
Abstract
During the last 25 years uncemented hip stem revision relying on diaphyseal fixation has shown improving clinical results and stem survival. The purpose of this study was to present the long-term results of hip revision with the SOLUTION stem (DePuy Warsaw Indiana).
Ninety-three consecutive SOLUTION hip stem revisions in 84 patients with a mean age of 69 years (range 33-86 years) were reviewed. Of these, clinical and radiographic follow-up examination by an independent observer was possible in 36 hips/29 patients after mean 14 years (range 10-18 years). Stem re-revision was documented by our own files and by the Danish Hip Arthroplasty Registry.
Stem re-revision had been performed in two hips for aseptic loosening, one due to deep infection and in one patient due to stem fracture. The 18 years cumulative survival, free of re-revision for any reason was calculated as 94.4% (88.9-99.8)% and for aseptic loosening to 97.6% (94.3-100%). Intraoperative complications were frequent with incidence of shaft fractures (14/93) and perforations (9/93) showing a significant learning curve. Mean Harris Hip Score was 85 (range 53-99). Osseointegration was seen in 34/36 stems with two stems fibrous fixated. Stress shielding was significant associated with stem diameters ≥15 mm. Severe preoperative bone deficiency had no negative bearing on stem survival and no significant influence on osseointegration of the stem or on Harris Hip Score.
Conclusion:
Femoral stem revision with an extensively porous-coated monoblock chrome-cobalt stem seems to be a reliable and reproducible technique resulting in excellent long-term survivorship and clinical outcome. It can be used in femurs with deficient bone stock.
Introduction
Revision hip arthroplasty has by health economic standards been shown to be an excellent cost-effective procedure, reducing pain and improving function and quality of life for patients with loose or otherwise malfunctioning hip prostheses (1). The goals of hip revision surgery are to restore and maintain lasting mechanical stability, to prevent further bone loss and ideally to promote new bone formation. Up to the 1980s these goals had not been fulfilled by cemented hip revision arthroplasty because of high incidences of progressive radiographic loosening, mechanical failure and re-revision (2–4).
As a consequence we changed from cemented to cement-less hip revision in 1986 choosing the 5/8th porous-coated AML stem (DePuy, Warsaw, Indiana) and the Trilock acetabular cup (DePuy, Warsaw, Indiana). Initially our results were promising, but within a few years we unfortunately experienced a significant increase in stem re-revisions with an 88.4% cumulative five years survival from re-revision of any reason (5). In our opinion the main reason for these unsatisfactory results was insufficient stem-bone contact in the isthmus area of femurs with severe distal bone stock damage rendering primary stem stability and bone ingrowth difficult. Inspired by the results published by Engh et al (6), we addressed this problem by changing to the extensively porous-coated monoblock chrome-cobalt Solution stem (DePuy, Warsaw, Indiana). This stem bypasses the damaged proximal femoral bone relying on distal fixation in the diaphysis and has been our standard device in femoral stem revision since October 1992.
The aim of this study is to report the 18 years cumulative survival of our first consecutive 93 Solution stem revisions and the 10-18 years clinical and radiographic outcome.
Patients and Methods
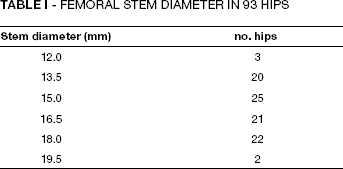
From October 1992 to October 1999 ninety-three consecutive SOLUTION stem revisions were performed by two surgeons (JK and PBT) in 36 women and 48 men with a mean age of 69 years (range 33-86 years). The SOLUTION stem is an extensively porous-coated cylindrical mono-block chrome-cobalt prosthesis. Stem range includes six and eight inch straight stems ranging between 10.5 and 22.5 mm in diameter together with eight and 10 inch bowed stems ranging between 13.5 and 22.5 mm in diameter and also calcar replacement stems. Our patients only received eight inch straight (nine hips) and 8/10 inch bowed stems (84 hips) combined with a modular 28 mm chrome-cobalt head. Stem diameter distribution is shown in Table I. Calcar replacement stems were not used. In 19 hips the acetabular cup was well fixed and not revised. Modular polyethylene liners however were always exchanged. In 74 hips the acetabular cup was revised to an uncemented hemispherical porous-coated cup (73 hips) or an Oblong cup (one hip).
