
Abstract
Introduction
Acetabular component position can be an important determinant of joint stability and bearing surface wear after THA. Nonetheless, the incidence of malpositioning is high. Patient obesity, low surgeon volume, and minimally invasive approaches are known risk factors for malposition. As the incidence of obesity continues to increase, it is important to recognise its effect on intraoperative component positioning in THA.
Objectives
Our goal was to assess the impact of obesity on component position for a high-volume surgeon using a standard postero-lateral approach.
Methods
A consecutive series of 120 obese (BMI >30, mean BMI 34.4) and 120 non-obese patients (mean BMI 25.4), who had undergone primary THA by a single surgeon, were included in our retrospective study. AP pelvis and cross-table radiographs obtained at the first postoperative visit were analysed using EBRA software to determine inclination and anteversion angles. Optimal position was defined as 30-45° of inclination and 5-25° of anteversion.
Results
Mean inclination and anteversion were 40.6 (+/-5.4°) and 16.6 (+/-5.5°) respectively, in the obese group and 39° (+/-5.0°) and 16.2° (+/-7.5°) in the non-obese group. In the obese group 89 (74%) patients were within the desired range for both measurements, 31 (26%) were out of range in at least one, compared to 91 (76%) and 29 (24%) in the non-obese group, respectively. The overall incidence of malpositioning was 25% for both groups. Among outliers, mean deviation from the optimal range was ≤3.8° in both groups.
Conclusions
The risk of component malpositioning in THA may be reduced when surgery is performed by an experienced, high volume surgeon utilising a standard posterolateral approach. In this setting the deleterious effect of obesity may be overcome.
Introduction
Acetabular component malpositioning represents an important modifiable risk factor for postoperative instability, bearing surface wear, and component impingement in total hip arthroplasty (THA) (1-2-3-4-5). Placement of the cup within the parameters of the “safe zone” is recommended to optimise implant stability and wear (1-2-3-4-5). Historically Lewinnek et al defined the safe zone as 15 +/- 10° anteversion and 40 +/- 10° inclination based on their retrospective case series (1). More recently, with increased understanding of the impact of edge loading on bearing surface wear, others have defined the safe zone as 5-25° of anteversion and 30-45° of inclination (6). While the exact definition of the safe zone and its relationship to the native hip anatomy have been debated, the concept remains an important principle in guiding surgical technique for THA (7).
In spite of a growing recognition of the importance of cup position, a number of studies have noted relatively poor accuracy of manual component positioning. Padgett et al noted wide variability in component inclination (23-57°) when using a manual positioning device (8). Similarly, a recent large registry study from a major academic center noted malpositioning in one or both planes in 50% of patients (6). Risk factors identified for malpositioning include low surgeon volume, minimally invasive approach, and patient obesity (6). Of these factors, only patient obesity is outside of the control of the operating surgeon.
The impact of obesity represents a growing public health concern. In 1997, the adult-obesity prevalence in the United States (US) was 19.4% (9). Currently 35.7% of adults are obese, and it is estimated that by 2030, 51% of the adult US population will be obese (9, 10). Obesity has been associated with a number of adverse events surrounding total hip replacement including increased risk of infection, thromboembolic disease, dislocation, early revision, and component malpositioning (11). Furthermore, increased body mass index (BMI) has been associated with an increasing risk of fixation failure in uncemented acetabular components (12). Indeed some have suggested bariatric surgery should precede elective joint replacement surgery to reduce the risk of complications and increase longevity (13). As the incidence of obesity continues to increase, it is important to recognise its effect on intraoperative component positioning in THA and identify means to optimise positioning in obese patients.
Regression analysis from Callanan et al suggests that risk of malpositioning may be reduced by a high volume surgeon using a posterolateral approach (6). Our objective was to characterise the impact of obesity on component positioning at our centre when surgery is performed by an experienced, high-volume surgeon using a standard posterolateral approach.
