
Abstract
Introduction
Numerous studies on cam femoroacetabular impingement (FAI) causing osteoarthritis have been conducted in Western populations, but not in Asian populations. The alpha angle in cam type FAI can be measured by routine hip AP and axial radiographs. The purpose of this study was to determine the range of alpha angles in an asymptomatic Asian cohort.
Materials and Methods
We performed a retrospective examination on 500 asymptomatic Asian adults (1000 hips) who underwent simultaneous spine MRI and hip coronal survey MRI for evaluation of back pain from December 2009 to March 2010. The alpha angle was measured on anteroposterior (AP) pelvic survey images. According to inclusion criteria, 372 hips of 186 men and 622 hips of 311 women were analysed.
Results
The mean alpha angles for men and women were 50.61° ± 7.61° and 49.82° ± 4.14°, respectively with no statistically significant differences (p = 0.063). Alpha angles of the two age groups (≥50 years old and <50 years old) were similar in both genders: 49.90° ± 6.88° versus 51.40° ± 8.30° in men (p = 0.060), and 50.61° ± 7.61° versus 49.82° ± 4.14° in women (p = 0.71). The frequency of pathologic alpha angle of men and women was 0.5% and 3.1%, respectively.
Conclusions
After review of 994 asymptomatic adult hips, we found neither gender-specific nor age-specific differences in the alpha angle. The frequency of the pathological range of the alpha angle was notably rare, as compared to those of Western countries. We assume that these findings could be related to a low prevalence of FAI and idiopathic osteoarthritis of the hip in the Asian population.
Introduction
Primary osteoarthritis (OA) of the hip is a painful and disabling disease, the end stage of which often requires total hip arthroplasty. Primary hip OA has been found to be associated with various risk factors, including gender, race, obesity, and subtle bony abnormality. Recent improvements in arthroscopic surgery lead to a new prospective in understanding femoroacetabular impingement (FAI) as a causative factor of primary hip OA.
Impingement caused by femoral and acetabular geometric deformity results in labral wear and tear and repetitive microtrauma of osseous structures followed by irreversible articular cartilage damage and resultant OA (1, 2). Ganz et al (3) categorised FAI into two types: a pincer type and a cam type, the so-called pistol grip deformity. The pincer type occurs when there is acetabular over-coverage of the femoral head, and the cam deformity type is when there is an abnormal femoral-neck contour.
Abnormal deformity of the femoral-neck junction can be diagnosed by various imaging modalities, including plain radiographs, computerised tomography and magnetic resonance imaging (MRI). Such deformity is quantifiable by measurement of the alpha angle, as described by Notzli et al (4). In regard to a causal relationship between FAI and hip OA, while Tanzer (5) claimed that all patients with hip OA of unknown cause have the pistol grip deformity, furthermore some have made a counterargument that not all hips with an abnormal alpha angle are symptomatic (6).
While OA is a common disease in Western countries, occurrence of primary hip OA in Asia is relatively rare, even with the rapid Westernisation of lifestyles (7, 8). Numerous studies on cam FAI causing OA have been conducted in Western populations, but not in Asian populations (7, 9, 10). We examined the alpha angle of 994 asymptomatic adult hips on the hip coronal survey view of spine MRI. The primary purpose of our study was to determine the prevalence of cam deformity in a population without hip symptoms. Our secondary aim was to describe the range of alpha angles in an Asian cohort for comparison with Caucasian populations.
Materials and Methods
This study was approved by the Medical Research Ethic Committee of Himchan Hospital, and all participants underwent informed consent. We conducted a retrospective assessment of 500 randomly selected patients (1000 hips) who underwent spine MRI with simultaneous hip coronal survey MRI at our institution for evaluation of lower back pain from December 2009 to March 2010. The following exclusion criteria were applied: suboptimal image quality with an ill-defined femoral head and neck margin, or a history of previous hip surgeries. Although imperfect, dysplastic hips and excessively internally or externally rotated hips were excluded if the obturator foramen index was not within 0.6 to 1.8 on anteroposterior radiographs of the lumbosacral spine, which were also performed with MRI. Applying these criteria, 994 hips were finally included in the study. The MRI was performed on 1.5-T scanners (Magnetom Essenza®; Siemens Korea, Seoul, Korea and Intera®; Philips Korea, Seoul, Korea). The Alpha angle was measured on coronal pelvic survey images taken during spine MRI scanning using methods described by Notzli et al (4). Along with the head contour, the angle was obtained by placing 1) a circle around the spherical contour of the femoral head, 2) a line in the centre of the femoral neck along its longitudinal axis, and 3) a second line that extends from the intersection of the first line and the centre of the femoral head to the point where the osseous anterior femoral head intersects the circle (Fig. 1). Resultant angles were determined using the measurement solutions available in the PACS system (STARPACS®; Infinitt, Seoul, Korea). Independent analysis of all MRI images was performed by two experienced orthopaedic surgeons (WJL and JSP), and the results were derived by consensus. Measurements were performed twice by two observers. To determine interobserver reliability, two experienced clinicians made the measurements and we calculated intraclass correlation coefficients (ICCs) with 95% confidence intervals. The study was designed so that the ICCs could be used to assess reliability.