Femoral Stem Diameter in 93 Hips
Routine antibiotic prophylaxis with Dicloxacillin and thromboembolic prophylaxis with Enoxaparin was employed. A postero-lateral approach and line to line reaming of the femoral canal to avoid splitting of the bone on insertion of the stem was utilised. Trochanteric osteotomy or prophylactic cerclage wiring to minimize intraoperative fractures/ perforations were used in three procedures. Postoperatively patients were mobilised with protective weight bearing for six to 12 weeks according to symptoms and radiographic appearance of the hip.
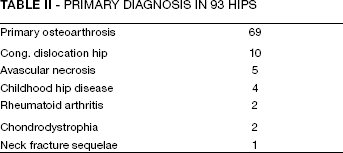
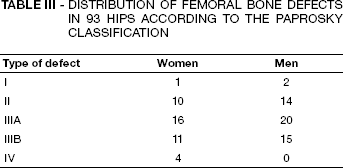
The reason for stem revision was aseptic loosening in 90 hips (64 cemented and 26 uncemented), deep infection in 2 cemented hips and intractable hip and thigh pain in one uncemented hip. In 71 hips it was the first revision operation, in 18 the second and in four hips the third revision. The revision operation was performed a mean of 9 years (range 1-19 years) after the previous arthroplasty. The primary diagnosis is shown in Table II and only 16 patients were Charnley class 1 while 44 suffered from bilateral hip disease and 33 had concurrent incapacitating illness. Bone transplantation was performed in 43 proximal femurs, not as impaction grafting but simply by ramming allogenic bone chips into the bone defects. No strut grafts were used. The distribution of femoral bone defects according to the Paprosky Classification (7), evaluated on preoperative AP X-rays is shown in Table III. Clinical and radiographic follow-up was performed by an independent observer (NJ) at a mean of 14 years (range 10-18 years) after the index stem revision operation. The Harris Hip Score (8) was used for clinical evaluation and ra-diographic assessment was undertaken by comparing the immediate postoperative AP radiographs with radiographs at the time of follow-up. Subsidence of the stem within the femur was defined as more than 5 mm distal migration of the stem measured by the distance from the stem shoulder to the tip of the greater trochanter on radiographs taken with the patient in supine position and feet in neutral. Fixation of the stem was evaluated according to the criteria by Engh et al (9) and bone remodelling changes were assessed in the different Gruen zones (10). Stress shielding was assessed using the criteria of Engh and Bobyn (11).
PRIMARY DIAGNOSIS IN 93 HIPS
Distribution of Femoral Bone Defects in 93 Hips According to The Paprosky Classification
Statistics
Statistical analysis was performed using Fisher Exact test. Significance was determined at a P-value less than 0.05. Survival analysis was undertaken using a Kaplan Meier survival analysis (12). For calculation of the survival analysis we used XLSTAT.
Results
At the time of latest follow-up 46 patients/48 hips had died after a mean follow-up of 62 months (range 1-118 months), all with the revision stem in situ documented by the Danish Hip Registry and our own files. Four stems had been revised, two because of aseptic loosening at 22 and 55 months respectively after the index revision operation. Both these stems were probably undersized. One patient had a 2-stage total hip re-revision because of deep infection with Staphylococcus epidermidis after seven years. One hip was re-revised after nearly 10 years because of stem fracture at the transition between the ingrown distal part and the bony unsupported proximal part of the stem in a Paprosky type 3a femur (Fig. 1). In three of the re-revised hips the index SOLUTION revision was the first revision operation and in one the second. None of these hips were Paprosky type 3b or type 4. Five patients/hips did not attend the final follow-up examination. Three could not (bad health) or would not attend, but all reported the revision stem in situ by telephone. Two patients/hips could not be traced, but according to our own files and to the Danish Hip Registry none of them have had stem re-revision. However, in a worst case scenario these two hips must be considered as failures.

Stem fracture nearly 10 years after the index revision operation.
This leaves 36 hips/29 patients for clinical and radiographic follow-up examination mean 14 (10-18) years after the index SOLUTION revision operation. There were 15 women/16 hips with a mean age of 78 (74-89) years and 14 men/20 hips with a mean age of 79 (56-91) years. The 18 years cumulative stem survival free of re-revision for any reason was calculated as 94.4% (88.9-99.8%) (Fig. 2). Eighteen years cumulative stem survival, free of re-revision because of aseptic loosening was 97.6% (94.3-100%) (Fig. 3). Stem survival was not influenced by the extent of preoperative bone defects (p = 0.30).
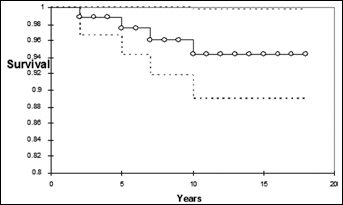
Kaplan Meier plot of cumulative stem survival with end point revision for any reason in 93 Solution stems.
