
Abstract
Total hip arthroplasty (THA) after acetabular fracture presents unique challenges, including acetabular fixation. Twelve patients with a history of acetabular fracture underwent THA with porous metal cups. The average age was 57 years (range 24-88). THA was performed at an average 20 months from initial fracture. Average follow-up was 39 months (range 24-49). Average WOMAC scores improved from 32 to 79; UCLA scores improved from 1.75 to 5.25. There was one case of acetabular loosening in a renal transplant patient with rheumatoid arthritis. No other patients showed progressive radiolucent lines. At average three-year follow-up, porous metal components afforded improved clinical and radiographic outcomes in the majority of patients. Longer follow-up will determine whether porous metal is a durable option in the management of prior acetabular fracture.
Introduction
Total hip arthroplasty (THA) for post-traumatic osteoarthri-tis provides satisfactory clinical outcomes (1–4). However, THA after acetabular fracture presents unique challenges to the orthopedic surgeon, including increased operative time, retained hardware, blood loss, and transfusion requirements (5). Of particular importance is adequate fixation of the acetabular component (5).
Romness and Lewallen demonstrated a 52.9% acetabu-lar fixation failure rate from aseptic loosening for a variety of cemented acetabular implants in patients with previous acetabular fractures (6). Weber et al studied 63 patients at a mean follow-up of 9.6 years after THA for post-traumatic arthritis after acetabular fracture (7). Nine acetabular component revisions were performed, all for cemented components (7). Additionally, Weber et al demonstrated that, at ten years, none of the cementless cups in the series were revised (7). Mid-term analyses of aseptic acetabular loosening in uncemented acetabular components for patients who developed post-traumatic arthritis demonstrate satisfactory Harris Hip Score clinical outcomes with 100% survival (8). Bellabarba et al demonstrated a 10-year survival rate of 97% in patients with THA for post-traumatic arthritis secondary to an acetabular fracture, with aseptic loosening on radiographs or revision as the primary end point (9).
While cementless acetabular components have shown promising results for post-traumatic arthritis in patients who have sustained a prior acetabular fracture, it is unknown whether porous metal acetabular components exhibit similar results. The use of porous metals has grown in importance in revision and primary THA, as well as in other areas of reconstructive surgery (10-13). We present here the short-term clinical and radiographic outcomes of porous tantalum cups in the setting of prior acetabular fracture.
Materials and Methods
Twelve consecutive patients who underwent THA following acetabular fracture were included in this study. Porous tantalum acetabular cups (Zimmer, Inc., Warsaw, IN) were used in all patients. There were six males and six females. One patient was a smoker. There was one Worker's Compensation claim at the time of THA; two patients were on disability prior to THA. During this same time period, two patients were treated with standard acetabular shells.
Fixation in the acute period after acetabular fracture was defined as within three weeks from fracture to time of THA, as per the timeframe previously defined by Mears and Velyvis (14). Similarly, subacute arthroplasty was any time between three weeks to three months after fracture; chronic time period was greater than three months from the time of fracture.
Clinical and functional outcomes, including pre- and postoperative Western Ontario and McMaster Universities Arthritis Index (WOMAC) (15) and UCLA Activity (16) scores, were recorded. The need for revision surgery for any reason was a primary clinical endpoint. Estimated blood loss was the assessment of intraoperative blood loss as documented in the anesthesia records for each case. Injury radiographs, pre- and postoperative fracture fixation radiographs, if fixation was performed, were reviewed. Serial radiographs after THA were studied for evidence of femoral or acetabular component loosening and osteolysis according to the method of DeLee and Charnley (17). Radiographs were also reviewed for gross hardware failure and heterotopic ossification (18).
Surgical Tips and Technique
The treating orthopaedic surgeon must be familiar with both internal fixation and revision arthroplasty techniques. Careful assessment of prior hardware, if any, as well as the choice of surgical approach must be determined preoperatively. We utilised an extensile posterolateral approach to the hip in all cases.
Judet views may be obtained to further characterise the bony anatomy. One must consider obtaining preoperative advanced imaging to better define the post-traumatic deformity of the acetabulum. For example, a computed tomography scan with fine cuts, as well as coronal/sagit-tal/ and three-dimensional reconstructions (including formatted images of the acetabulum with the femoral bone subtracted) may aid in the reconstructive planning, and to ensure the integrity of the anterior and posterior acetabular columns. Residual fracture defects and pelvic discontinuity or non-union must be determined.