MATERIALS AND METHODS
Patients undergoing primary THA by our senior surgeon between August 2010 and August 2011 were eligible for inclusion in this retrospective case-control study. Study design was reviewed and approved by our Institutional Review board. Patients were classified according to criteria of the World Health Organization, with BMI ≥30 defined as obese; accordingly two consecutive cohorts were identified, 120 obese and 120 non-obese patients.
Patient characteristics including age, gender, BMI, diagnosis, and range of motion were determined from the medical record. Cup and femoral head sizes were recorded and utilised for image analysis. In addition, any dislocations requiring reduction were noted.
All surgeries were performed by our senior surgeon, who is an experienced, hip arthroplasty surgeon with a surgical volume greater than 350 THAs per year, using a posterolateral approach, supported by an experienced surgical team. A number of techniques were utilised to optimise accuracy in component positioning and reduce the impact of patient body habitus. Firstly, care was taken to ensure secure fixation of the pelvis to the operating room table with anterior and posterior supports centered on the pubis and sacrum so as to minimise motion of the pelvis intraoperatively. Secondly, length of incision varied from four to six inches according to patient body habitus with longer incisions utilised for visualisation in patients with increased muscle mass and/or adipose tissue. Thirdly, cups were inserted utilising a curved (offset) impactor. The curved impactor, as opposed to the conventional straight impactor, minimises impingement of the instrument with the proximal femur, soft tissue envelope, and distal portion of the incision during cup insertion. Finally, cups were inserted using a free hand technique after preoperative templating as described by our senior authors (14). Careful attention to bony landmarks and the preoperative template were routinely observed. All cups were uncemented (Trilogy, Zimmer, Warsaw, IN). Ancillary screw fixation was used rarely, at the discretion of the surgeon.
Standardised anteroposterior (AP) pelvic radiographs obtained at the first, six week, postoperative visit were analysed, using Ein-Bild-Roentgen-Analyse (EBRA-Cup®) hip analysis software, to determine cup inclination and anteversion angles (Fig. 1). After marking several points on the outer margin of the acetabular component, EBRA-Cup® creates an ellipse with a centre that overlaps the centre of rotation. Component version is calculated through ellipse geometry. The software does not distinguish between anteversion and retroversion. Therefore, the direction of version was confirmed with standard cross-table lateral radiographs (Fig. 2) (6, 15). The use of this method allows for assessment of component position using standard postoperative radiographs. While CT scan and cross-table lateral alone have been previously utilised to measure anteversion, the cost and radiation associated with CT is prohibitive and accuracy of cross-table lateral imaging is dependent on patient positioning (15). The accuracy of this software has been previously documented (16). Similar techniques for assessment of component position have been reported in a number of recent studies (6, 17, 18). Optimal position was defined as 30-45° of inclination and 5-25° of anteversion as described by Callanan et al (6). All radiographic measurements were performed by an independent observer, who was not involved in the patient's care.
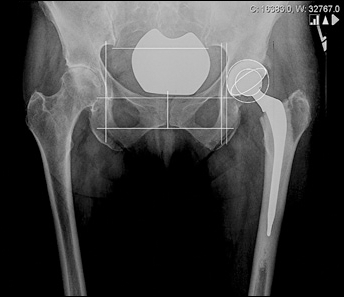
(EBRA-Cup®) hip analysis software utilises ellipse geometry to determine cup inclination and version angles.

Standard cross-table lateral radiographs are utilised to determine direction of version, distinguishing anteversion from retroversion.
Outliers were defined as patients with one or both measurements outside of the target range and deviation from the target range was quantified. Chi squared tests were used to compare the number of outliers in each group and a logistic regression analysis was used to evaluate the impact of the studied variables on component positioning. Age, gender, diagnosis, laterality, and ROM were compared between the two groups. Significance was set at p<0.05.