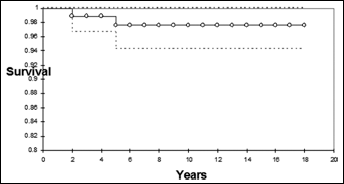
Kaplan Meier plot of cumulative stem survival with end point revision for aseptic loosening in 93 Solution stems.
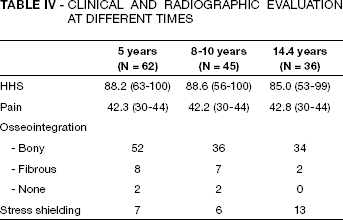
The mean Harris Hip Score was 85 (range 53-99) and the mean pain score 43 (range 30-44). As shown in Table IV, these values hardly differ from the scores at five and 10 years follow-up. According to the Harris Hip Score 24 hips are considered as excellent or good (more than 80 points), seven hips fair (71-80 points) and five hips poor (less than 71 points). Paprosky 3b and 4 hips had no bearing on Harris Hip Score (p = 0.45), but was significantly associated with hip pain (p = 0.024).
-Clinical and Radiographic Evaluation at Different Times
Intraoperative complications at the index SOLUTION operation included 14/93 fractures of the femoral shaft and/or greater trochanter. Ten fractures were treated with cerclage wires, two with a trochanter grip and two did not need osteosynthesis. All fractures healed without further complications. Of 7/14 cases, fractures were in hips undergoing the second revision operation and five of the hips showed Pa-prosky type 3a defects, five type 3b and four hips Paprosky type 4 defects. Nine shaft perforations were bypassed by the revision stem without needing further treatment. Intraoperative fractures and perforations resulted mainly from the instrumentation of the femoral canal by cement removal and to a lesser degree from preparation for and insertion of the revision implant. In eight fracture hips the stem became bony fixated, in five fibrous fixated and one of these stems never showed signs of stable fixation. Six perforation hips became bony ingrown and three stems fibrous fixated. In 10/14 fractures and 7/9 perforations, these were experienced in the first half (47) and 4/14 fractures and 2/9 perforations in the second half (46) of the of the patient cohort (p = 0.015) indicating a distinct learning curve. Perioperative fracture/perforation was significantly associated with pronounced femoral bone defects (p = 0.023).
Postoperative dislocation was experienced in 12/93 hips. Five dislocations were managed by closed - and one by open reduction. Six recurrent dislocations were managed by cup revision in three, liner exchange in one and by neck elongation in two hips. One of the hips treated with neck elongation and the hip treated with liner exchange simultaneously had a distal transfer of the greater trochanter.
Cup re-revision was undertaken in 3/74 hips (4%). Of cups not revised at the index stem revision operation 2/19 (10.5%) were later revised. One cup was revised because of deep infection, three cups because of recurrent dislocation and one cup because of aseptic loosening. One polyethylene liner was exchanged for wear and for recurrent dislocation respectively.
The radiographic evaluation showed calcar rounding off in 14 hips, moderate calcar resorption in four and severe resorption in two hips. Ectopic ossification was noted in 17/36 hips with Brooker grade 4 in four hips. Subsidence of 8 and 10 mm respectively was seen in one Paprosky type 3b and in one type 4 hip, but these stems stabilized with fibrous fixation. Stress shielding was seen in one of 11 hips with a stem diameter less than 15 mm and significant more often (p = 0.03) in hips with a stem diameter of 15 mm or more (12/25). Four hips showed severe stress shielding, all with thick stems (Fig. 4). Osseointegration of the stem was seen in 34/36 hips, showing distinct spot welds on the radiographs (Fig. 5). Two stems showed neither spot welds nor progressive lucent lines and they were assessed as fibrous fixated. No statistical connection between osseointegration and preoperative bone defects were seen (p = 0.58). The incidences of stress shielding and stem fixation at five years, 10 years and at latest follow-up respectively are shown in Table IV. No hips showed progressive lucent lines or lucencies wider than 2 mm, but 10/36 hips had lucent lines in Gruen zone 1, three hips in zone 2, two hips in zone 6 and nine hips showed lucent lines in zone 7 on AP radiographs. There were no distal osteolysis but one hip showed a progressive new osteolytic lesion in the greater trochanter.

Bone fixated stem with pronounced stress-shielding 16 years after the index revision operation.

Osseointegration with spot welds 14 years after the index revision operation.
