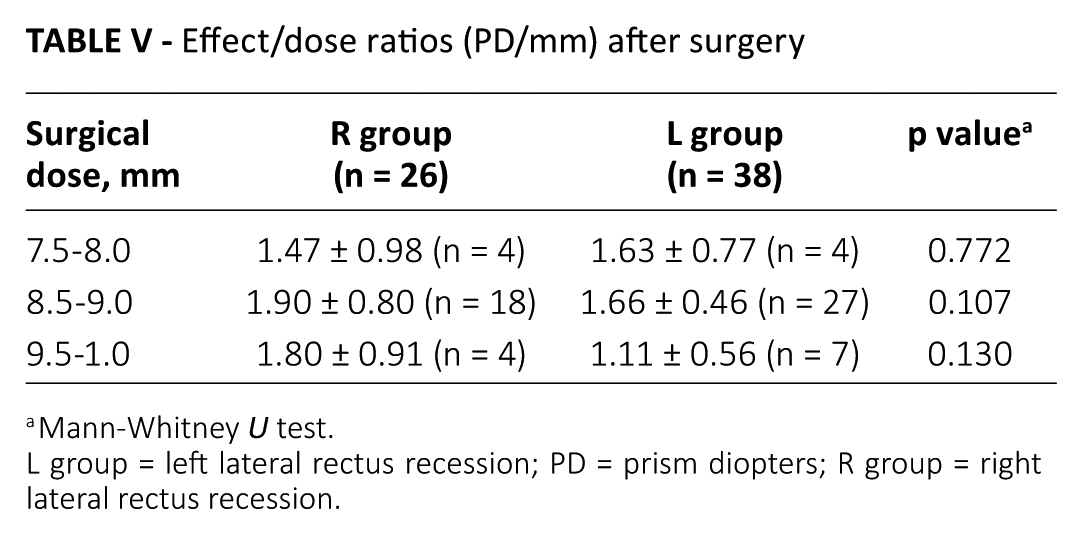
Table IV compares the surgical success rates between the groups. At postoperative 1 month, the success rate was 100% in the R group and 97.4% in the L group (p = 0.404). By final follow-up, success was achieved for 19 of 26 patients (73.1%) in the R group and 27 of 38 patients (71.1%) in the L group (p = 0.860). Overall, the R and L groups did not show any significant differences in their success rates at any of the postoperative visits, including the final follow-up. The effect/dose ratio of unilateral LR recession is compared in Table V. Each group was stratified for surgical doses and compared for the effect/dose ratio between the 2 groups. Consequently, there was no significant difference in the effect/dose ratio at any surgical dose between the R and L group (p>0.05). There was no intraoperative or postoperative complication.
Surgical success rates
Pearson chi-square test.
L group = left lateral rectus recession; PD = prism diopters; R group = right lateral rectus recession.
Effect/dose ratios (PD/mm) after surgery
Mann-Whitney U test.
L group = left lateral rectus recession; PD = prism diopters; R group = right lateral rectus recession.
Discussion
Unilateral LR recession as a treatment for moderate-angle exotropia has been studied since 1950 (3), and reported to be successful in various rates depending on the definition of success rate and the follow-up period (4-10). As in the author’s previous report, in a comparison study of unilateral LR recession and recession of the LR muscle and resection of the ipsilateral medial rectus muscle for intermittent exotropia of 20-25 PD, unilateral LR recession was an effective surgical method for moderate-angle intermittent exotropia, showing results similar to those of recess resect (11). Although a surgeon’s technique is determined, initially, by training, it eventually comes to incorporate his or her individual habits. In the present study, all of the surgeries were performed under general anesthesia by one right-handed surgeon. In the procedures, the right and left eyes differed in the insertion of the continuous double-armed suture through the rectus muscle. In the R group relative to the L group, the suture was positioned far from its insertion, approximately 1.0 mm by caliper measurement.
In this study, we reviewed the influence of the surgeon’s technique on the surgical results by comparing the distance between the preplaced suture and the muscle insertion in LR recession for exotropia. The results indicated that the distance between the preplaced suture and the muscle insertion in the LR recessions did not affect the surgical success rates or the postoperative alignment at final follow-up. The groups’ mean deviation angles at postoperative 3 months and 1 year were significantly different, the L group showing more exotropic drift.
Lateral rectus recession imparts muscle laxity and reduces muscle strength (1), because recession alters the tangential point of the muscle, thus changing the direction of the force and making for partial loss of mechanical force (12). In this aspect, the results of the present study were rather unexpected, as the suture was located far from the insertion in the R group, causing, at least theoretically, a slight decrease of the recession effect. We were unable to explain the exact underlying mechanism of the results we obtained. A possible explanation is that sensory-motor mechanisms might hang up the eyes regardless of small angle variations when normal binocular vision is present, making the small differences in the alignment that lie immediately after the surgery disappear in the following months. The issue will have to await confirmation by further, prospective evaluation with a larger sample. Nonetheless, there was no significant difference in mean angle of deviation or success rate between the 2 groups at final follow-up.
According to the textbook approach, as regards preplaced suture location, sutures are inserted and locked to the lower and upper edges of the muscle close to the insertion in order to maintain surgical doses strictly (13, 14). In actual practice, surgeons, especially beginners, are concerned about accidental cutting of preplaced sutures during disinsertion of the recessed muscle if the suture is positioned so close to the insertion. But as the present study demonstrated, surgeons need not worry about small changes in preplaced suture position.
This study has several limitations. First, as a retrospective study, the data obtained from the medical records were not complete. Also, the sample sizes were relatively small and the subjects were recruited consecutively. The third drawback of this study was that all of the surgeries were performed by a single right-handed surgeon; the results therefore will have to be confirmed by other surgeons. Further prospective and comparative study with larger sample sizes is required.
In conclusion, the distance between the preplaced suture and the muscle insertion in LR recession did not affect the surgical success rate or the postoperative alignment at final follow-up.
Footnotes
Disclosures
Financial support: No financial support was received for this submission.
Conflict of interest: None of the authors has conflict of interest with this submission.