Preoperative templating is instrumental to guide component sizing, as well as to establish the patient's hip center of rotation. At the time of surgery, intraoperative fluorosco-py may aid in identifying key bony landmarks, which may be difficult to interpret with deformity, scar tissue, or existing heterotopic ossification. All patients had a posterolat-eral approach.
When preparing the socket, complete removal of scar or fibrous tissue must be done to prevent obstruction of the cup/host bone interface. Curette-type instruments, as well as textured surgical sponges (e.g. Ray-Tec, Johnson and Johnson, Inc.) may be used to abrade and remove soft tissues. Hemispherical reaming is performed to establish a bleeding bone bed. Sclerotic areas may be carefully burred. The surgeon must assess bone deficiencies given post-traumatic deformity, and adequate coverage must be maintained. Avoid eccentric or superior reaming within a deformed acetabulum, and preserve the anterior/ posterior acetabular walls as the cup is sequentially expanded with serial reamers. Prior to placement of the real cup, bone grafting with hand-packing and reverse-reaming techniques may be performed to contained defects. Supplemental screw fixation is often utilised in compromised bone to increase initial fixation strength of the construct. Postoperatively, the patient may be kept toe-touch or protected weight-bearing to allow for osseous-integration of the cup.
Results
The average age at THA was 57 years (range 24-88 years). Arthroplasty was performed at an average interval time of 20 months (range 1 week to 156 months) from initial fracture. The median time from time of fracture to THA was 6.5 months. The average postoperative follow-up averaged 39 months (range 24-49 months). The average Body Mass Index was 24 kg/m2 (range, 18-33 kg/m2). Two patients underwent arthroplasty with porous metal cups in the acute time period. Two patients underwent THA in the sub-acute period, and eight underwent THA more than three months from the time of fracture.
Two patients were treated nonoperatively initially. Seven patients were treated with prior open reduction and internal fixation of the acetabular fracture. Three patients were treated with prior THA. One patient had a simultaneous plating/ open reduction of the acetabular fracture and THA. The average operative time for the THA procedure was 145 minutes (range 86-182 minutes), and the average estimated blood loss was 512 mL (range 350-1000 mL). Six patients were bone-grafted at the time of surgery. The in-hospital length of stay was 3.9 days on average (range 3-8 days).
WOMAC scores increased from a preoperative average of 32 to 79 postoperatively (p = 0.02). Similarly, average UCLA scores improved from 1.75 to 5.25 at postoperative follow-up (p = 0.03). There were no revision surgeries in the cohort for aseptic loosening, infection, dislocation or other complications. One patient had a single dislocation event treated with closed reduction. Two patients had 1 cm leg-length discrepancies after arthroplasty surgery.
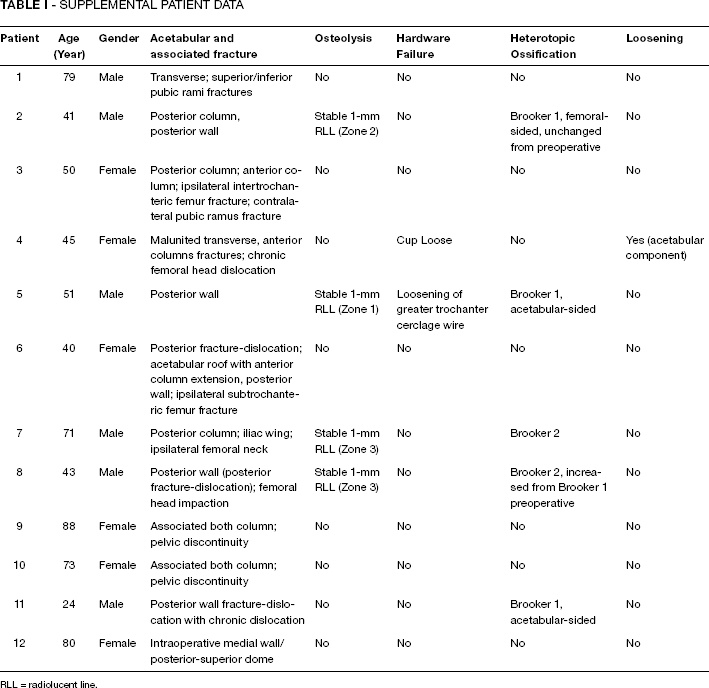
There was one case of radiographic acetabular cup loosening in a patient with a history of renal transplantation and rheumatoid arthritis. The patient denied functional limitation in her activities of daily life and has elected to be followed clinically and radiographically. No other patient demonstrated progressive radiolucent lines about the acetabular components. One patient had evidence of loosening of a greater trochanteric wire without breakage. All other patients demonstrated satisfactory fixation of the porous tantalum cups with osseous integration (Fig. 1). Heterotopic ossification was seen in five patients. Please see Table I for a summary of fracture patterns and radio-logic features of the cohort.
