
Abstract
Purpose
Cardiac screening in adult kidney transplant candidates with myocardial perfusion scintigraphy (MPS) can reveal findings associated with increased risk for coronary heart disease events, but the exact value of this screening test is still undetermined.
Methods
Narrative review based on the available literature and guidelines on the yield, benefits, and harms of MPS screening in kidney transplant candidates.
Results
Although coronary angiography carries low risk in general population, it is not without risk particularly in patients with complex comorbid disease and the use of intravenous contrast media may precipitate a need for hospitalization and death. We could avoid invasive coronary angiography in patients with chronic kidney disease, although with high coronary calcium score, but good left ventricle function and normal perfusion, evaluated by Gated single-photon emission computed tomographic (SPECT) MPS. In fact, although Gated SPECT MPS has not a high sensitivity, it provides some variables that are closely related to sudden death: post-stress and rest-ejection fraction and left ventricular volumes, left ventricle muscle mass, extent of ischemia and scar.
Conclusions
Gated SPECT MPS is a valid noninvasive cardiac screening test. It can be used as alternative to stress echocardiography in kidney transplant candidates with high cardiovascular risk and a positive or inconclusive exercise tolerance ECG test.
Patients with abnormal perfusion and cardiac dysfunction should undergo invasive coronary artery imaging and endovascular treatment, while angiography could be avoided in patients with normal MPI, having good long-term prognosis.
Introduction
Patients with chronic kidney disease (CKD) have a high risk of cardiovascular (CV) events, but the majority of deaths are due to sudden cardiac death, arrhythmia, congestive heart failure, with relatively few caused by vascular events such as myocardial infarction (1). In addition, symptoms of coronary artery disease (CAD) may be atypical due to neuropathy, over-hydration, or low functional capacity. No prospective study has yet demonstrated the benefit of cardiac risk stratification before kidney transplantation. In selected high-risk patients, early referral to cardiac catheterization and coronary revascularization may improve outcomes (2). However, acute deterioration of renal function following diagnostic coronary angiography occurs in approximately 10% of patients (3) and in up to 30% of patients after percutaneous coronary intervention (4). Contrast medium-induced renal dysfunction after coronary procedures carries poor prognosis, especially if dialysis becomes necessary (4, 5). Even in patients already undergoing dialysis, loss of residual renal function is associated with worse outcomes. In addition, coronary revascularization procedures in patients with renal impairment are associated with markedly higher risks of both fatal and nonfatal adverse outcomes (6, 7). Even after transplantation, patients remain at high risk of long-term CV complications. Consequently, careful selection of high-risk patients for referral to coronary angiography and revascularization is of paramount importance. In this review article we address the role of myocardial perfusion scintigraphy as a cardiac screening tool in kidney transplant candidates.
Current status of cardiac evaluation for kidney transplant candidates
To ensure that graft survival is not limited by premature CV death, several regulatory agencies and scientific societies (Tab. I) recommend noninvasive CV assessment of those transplant candidates with multiple risk factors or diabetes, although there is no clear guidance on which imaging method to use (8-9-10-11-12-13). Overall, the current suggestion is to adopt an imaging protocol for CV stratification according to “best local expertise”.
Recommendations of different guidelines on noninvasive stress testing
The UK Renal Association suggests that there is no compelling evidence that pre-transplantation screening for coronary artery disease with subsequent coronary intervention is effective in patients with established renal failure in preventing future cardiac events or reducing mortality after transplantation. However, the UK Renal Association also indicates that screening tests may be used to identify high-risk patients for exclusion from the transplant waiting list (9).
Accordingly, many transplant centers continue to use stress/rest myocardial perfusion single-photon emission computed tomographic (SPECT) imaging because of long-standing data supporting its prognostic utility in end-stage renal disease (ESRD) (14-15-16-17).
Technical aspects of myocardial perfusion scintigraphy
The most used tracers for MPS are the isonitrile compounds labeled with technetium-99m (99mTc): sestamibi and tetrofosmin. These tracers distribute in the myocardium proportionally to regional blood flow and, after entering the myocardial cells, have an extremely low washout, allowing the acquisition of perfusion images up to two hours from the injection. It is therefore necessary to perform a double injection in order to compare the myocardial perfusion after stress and at rest. The two studies are carried out preferably on different days. An average activity of 740 MBq is used for each study. The estimated effective radiation dose to the patients is 10 mSv for a two-day protocol, compared to 15-20 mSv of a coronary computed tomography angiography (18).
