
Abstract
The aim of this study was to compare fixation of proximal femoral osteotomies using reverse contralateral LCP-Distal Femoral Plates (LCP-DF) with the more traditional blade plate technique.
This was a retrospective review over six years of a single surgeon's practice within a tertiary orthopaedic unit. Patient demographics were collected, along with indication for surgery. Radiological outcomes, fixation failures and the need for revision surgery were recorded. Forty-six patients were identified; 23 patients in the LCP-DF plate group (7 females, 16 males. Mean age 18.3 years old) and 23 patients in the blade plate group (6 females, 17 males. Mean age 19.1 years old).
The patients’ presenting conditions were; 26 Perthes’; eight hip dysplasia; 11 slipped capital femoral epiphysis; one fibrous dysplasia. Osteotomy type included; 13 Double osteotomy, 11 Imhauser; 13 pure valgus; eight valgus + rotation;
There was one revision for implant failure in the LCP-DF group. In the blade plate group, there were four implant failures – three requiring revision operations (p = 0.155). In the LCP-DF group the mean neck-shaft angle difference compared to the contralateral side (if normal) or 135 degrees (if abnormal) was 0.58°. In the condylar plate group the mean difference was 4.37°.
The use of a contralateral LCP-DF plate in the reverse contralateral position to stabilise proximal femoral osteotomies in our cohort confers advantages over blade plate technology. We have found that the plate is stiffer, is easier to use and provides increased screw placement options over standard proximal femoral locking plates.
Introduction
The use of region-specific locking plates has been recently popularised in the fixation of a variety of fractures. The Locking Compression Plate – Distal Femur (LCP-DF) has been designed to match the contour of the distal femur but has proven use in the non-anatomical ‘reverse’ mode- providing fixation for proximal femoral fractures. It is often used as part of the Less-Invasive Stabilisation System (LISS; Synthes, Stratec Medical Ltd, Mezzovico, Switzerland). Studies have shown satisfactory union rates, avoidance of coxa vara, shorter operation times and improved functional outcome compared to alternative methods of fixation for proximal femoral fractures (1-6). We are not aware of any studies reporting the use of locking plates in areas for which they were not designed, for proximal femoral osteotomies in a young adult or paediatric population.
Operative management of paediatric hip disease aims to restore normal anatomy; maintain joint congruency and optimise hip biomechanics. Depending on the site of the deformity osteotomy of the pelvis and/or of the femur may be required. In the femur, flat plates and blade plates of various angles are available to assist the surgeon in achieving accurate correction of deformity. The purpose of these operations are, in the short-term, improvement in pain and function and in the longer-term to delay the onset of and reduce progression of degenerative change and ultimately to delay arthroplasty.
The purpose of this study was to analyse two cohorts of patients undergoing proximal femoral osteotomy with fixation using either the blade plate or the reverse contralateral LCP-DF. Radiological outcome and the need for further surgery were compared.
Materials and Methods
We reviewed a single surgeon's practice over a six-year period within a tertiary orthopaedic unit. Inclusion criteria were any patient undergoing proximal femoral osteotomy for paediatric hip pathology. Postoperatively, patients were reviewed at six weeks, three months and six months, and then at 3-4 monthly intervals until union and subsequent metalwork removal (which was the study endpoint). Standard orthogonal pelvic and femoral radiographs were taken at these intervals.
Patient demographics were collected using case notes and clinic letters. Plain radiographs were analysed using the Picture Archive and Communication System (PACS). Radiological parameters included neck-shaft angle at union compared to normal side (or 135° if other side deemed to be abnormal), union, metalware failure (fracture or plastic deformation), implant cut-out, or joint penetration.
Failure was defined as non-union, implant penetration, cut-out and excessive shaft medialisation, requiring revision surgery. Delaying progression of osteoarthritis and hip pain was a longer-term concern and hence functional outcome comparison was not assessed between groups.
Data was analysed with SPSS 17.0 using unpaired t-test for parametric data and Chi-squared test for non-parametric data. A p-value <0.05 was deemed to be statistically significant.
Operative technique
Preoperative planning was based on plain radiographs and CT scans to assess the osteotomy type and degree of angular correction needed. For either implant, the patient is placed in the lateral position. A lateral incision is made extending distally from the greater trochanter. A subvastus approach is used for access to the femoral shaft.
Blade plate: A standard blade-plate technique was used with the initial guide wire inserted through the central hole in the three-hole jig at an angle at the side of the femur to provide the desired correction according to the plate type. The remainder of the operation has been described extensively elsewhere and will not be elaborated upon.