Supplemental Patient Data
RLL = radiolucent line.
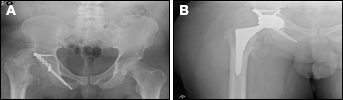
Anteroposterior preoperative
Discussion
Acetabular fixation in the face of significant osteopenia, prior irradiation to the pelvis, and other situations with poor bone quality have traditionally posed a challenge to the ar-throplasty surgeon. Prior acetabular fracture may be also considered in this group of challenging fixation scenarios, given retained hardware, compromised bone stock, and prior surgical interventions. While post-traumatic osteoar-thritis after an acetabular fracture can be effectively treated with THA, previous studies have examined the use of ce-mentless acetabular components but not specifically newer porous metal (tantalum) acetabular components. This study presents a series of porous metal cups with greater than three-year average clinical and radiographic follow-up.
Ranawat et al presented 32 patients treated with unce-mented cups after acetabular fractures (19). Twenty-four patients underwent open reduction and fracture fixation prior to THA, and eight were managed without initial fracture fixation. The revision rate was 19%; one case was for aseptic acetabular loosening (19). Peri-acetabular radiolu-cencies in DeLee and Charnley zones were observed in five patients, with two of these patients exhibiting radiolu-cencies in all three zones. Bellabarba et al studied 30 patients who underwent THA after prior acetabular fracture, comparing outcomes in patients who initially were treated with and without acetabular fracture fixation (9). There was no difference between fracture fixation and non-fixation groups (p = 0.39) (9). Revision for evidence of radiographic aseptic loosening and pain at ten years was 3% (9). Mears and Velyvis assessed 57 acute THA in the setting of displaced acetabular fractures and found that, after two to 12 years of follow-up (14), there were no cases of loosening or osteolysis, and only one case was revised for recurrent dislocations. The authors concluded that THA after acute acetabular trauma can restore function and relieve pain (14). These studies, however, do not examine a consecutive series of patients managed with modern generation porous metal cups as reported in our group of porous tantalum components.
Berry and Halasy reported on 34 uncemented titanium porous-coated THAs after acetabular fracture (20). There were nine aseptic revisions at follow-up of 10 to 16 years. Four of the nine revisions had the shell and polyethylene liner revised: one for loosening, another for loosening and dislocation, and two for osteolysis with well-fixed acetabu-lar components, one of which was associated with instability. The study concludes that uncemented sockets show acceptable aseptic loosening rates (20). While our findings also support the low loosening rates with uncemented ac-etabular cups, it is unclear whether the porous metal cup fixation in our study afforded superior results compared with the porous-coated components studied in prior reports after acetabular fracture.
Porous tantalum acetabular cups offer the potential for improved biologic fixation (13, 21–24). Hacking et al demonstrated that porous tantalum materials provide three to six-fold increased attachment strengths compared to porous beads (24). They demonstrated that porous metal in animal models afforded rapid ingrowth of tissue and vascular structures (24). This may prove important not only in component longevity, but also fixation in compromised bone. Porous metal cups have proved superior to titanium wire mesh cup designs with respect to repeat revision rate due to aseptic loosening (hazard ratio 2.01; 95% confidence interval: 1.44-2.80) (25). The use of tantalum metal as a means of providing secure acetabular cup fixation has been repeatedly demonstrated in the literature (12, 13, 26, 27). Porous tantalum provides an attractive fixation in patients with acetabular bone deficiency or poor bone quality, because of its high surface coefficient of friction and greater degree of osseous integration. Joglekar et al published a minimum five-year follow-up of tantalum acetabular cups for 34 THA after pelvic irradiation in 29 patients (10). There were no revisions for any reason, and there were no clinical or radiographic failures at five years (10).