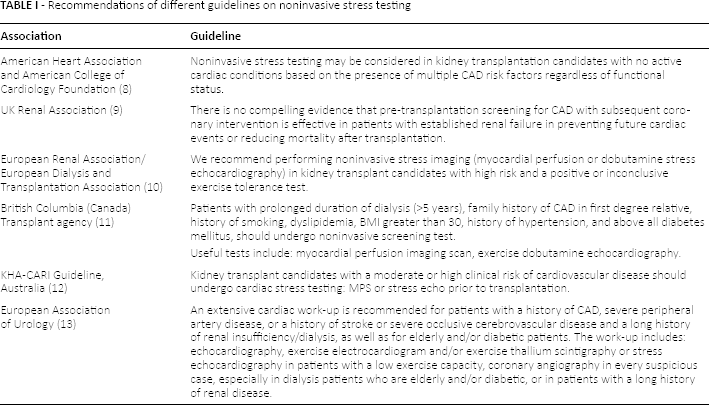
The tomographic acquisition (SPECT) is currently performed with dual headed gamma cameras, with variable geometry. The tomographic sections obtained allow a good visualization of the left ventricle, whose walls have a greater thickness than those of the others chambers of the heart. The acquisition with gated technique allows to evaluate ejection fraction, left ventricular volumes, and regional myocardial motility with no additional time and dose. MPI provides functional significance of any coronary stenosis, while coronary angiography provides morphological information of coronary tree.
In normal subjects, there is a homogeneous tracer uptake inside the left ventricle walls (Fig. 1A).
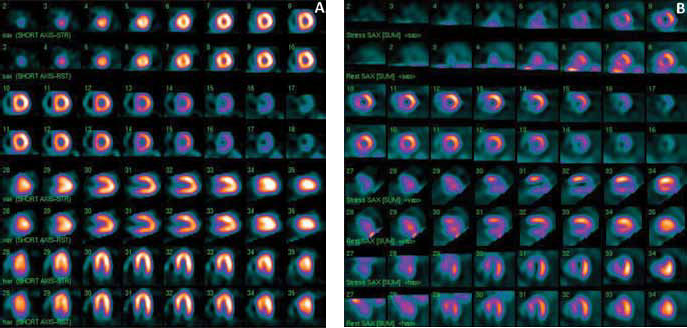
(
The presence of fixed defects in both stress and rest images is usually expression of myocardial infarction, or very severe ischemia, while the presence of reversible defects is expression of transient ischemic changes (Fig. 1B).
Performance of myocardial perfusion scintigraphy
The diagnostic accuracy of a noninvasive test like myocardial perfusion scintigraphy is low. Wang et al (19) performed a systematic review of the diagnostic test accuracy of MPS compared with angiography in detecting significant CAD in potential kidney transplant recipients. Seven studies (317 participants) evaluated MPS (20-21-22-23-24-25-26). The sensitivity of MPS varied from 29%-92%, and specificity, from 50%-88%. Pooled sensitivity was 0.69 (95% CI, 0.48-0.85), and specificity was 0.77 (95% CI, 0.59-0.89). Removing from the analysis the only one study (24) which used a reference threshold of ≥50% stenosis instead of ≥70% stenosis, the pooled sensitivity was 0.68 (95% CI, 0.43-0.85), and specificity improved to 0.80 (95% CI, 0.60-0.91). Patients with end-stage kidney disease often have hypertension, left ventricular hypertrophy, and decreased coronary flow reserve, all of which may account for the decreased specificity of MPS in transplant candidates, due to the higher incidence of false-positive uptake defects (27). The reason for the low sensitivity of MPS in transplant recipients compared with the general population is less clear. One possible explanation is that any discrepancy between MPI and coronary angiography can depend on the fact that the coronary angiography provides morphological information of coronary tree, while the MPI provides the functional significance of any coronary stenosis. Another explanation may be cardiac parasympathetic denervation, particularly in diabetic patients who have CKD, which would decrease the relative efficacy of dipyridamole (routinely used in MPS as stress test) compared with dobutamine (routinely used in stress echocardiography) (28, 29). In fact, three studies of the Cochrane review (22-23-24) included only diabetic patients. Moreover, MPS is not able to detect subclinical atherosclerosis, potentially predisposing the patient in the longer term to subsequent obstructive CV events.