LCP-DF: Valgus and Imhauser Osteotomy: The plate with manufacturers black multihole jig attached was laid onto the outside of the (usually) mid-part of the greater trochanter (GT). A left handed distal femoral plate was used on the right proximal femur and vice versa. As the central guide-wire hole subtends an angle of 95 degrees to the five-hole section of the plate, the direction of the guide-wire into the proximal femur was considered similar to the application of a 95-degree blade plate. The expanded seven-hole end of the plate was applied (upside down) to the proximal outer part of the greater trochanter. The LCP-DF was angled outwards from the lateral aspect of the femur (with metal wedges supplied with the angled blade-plate set) to set the required valgus correction. The central hole for the guide-wire on the jig was used to place a wire through the centre of the GT aiming for the inferomedial part of the neck, towards the mid A-P plane of the head under image intensifier (II) control. In performing an Imhauser osteotomy in aiming towards the centre of the displaced head, it was often necessary to swing the plate forwards on trochanter, leaving the plate proud by up to a centimetre at the front. With the guide-wire correctly placed, the plate could then be rotated on it anteriorly, providing any desirable amount of flexion into the osteotomy. Only then was the first of the other proximal holes drilled and the long (usually) 60-70 mm locking screws placed (at this point, further flexion could still be obtained by removing the guide-wire and rotating the plate on the first screw). In the first three cases all the long proximal screws were inserted under direct II control; experience showed that once the guide-wire was in the correct position, the convergence of these screws made this radiation exposure unnecessary. It was not usually possible to find bone for more than five of the seven possible screws through the proximal part of the plate.
The osteotomy was performed ideally just above the lesser trochanter. The remainder of the operation, fixation to the shaft of the femur was completed in the usual way with anterior capsular release in every case and arthrotomy with cam debridement as required. A wedge of bone was removed from the posterior aspect of the proximal fragment and placed in the matching anterior gap at the front of the osteotomy.
In double femoral osteotomy, the LCP-DF was first affixed to the GT with four 22 mm screws, the GT was osteotomised approximately along the line of the trochanteric apophysis; the GT was towed downwards using the plate and then fixed definitively distally and laterally with five or six long screws. The distal osteotomy was then performed obliquely using a reciprocating saw from inferolateral to superomedially exiting just above the lesser trochanter. The lesser-trochanter-shaft fragment was then fixed to the plate, producing the required distalisation and lateralisation.
Results
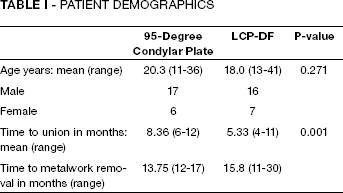
Between May 2006 and January 2008, 23 patients underwent proximal femoral osteotomy using a 95-degree condylar plate or a 130 degree blade plate. Between February 2008 and February 2011, 23 patients had a proximal femoral osteotomy using the LCP-DF. In all cases after osteotomy union, the plate was removed to prevent local pressure symptoms, iliotibial band irritation and make any subsequent femoral surgery easier. The demographics of the patients are shown in Table I. There was no significant difference in age between groups (p = 0.2708). The LCP-DF showed statistically faster time to radiographic union. All patients were ASA 1-2 at the time of surgery.
PATIENT DEMOGRAPHICS
Hip pathology requiring surgery included; Perthes’ disease, slipped upper femoral epiphysis (SUFE), developmental dysplasia of the hip (DDH) and fibrous dysplasia (Fig. 1). Osteotomy type for the different groups is shown in Figure 2.
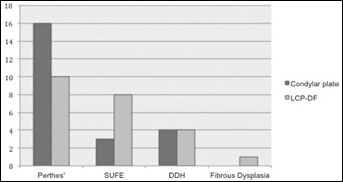
Pathology distribution between groups
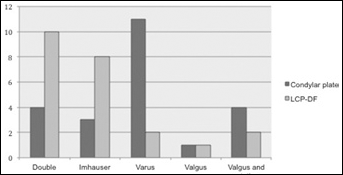
Osteotomy types with the condylar plate and LCP-DF
In the LCP-DF group the mean neck-shaft angle difference compared to the contralateral side (if normal) or 135° (if abnormal) was 0.58° (standard deviation 4.38). In the condylar plate group the mean difference was 4.37° (standard deviation 14.30), p = 0.231.
22 patients in the LCP-DF group progressed to uneventful osteotomy union and plate removal. One patient fractured through the plate and osteotomy site whilst playing rugby, when a scrum (potential weight of 16 players) collapsed on top of his leg four months following his osteotomy. This was subsequently revised to another LCP-DF plate and united uneventfully at 10 months postoperatively.
In the blade plate group, 22 patients eventually progressed to full union. There were a total of four failures.
Patient 1 had an Imhauser osteotomy for SUFE using a condylar plate. She fractured through her plate whilst walking 16 months postoperatively. This was subsequently revised to another condylar plate which united at 14 months following revision surgery. Eighteen months later she required hip resurfacing for significant degenerative changes in the hip joint.
Patient 2 had malunion and excessive medialisation of the shaft following Imhauser osteotomy and was revised to a LCP-DF plate which united fully at eight months postoperatively (Figs. 3a-e).