Discussion
According to the literature an extensively porous-coated stem does fulfill the goals of hip revision surgery by restoring and maintaining long-term mechanical stability (13-16). These qualities are reflected in this study documented by an 18 years cumulative survival free of re-revision for aseptic loosening of 97.6% (94.3-100%), bone ingrowth of 34/36 stems at 10-18 years and osteolysis only in one hip. No other revision stem concept has invariably proved similar long-term durability, but long hydroxyapatite coated stems (17, 18), long uncemented tapered stems (19, 20) and impaction bone grafting with cemented stems (21-23) have shown excellent survivorship. The long-term results using uncemented proximal coated stems are contradictory (24-27). Simple re-cementation still yields inferior long-term results with a continuous increase in re-revisions with time (28-30). This is in contrast with the continuous high stem survival of extensively porous-coated stems for more than 20 years documented by Hamilton et al (15) (and now our study) with no further re-revisions more than 10 years after the index stem revision operation. A study of 4762 revision total hip arthroplasties from the Norwegian Arthroplasty Registry confirms the above-mentioned findings (31).
Paprosky et al (32) experienced a high mechanical failure rate with an extensively porous-coated long stem in femurs with type 3b and type 4 bone defects, why Sporer and Paprosky (33) in these cases recommended the use of a distally based modular tapered stem (19, 24), a long fully hydroxyapatite coated stem (34) or impaction bone grafting with a cemented long stem (22). In contrast we experienced no stem re-revision in 30 Paprosky type 3b and type 4 femurs in our 93 long-term hips. The two subsiding stems were transiently considered as loose but both eventually stabilised as fibrous fixated.
As Garcia-Cimbrelo et al (35) using cemented impaction bone grafting and a standard Exeter stem we also experienced more intraoperative fracture complications and a lower clinical score at follow-up in severe bone deficient femurs but not a higher incidence of stem re-revision.
Fracture of the SOLUTION stem is a quite rare event (14) and associated with poor proximomedial bone support, a small stem diameter, a body mass index greater than 30 and the use of an extended trochanteric osteotomy (36). Our patient with stem fracture was not obese and had no osteotomy, but the stem diameter was 13.5 mm with insufficient proximomedial bone support.
The clinical long-term outcome of our study showed that most patients were satisfied with their revision hip having a Harris Hip Score greater than 80 points and no or only little pain. Even though some authors recommend both subjective and objective scoring systems to evaluate the outcome of hip arthroplasty (37, 38), others have stated that the Harris Hip Score shows high validity and reliability (39) and that an independent surgeons scoring is in excellent concordance with patients self-reported outcome (40). Egan and DiCesare (41) report a high incidence of intra-operative femoral fractures (20%) and perforations (17%) and a significant learning curve using a SOLUTION stem in 135 hip revisions, especially with long/large diameter stems. Also we experienced a significant learning curve and all our fractures/perforations occurred in Paprosky type 3 and 4 femurs indicating that inferior bone quality and bone defects are significant factors. Furthermore, 20 of 23 intraoperative lesions appeared in hips inserted with long stems measuring 15 or more mm in diameter. Like Meek et al (42) intraoperative fractures/perforations had no bearing on stem survival (no re-revisions) or on functional outcome in our patients. Revision with uncemented proximal coated stems (43) and with impaction bone grafting and cement (44) has shown intraoperative fracture/perforation incidences of 40-46%.
Radiographic evaluation at final follow-up showed only few serious or worrisome bone remodelling changes. However, we experienced stress shielding in 13/36 hips but severe only in four hips. As Sköldenberg et al (45) we found stress shielding statistical significant associated with large diameter stems. According to Sychterz et al (46) stress shielding occurs regardless of the implants' level of coating and is predictable for a bone ingrown stem. As Bugbee et al (47) we have never experienced that stress shielding adversely affected the outcome of the revision arthroplasty at minimum 10 years follow-up.
According to Engh et al (9) the presence of spot welds has a high specificity for bony fixation, although the absence of spot welds has a low specificity for unstable fixation. The two hips with no spot welds in our study showed no signs of loosening and were judged fibrous fixated.
Subsidence of more than 5 mm appeared in 2/36 hips, which is considerably less than often experienced with extensively porous-coated stems (32), the Wagner SL stem (19) and with impaction bone grafting and cement (48).
After our first 93 consecutive revision hip arthroplasties with the extensively porous-coated mono block chrome-cobalt SOLUTION stem we conclude, that this stem, in spite of a significant number of intraoperative fractures/perforations, postoperative dislocations and a few number of worrisome radiographic bone remodelling changes, shows a very high long-term survival and an excellent clinical outcome, also in severe bone deficient femurs.