Furthermore, porous tantalum acetabular cups more closely resemble normal physiological force distribution. This may limit the effects of stress-shielding, provide increased bone mineral density (BMD), and decrease osteolysis (28, 29). Meneghini et al showed that, when peri-acetabular BMD was compared between patients with porous tantalum and titanium cups, there was a statistically significant increase in BMD of 5-40% in the porous tantalum patients in all peri-acetabular regions (28). These findings support the use of porous tantalum implants in patients who are at greater risk of loosening and osteolysis, including post-traumatic bone.
For these reasons, we had transitioned from the use of standard cementless shells to current generation porous metal cups for the theoretical increased ingrowth potential in compromised bone seen after acetabular fracture. The low stiffness, porous tantalum, monoblock implants produce a more physiologic stress response over traditional rigid metal backed acetabular designs. Compared to other cementless designs available, the isoelasticity (modulus between cortical and cancellous bone, is significantly less than other metal alloys such as chromium cobalt) and surface coefficient of friction offer a more biologically active ingrowth material and may maintain bone stock due to decreased stress-shielding. Furthermore, the tantalum nanostructure, while creating an environment more suitable for bone ingrowth, also offers greater resistance to shear stress when compared with conventional implants. Basic science studies, including a THA study in canines, showed accelerated bony in growth, neovascularisation, and increased bone density of porous tantalum when compared with conventional metal cups (22, 24, 30).
For this patient cohort, we used one type of porous metal shell (Trabecular Metal, Zimmer, Inc.) comprised of tantalum. Despite the availability of other porous metal shells, we believe that certain design characteristics of this particular implant offer a superior ingrowth surface in the setting of compromised bone. Unlike other porous metal implants available, the porous tantalum shell is made entirely of trabecular metal. That is, the implant is not simply coated with a porous metal material. Both the porosity, as well as the coefficient of friction unique to porous tantalum in this shell offer initial fixation and theoretical long-term fixation advantages. Moreover, the architecture of the tantalum cup allows for drilling of supplemental screws, if needed, directly through the porous metal material.
While cemented and cementless cups may demonstrate similar results in standard primary THA, accounting for geographic and surgeon-specific training, there are few studies looking at THA after acetabular fracture. No study directly compares cemented versus cementless cup fixation after acetabular fracture in a single cohort. One study examined the use of impaction grafting and cement for fixation after acetabular fracture (31). Twenty hips (20 patients) with a mean age of 53.3 years were reviewed at a mean follow up was 9.5 years. There were two cup revisions: one after 14.5 years for septic loosening, and one after 15.3 years for aseptic loosening. The survival rate of the acetabular component with revision as an end-point was 80% after 15 years. Despite no control group, the use of acetabular impaction grafting and cup cementation in this small series seems a viable option at long term follow-up but is certainly technique dependant.
In the adoption of new technology with potential clinical advantages, the cost of associated technology must be considered. At our institution, there is an approximate 12% cost differential between standard and porous metal shells. It is unclear whether this increased cost at time of implantation may be offset by savings associated with revision-free survival at longer-term follow-up.
Limitations of our study include those related to the retrospective design and small sample size. However, given the smaller number of patients undergoing THA after ac-etabular fracture, this series adds data on porous metal cups to the literature. One patient's scores were excluded from pre/postoperative analysis due to C6-level quadriple-gia secondary to a military training accident. This patient received THA due to recurrent dislocations of his native hip following his accident. These difficulties functionally limited his independence and ability to transfer. With THA he has achieved more independence, improved ability to transfer, and a greater quality of life with no persistent discomfort. Several patients had poly-trauma at the time of their ac-etabular fractures, which ultimately resulted in chronic pain and functional limitations not related to their THA. These injuries may alter the patients' ability to isolate particular limitations on WOMAC scoring related to the THA procedure itself. This also points to the heterogeneity in the patients studied in this type of cohort, given the variety of acetabular fractures, operative fractures fixation methods, and other patient variables. Despite these issues, our results still demonstrate a significant postoperative improvement in WOMAC and UCLA scores after THA in patients with osteoarthritis secondary to acetabular fracture. Finally, there were no direct comparisons to other fixation methods, such as cemented fixation or traditional cementless cups. Strengths of our study include the use of a single porous metal acetabular implant in a single-surgeon series. The specific study of porous metal cups in the setting of prior acetabular fracture has not been reported elsewhere to our knowledge.
In this small patient series at short-term follow-up, porous tantalum acetabular components afforded improved clinical outcomes and satisfactory component longevity in the majority of patients. With longer follow-up and increased patient numbers, porous tantalum may prove a viable option in the management of post-traumatic arthritis in patients with prior acetabular fracture.