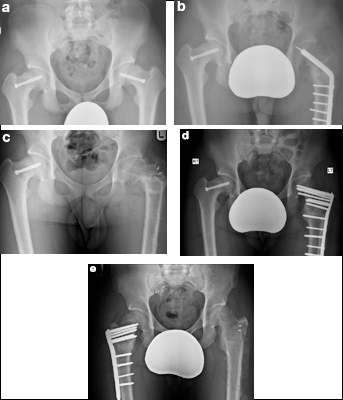
a) Pre-osteotomy x-ray showing bilateral SUFE screws. b) Imhauser osteomy of the left hip using a 130 degree blade plate. Note the broken wire tip in the head of the femur (this was recognised at the time but was not interfering with comfort or function and was removed at the same time as the plate). Note the medialisation of the shaft caused by the inset of the plate below the GT. c) The metalwork has been removed but the neck has malunited in varus. d) The osteotomy has been revised using a reversed contralateral LCP-DF. e) The metalwork has been removed and the neck-shaft angle has been maintained. The patient was satisfied with the outcome and an Imhauser osteotomy with similar fixation has now been performed on the right side.
Patient 3 had Imhauser osteotomy following SUFE and following excessive shaft medialisation was revised to a dynamic hip screw.
Patient 4 had a valgus osteotomy for Perthes’ disease. Malunion resulted and she was revised to an uncemented total hip replacement six years later.
Discussion
Proximal femoral osteotomy for paediatric and young adult hip pathology aims to normalise hip anatomy to optimise function in the short-term and delay the need for arthroplasty. Long-term clinical and radiological results are unknown. We report the first clinical study comparing two different implants for proximal femoral osteotomy until subsequent union and implant removal. The study suggests potential biomechanical advantages of the LCP-DF over the traditional gold standard ‘blade’ technology.
The LCP-DF in the off-label ‘reverse contralateral’ position on the proximal femur showed better maintenance of neck-shaft angle, less malunion and less shaft medialisation. We showed it can lead to a significantly faster time to union. Biomechanical lab studies have analysed different plate designs for simulated subtrochanteric fractures. Forward et al (7) found femoral head cut-out in five of 10 blade plate designs and none in the locking plate group. Floyd et al (8) found proximal femoral locking plates to be significantly stiffer, with less fatigue fractures than blade plates. Crist et al (9) found proximal femoral locking plates to provide more axial stiffness and less plastic deformation than blade plates.
Clinical studies have looked at the use of the reverse LCP-DF for proximal femoral fractures. Zhang (3) reported no incidence of screw cut-out or head penetration and union by 6 months in all patients. Ozkaya (5) reported successful union in all but one patient using reverse LISS, and claimed incorrect positioning at that time of surgery was the cause. Han (2) found more avoidance of coxa vara using the reverse LISS method compared to anti-rotation blades.
Newer proximal femoral locking plate designs have sought to negate problems experienced with blade plates and other proximal femur fixation devices. Several studies have shown a high failure rate in the setting of proximal femoral fracture. Glassner (10) found a higher than expected rate of varus malunion, screw cutout and non-union even in the hands of experienced surgeons. Streubel et al (11) found a 34% failure rate of LCP for subtrochanteric fractures, with varus collapse and screw cut-out being the most frequent mechanism. In a younger cohort of patients, in the setting of osteotomy with improved bone quality, these complications may be less. We found the reversed contralateral LCP-DF gave better screw placement options then some of the newer site-specific proximal femoral designs. We are pleased with the low failure rate, and the ease of use.
In our study, all three patients having an Imhauser osteotomy in the condylar plate group had plate failure requiring revision. In contrast, all eight patients in the LCP-DF group who had an Imhauser osteotomy went on to subsequent union, with no failures. We feel the complex pattern of the osteotomy; flexion, rotation and valgus, may necessitate a stiffer plate.
Our study had several limitations. Although matched for age and ASA there was a difference in hip pathology between groups. There were more Perthes’ patients in the blade plate group and less SUFE compared to the LCP-DF group. Osteotomy type varied as a result. Most failures were in the Imhauser group. A higher number of Imhauser's in the blade group may have led to further failures. The LCP-DF cohort were performed after the blade plate cohort. Whilst this might suggest a femoral osteotomy learning curve effect, in practice, we have used blade plates in a variety of ways since 1990 and we doubt if this accounts for the difference in outcome. As our purpose was to look at the stability of the osteotomy and the speed of union, functional scoring was not performed and a comparison might have been misleading due to the different pathologies treated.
Our study shows biomechanical advantages of the LCP-DF in the reversed contralateral position as compared with blade plate technology. It is stiffer – and may be more resistant to axial and torsional load. There is less risk of cortical penetration and guide-wire breakage as compared to the condylar blade design. We feel it is easier to use, has greater reproducibility and therefore confers advantage to comparable implants in the setting of highly complex multi-planar osteotomies.