Alternative methods for cardiac risk evaluation in kidney transplant candidates
Hybrid SPECT/CT imaging offers the opportunity to combine anatomic evaluation of coronary stenosis alongside a functional assessment of myocardial ischemia. The coronary artery calcium score (CACS), as assessed by using non-enhanced CT, provides an absolute measure of coronary calcification, adds prognostic information, and correlates moderately with obstructive CAD (30, 31). Coronary computed tomography angiography (CTA) has been shown in several multicenter studies to have a high sensitivity (30, 32). However, its specificity is not optimal due to false-positive results in patients with extensive coronary calcifications or high/irregular heart rates. Winther et al (33) compared the accuracy of diagnosing obstructive CAD by using CACS, coronary CTA and SPECT (with invasive coronary angiography as the reference) in 138 patients referred for pre-transplant cardiac evaluation: 43% treated with dialysis. In a patient-level model, the sensitivity and specificity, respectively, for diagnosing obstructive CAD were: CACS (threshold of 400), 67% and 77%; coronary CTA, 93% and 63%; SPECT MPS, 53% and 82%; hybrid (CACS/SPECT), 33% and 97%; and hybrid (coronary CTA/SPECT), 67% and 86%. The authors concluded that coronary CTA is a reliable test with high sensitivity and a high negative predictive value for diagnosing obstructive CAD before kidney transplantation. A noninvasive approach using either coronary CTA or a combination of coronary CTA and SPECT to rule out obstructive CAD seems recommendable. The reduced diagnostic performance of MPS SPECT in advanced CKD patients may be due to false-negative results in patients with severe CAD and balanced ischemia, in addition to an impaired response to myocardial stress agents. Noninvasive imaging methods are insensitive for detecting the presence of diffuse mild atherosclerosis and its impact on coronary epicardial and microcirculatory function and myocardial ischemia. Several investigations have suggested that renal disease is associated with abnormal coronary vasodilator function (34), which may result from multiple mechanisms (35), including decreased capillary density (36), leading to microvascular dysfunction as well as vascular remodeling in epicardial arteries (37). Noninvasive measure of coronary vasodilator reserve by positron emission tomography (PET) perfusion agents, integrates the hemodynamic effects of local epicardial coronary stenosis, the fluid dynamic effects of diffuse atherosclerosis, and the presence of coronary microvascular dysfunction (29, 38).
Prognostic value of myocardial perfusion scintigraphy
MPS has been validated as a powerful prognostic tool for predicting adverse cardiovascular outcomes in patients with known or suspected CAD. Wong et al (39) showed that a positive 99mTc myocardial perfusion scanning, defined by the presence of a reversible defect, was associated with three times the risk of post-transplantation cardiac events and nearly twice the risk of death compared with normal test results. Aalten et al (40), demonstrated that after the introduction of the standardized cardiac assessment program, the incidence of significant cardiac ischemia assessed by noninvasive cardiac stress testing in high-risk renal transplant patients was low (6.6%) and was followed by revascularization in 67% of positive tests (4.4% of the tested population). A non-significant decrease in kidney transplant perioperative cardiac events (3.8% vs. 7.6% of historic controls) was observed.
Gated SPECT MPS, which allows a simultaneous evaluation of myocardial perfusion and function, increments the prognostic power of MPS (41-42-43-44-45). Hakeem et al (17) assessed the prognostic utility of Gated SPECT MPS in patients with varying degrees of renal dysfunction and the impact of CKD on cardiac death prediction. The study population was predominantly composed of patients with stage III CKD. Presence of ischemia was independently predictive of cardiac death, all-cause mortality, and nonfatal myocardial infarction. Patients with normal MPS and CKD had higher cardiac death event rates than those with no CKD and normal MPS (2.7% vs. 0.8%, p = 0.001). Multivariate Cox analysis revealed that both perfusion defects (hazard ratio [HR]: 1.90, 95% CI 1.47 to 2.46) and CKD (HR 1.96, 95% CI 1.29 to 2.95) were independent predictors of cardiac death after accounting for risk factors, left ventricular dysfunction, pharmacological stress, and symptoms. The results are in agreement with those of the meta-analysis by Rabbat et al (15), which evaluated the prognostic utility of thallium MPS for predicting myocardial infarction (MI) and cardiac death (CD) in patients with ESRD (stage V) assessed for kidney and kidney-pancreas transplantation. Patients with inducible ischemia had a 6-fold increased risk of MI and a 4-fold increased risk of CD, whereas fixed defects (scars) were only predictive of CD (relative risk 4.7) and not of MI. The increased rate of CD relative to baseline in the group of CKD and normal MPS (2.7% vs. 0.8%), is very close to the 3% reference value defined as high risk by the American College of Cardiology/American Heart Association, and may be due to mechanisms other than myocardial ischemia. There is growing evidence that patients with CKD have unrecognized left-ventricle dysfunction, both systolic and diastolic. The addition of ejection fraction to the Cox analysis greatly