
Abstract
Acute coronary syndrome (ACS) due to embolic phenomenon in the setting of peripartum cardiomyopathy (PPCM) and left ventricular mural thrombus is a rare occurrence. There have been two known cases described in medical literature. We present a unique case in which catheter-based aspiration thrombectomy was used to successfully treat a patient with ACS due to coronary emboli in the setting of PPCMand left ventricular mural thrombus. We believe this to be the first report of the use of aspiration thrombectomy in such a clinical case.
Case report
We report on a 28-year-old woman, who presented two months postpartum after delivering twins with complaints of transient ischemic attack (TIA), dyspnea and chest pain. Physical examination demonstrated jugular venous distention (JVD) and s3 gallop on cardiac auscultation along with minimal rales and pedal edema. Her electrocardiogram (ECG)
showed sinus tachycardia with lateral T wave inversion (Fig. 1). Laboratory work up revealed an elevation in her cardiac biomarkers with a peak troponin-I level of 10.2 ng/mL. The echocardiogram showed moderate left ventricular (LV) dilatation with severely reduced LV systolic function and left ventricular ejection fraction (LVEF) <15% associated with a 2.1 cm apical thrombus (Fig. 2). Given the chest pain, elevated cardiac biomarkers and ECG changes suggestive of ischemia, a coronary angiography was performed which revealed two filling defects in the distal segment of the second obtuse marginal artery with a hazy appearance consistent with thrombi (Fig. 3). The rest of the coronary arteries were angiographically normal. Aspiration thrombectomy was performed with multiple passes at the site of thrombi and fresh clot was retrieved (Fig. 4). Repeat images were performed and showed resolution of the thrombus (Fig. 5). Post-procedure, the patient did well; her troponin-I levels down-trended and her symptoms improved. She was started on oral anticoagulation for treatment for left ventricular apical thrombus and she was strongly counseled on avoidance of future pregnancies and tubal ligation. She was discharged on oral anticoagulation, and guideline directed heart failure medical therapy.

Electrocardiogram: with lateral T wave inversion.
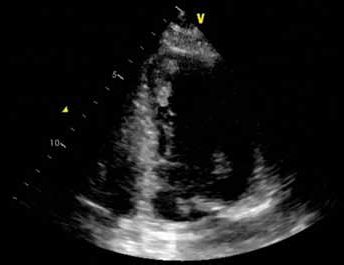
Apical two-chamber view of the heart with left ventricular thrombus shown.

Two sequential thrombi in the distal segment of the obtuse marginal 2 (OM2).

Fresh thrombus which was aspirated from the distal obtuse marginal 2 (OM2).

Repeat images demonstrating resolution of the stenosis in the obtuse marginal 2 (OM2).
Discussion
Peripartum cardiomyopathy (PPCM) is characterized by the development of heart failure during the last month of pregnancy or during the first five months of the post-partum period in the absence of any other identifiable causes of heart failure (1, 2). Several risk factors have been identified with PPCM including ethnicity, age, pregnancy-induced hypertension or pre-eclampsia, multiparity, multiple gestations, obesity and chronic use of tocolytics (2). In the case described, multiple gestations, pregnancy with twins, and African descent were identified as significant clinical risk factors. PPCM is known to increase the risk of thrombus formation and arterial emboli (3, 4). The risk of acute myocardial infarction is approximately three times higher in pregnant women compared to non-pregnant women of the same age (5-6-7-8). In our case, the inherent hypercoaguable state that exists in pregnancy along with poor LV systolic function and resulting stasis of blood flow in dilated heart, likely provided an environment for the development of an intraventricular thrombus (3, 4). The findings of two intracoronary thrombi in the setting of otherwise normal coronary arteries, which were free of atherosclerotic disease, suggests embolism from LV mural thrombus as the primary mechanism of her coronary thrombi and myocardial infarction. Upon review of available literature there are only two reported cases of embolic myocardial infarction in the setting of PPCM and an associated LV thrombus (9, 10). Our case is unique in the aspect that catheter-based aspiration thrombectomy was performed safely for reperfusion therapy and was successful with the resolution of thrombus as documented angiographically (Fig. 5). Based upon these results, we propose that it be considered as a treatment modality in future similar cases in the absence of contraindications.
Footnotes
Financial support: None.
Conflict of interest: None.