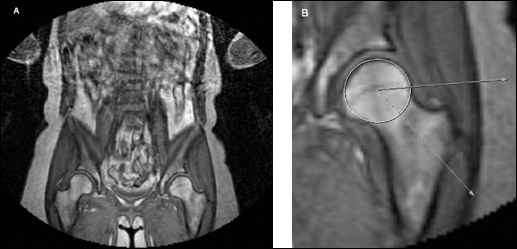
A) T1-weighted coronal survey MRI performed simultaneously with spine MRI. B) Magnified T1-weighted coronal MRI demonstrating the method for measurement of alpha angle. Alpha angle is determined as the angle between a line drawn from the centre of the femoral head through the central axis of the femoral neck and a line drawn from the centre of the femoral head to a lateral point where the femoral head extends beyond the best-fit circle of the head.
We stratified all subjects into three categories according to criteria defined by Gosvig et al, based on the Copenhagen Osteoarthritis Study (9): for men, pathological (≥83° alpha angle), borderline (69°-82° alpha angle), and normal (≤68° alpha angle) and for women, pathological (≥57° alpha angle), borderline (51°-56° alpha angle), and normal (≤50° alpha angle). Cam FAI is a common disorder in young adults. Therefore, all subjects were further classified into two groups according to age: those who were 50 or older and those who were younger than 50 years old.
Statistical analysis
Analysis of alpha angles for gender and age groups was two-tailed, and an independent t-test was used for comparison of the results. Frequencies of pathological, borderline and normal categories for gender and age groups were compared using the Chi-square test. A p-value <0.05 was deemed significant. The inter-class correlation coefficient (ICC) was used to assess alpha angle measurement for intra- and inter-observer variability. The ICC is a test of conformity for measurements made by multiple observers measuring the same quantity in the 0–1 range. An ICC greater than 0.75 indicates excellent agreement between different observations or multiple observers. All statistical analyses were performed using SPSS statistical software version 14.0 (SPSS Inc., Chicago, IL, USA).
Results
Three hundred seventy-two hips of 186 men and 622 hips of 311 women were eligible for this study. The mean age of male participants was 50.02 years old (range 19-96), and that of female participants was 58.19 years old (range 18-86). The ICC varied from 0.81 to 0.85 for intra-observer variability of alpha angle measurements. The ICC for inter-observer variability was 0.67 and 0.90, indicating good to excellent agreement.
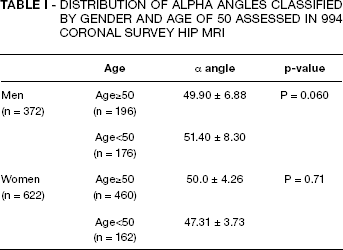
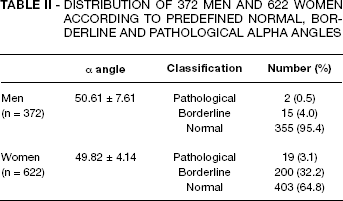
The mean alpha angle was 50.61°±7.61° in men and 49.82° ± 4.14° in women (p = 0.063). Statistically, no gender-specific difference in mean alpha angle was found. The mean alpha angles of both genders classified by age are summarised in Table I. No statistically significant differences were observed between age groups in men and women. The stratified distribution of pathological, borderline, and normal alpha angles is presented in Table II. The frequency of pathologic alpha angle in both men and women was significantly low: 0.5% and 3.1%, respectively. In contrast to previous data in the literature, women showed a significantly higher frequency of pathological and borderline alpha angles than men (p<0.05).