increased the X2 index, indicating the importance of left-ventricle systolic dysfunction (ejection fraction <40%) as a predictor of CD in patients with CKD. Similar results were obtained by Venkataraman et al (14) which examined the prognostic power of MPI in 150 patients with ESRD candidates for renal transplantation with known coronary anatomy using angiography, followed for 3.4 years. In a multivariate model, abnormal MPS results (left-ventricle ejection fraction ≤40% or abnormal perfusion) was the strongest independent predictor of all-cause mortality (adjusted OR 2.5, 95% CI 1.2 to 5.3, p = 0.012). Diabetes mellitus was also an independent predictor, with an adjusted OR of 2.2, whereas the number of narrowed arteries using coronary angiography was not. Gated SPECT MPS provides some variables that might be related to sudden death: post-stress and rest-ejection fraction and left-ventricular volumes, left-ventricle muscle mass, extent of ischemia and scar. This may explain the superiority of MPS over coronary angiography in predicting death. In a recently published study, Moody et al (46) evaluated the prognostic utility of calcium scoring as an adjunct to MPS in ESRD obtained by hybrid technology SPECT/CT. Coronary artery calcium score (CACS) is in fact a surrogate marker of atherosclerotic burden and a strong predictor of adverse cardiovascular events in subjects at intermediate risk from the general population (47). In the multivariate model, abnormal perfusion on SPECT (HR 4.18, 95% CI 1.43 to 12.27, p = 0.009), but not moderate-to-severe CACS (HR 2.4, 95% CI 0.76 to 8.20; p = 0.13), independently predicted all-cause death or MI. The risk of CD and MI increased significantly with the presence and extent of SPECT abnormality. Therefore, MPS continues to be a useful method to identify those subjects with ESRD at high cardiovascular risk. In a study of 1126 largely asymptomatic patients with no ESRD, after a much longer duration of follow-up (median 6.9 years), Chang et al (48) demonstrated that CACS offered incremental risk prediction in subjects with a normal perfusion result. The relative increase in all-cause death/MI was limited to those with high CACS (>400 U) and survival curves only began separating after 3 years. The follow-up duration of only a median of 18 months in the study of Moody et al (46) could be an explanation for the failure of CACS to provide incremental risk predictive value over SPECT. A second possible explanation relates to the particular pathophysiology of arterial calcification in ESRD (1), that is not limited to the intima as in atherosclerosis, causing obstructive coronary disease, but also affects the media (arteriosclerosis), which is associated with pressure overload and heart failure. Moreover, the prevalence of moderate and severe CACS in these patients may be a consequence of other factors including abnormal calcium-phosphate handling, rather than reflecting atherosclerosis alone. The high rates of left ventricle hypertrophy, dilatation, and fibrosis in CKD and their robust association with an adverse cardiovascular prognosis offer alternative targets for intervention (49-50-51).
Cardiac surveillance awaiting kidney transplantation
Cardiac surveillance by MPS while on the waiting list for transplantation is another area of uncertainty. The optimal frequency for repeat noninvasive stress testing for patients awaiting kidney transplantation is unknown. Cardiac surveillance policies among listed candidates differ across transplant centers. Among 68 transplant centers surveyed to determine current practices, 18% did not reevaluate candidates (52). About half of centers relied on the initial cardiac evaluation and cardiac history, with varying criteria used to determine cardiovascular status.
Kidney Disease Outcomes Quality Initiative guidelines (53) indicated an evaluation of coronary artery disease in dialysis patients, dependent on individual patient status, ranging from 12 months (diabetics, high-risk patients) to 36 months (low-risk patients). In patients fulfilling criteria for individual risk, coronary artery disease evaluation should also include exercise or pharmacological stress echocardiographic or nuclear imaging tests (53) especially in symptomatic patients.
In a more recent assessment, it was recommended that the usefulness of periodically screening asymptomatic kidney transplantation candidates for myocardial ischemia while on the transplant waiting list to reduce the risk of major adverse cardiovascular events is uncertain (8).
Conclusion
MPS is a valid noninvasive cardiac screening test. It can be used as an alternative to stress echocardiography in kidney transplant candidates with high cardiovascular risk and a positive or inconclusive exercise tolerance ECG test. Recent suggestions of adding a coronary artery calcium score do not seem to improve sensitivity and specificity of MPS, which are suboptimal. A perfusion defect on MPS associated to abnormal contractile function being an independent predictor of adverse outcome in potential renal transplant candidates, should be evaluated by invasive coronary artery imaging and, if necessary, submitted to endovascular treatment. Otherwise patients with normal MPI, having good long-term prognosis, may not undergo angiography.
Footnotes
Financial support: No grants or funding have been received for this study.
Conflict of interest: None of the authors has financial interest related to this study to disclose.