DISTRIBUTION OF ALPHA ANGLES CLASSIFIED BY GENDER AND AGE OF 50 ASSESSED IN 994 CORONAL SURVEY HIP MRI
DISTRIBUTION OF 372 MEN AND 622 WOMEN ACCORDING TO PREDEFINED NORMAL, BORDERLINE AND PATHOLOGICAL ALPHA ANGLES
Discussion
Since the concept of FAI was defined by Ganz et al (3), numerous studies have been conducted (11). However, little is known about the exact aetiology and natural history of progression to primary OA. FAI is a pathological condition in which there is an abutment between the femoral head-neck junction and the rim of the acetabulum. The alpha angle in cam type FAI can be measured not only by routine hip AP and axial radiographs but also using various imaging modalities, including specialised radiographs such as Dune's view, and cross sectional imaging, such as axial oblique MRI. We intended to investigate the prevalence of cam type FAI and alpha angle distribution in the Korean population in comparison with Western populations, using hip MRI coronal views in asymptomatic adults. To the best of our knowledge, this is the first study on the frequency of cam type FAI and the range of alpha angles in a relatively large cohort of asymptomatic adults in Asia and more specifically in Korea. In their study of 2803 AP pelvic radiographs of a Caucasian population in Denmark, Gosvig et al (9) reported a mean alpha angle of 55° in men and 45° in women. In our study, the mean alpha angle of men was 50.6° and that of women was 49.8°. This finding showed a relatively smaller alpha angle in Korean men and larger alpha angle in Korean women as compared to their Caucasian counterparts. While Gosvig's results presented a 10° difference in gender, our results showed no difference in gender.
In our study, the prevalence of cam deformity was found to be 2.1%; 0.5% in men and 3.1% in women in 994 asymptomatic adult hips. While this differs from studies found in Western literature (10, 12, 13) where there is a 15-17% prevalence, it is consistent with Asian studies of rare idiopathic hip OA or FAI, where most hip OA is secondary OA caused by developmental dysplasia or infective arthritis (14, 15). In this study, although the mean alpha angles of men and women were not statistically different, an alpha angle in the pathological or borderline range occurred more frequently in women. This is different from previous studies on the male predominance of the cam type deformity, including that of Gosvig et al (13), with a prevalence of 17% in males and 4% in females. In addition, contrary to the previous belief that cam morphology of the femoral-neck junction is a predisposing factor for premature hip OA in young males, the alpha angle of the two age groups did not show statistical difference in either men or women. Despite an unclear connection, if FAI is, in fact, a primary causal factor for idiopathic hip OA, it is reasonable to assume that the low prevalence of cam type FAI, the lack of difference in alpha angles between different genders and ages, and the relatively small mean alpha angle in men seen in this study could be reasons for the low prevalence of idiopathic OA in the Asian population, more specifically in Koreans. It is important to note that the Copenhagen Osteoarthritis Study (13) showed a significant difference in the prevalence of cam deformity and a sex-related difference in cam malformation, although it used methods similar to ours. Therefore, it is necessary to use different radiologic indices and pathologic cutoff limits for cam type FAI for Koreans and for Asians who are racially and genetically similar.
There are some limitations of this study. Firstly, our measurement of the alpha angle was solely reliant on unstandardised coronal MRI images. Therefore, there may be an argument that coronal images are not suitable for measurement of the alpha angle and that the shape of a cam lesion can change according to the patient's position. According to Gosvig et al (9) AP radiographs can detect most femoral head-neck malformations at an acceptable level, and accuracy increases when measured with a triangular index. In addition, Laborie et al (16) used AP pelvic radiographs to report on the prevalence of the qualitative radiographic findings of FAI on 2081 healthy young adults and Jung et al (17) employed an AP pelvic CT scout view to assess for FAI deformity in the general population in the United States. In the same study, they asserted that there were no visual changes of femoral head-neck contour with excessive rotation, which would produce a false positive cam deformity. However, because the cam deformity is a three-dimensional lesion, it is possible that the alpha angle could have been underestimated by a blind spot of the coronal view or due to hip joint rotation. Secondly, we assumed that not all subjects had symptoms related to a hip problem. This assumption might have affected the study results because the examination by a spine specialist and the MRI scan might not have completely excluded subjects with hip joint problems. Thirdly, although our study involves a relatively large cohort, a large multicentre study is needed in order to apply our study results to the entire population of Korea.
In conclusion, under the conditions and limitations of this study of 994 asymptomatic adult hip joints, the prevalence of cam deformity was very low compared with previous studies of Western populations. Furthermore, the alpha angle did not differ significantly by either gender or age contrary our expectations. We believe that this may be related to the low prevalence and different aspects of FAI in the Asian population, even though our study used a hospital-based cohort. However, whether or not this is related to an overall low prevalence of primary OA of the hip remains to be determined in future studies.