Results
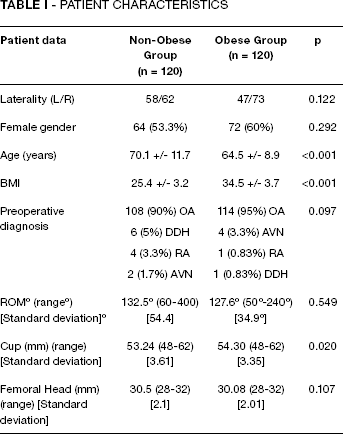
Obese patients were significantly younger than non-obese patients, mean age 64.5 as compared to 70.1 (p<0.001). Cup diameter was greater in the obese group, mean 54.3 mm as compared to 53.2 mm (p = 0.02). The remaining variables were similar between the groups (Tab. I). Mean component position was similar for the two groups. The mean inclination (+/- standard deviation) was 40.6° +/- 5.4° (range 27.2-55.4°) and 39 +/- 5° (range 27.8-53.1°) respectively for obese and non-obese patients (p = 0.02). Mean anteversion (+/- standard deviation) was 16.6° +/- 5.5° (range 5.2-31.6°) and 16.2° +/- 7.5° (range 3-41°) respectively for obese and non-obese patients (p = 0.51).
PATIENT CHARACTERISTICS
There was a similar number of outliers in the obese and non-obese THA groups, 31 (25.8%) and 29 (24.2%), respectively, (p = 0.766) (Tab. II). Obese outliers were more likely to present with increased inclination and normal version, whereas non-obese outliers more frequently presented with excessive inclination and version (Fig. 3). Gender, age, and ROM were not significantly different between obese and non-obese outliers (Tab. III). Regression analysis revealed no significant association between BMI and component position. Among the outliers, mean deviation from optimal range was ≤3.8° in both groups.
OUTLIER PATIENTS: CHARACTERISTICS
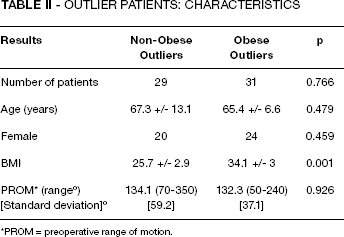
PROM = preoperative range of motion.
OUTLIERS VS. NON-OUTLIERS

ROM = range of motion.
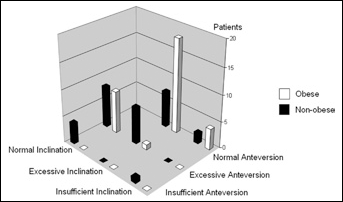
Graphical representation of version and inclination range for obese and non-obese cohorts.
Female gender was significantly over-represented among the outliers. Eighty-nine (74%) female patients had the acetabular cup within the desired range, while 44 females were outliers (p<0.001) (Tab. III). At the one-year follow-up, no patient had dislocated.
Discussion
The risks associated with acetabular components oriented outside of the “safe zone” include instability (2, 19, 20), impingement (19, 21, 22), liner fracture, dislodgement (23), and wear (4, 5, 21). Both surgeon-related and patient-related factors have been identified as risk factors for cup mal-orientation (6, 24). The factors include free-hand cup positioning (24), minimally invasive surgical approach, low surgeon volume, and obesity (6). It has been shown that cup mal-orientation is seen in up to 55% of obese patients undergoing THA (6).
Patients in the obese group were significantly younger than non-obese patients, a finding consistent with the literature (25, 26). Mean inclination and anteversion angles for either obese or non-obese patients fell in the “safe zone” defined as 30-45° of inclination and 5-25° of anteversion. Obese patients had mean inclination and anteversion angles of 40.6° and 16.6°, respectively. These values are comparable to those reported by Callanan et al for their 2061 patients, namely 42.2° of inclination and 12.7° of anteversion (6), a study which included patients operated through different approaches and by several surgeons (high and low volume). In our study, 75% of all cups were placed within the desired range, comparing favorably to the highest rate of optimally placed cups (70.5%) reported in the literature (24). Callanan et al reported that 50% of cups implanted in their cohort were outside the desired range (6). Based on their regression analysis the authors concluded that elevated BMI represented a risk factor for mal-orientation, but also noted that the risk of malpositioning was less when surgery was performed by a high volume surgeon using a posterolateral approach.
Barrack et al similarly reported on 1549 THA and resurfacings performed at their institution and assessed component position by similar methods (17). They noted 93% of components met their target for inclination, 95% for anteverision, and 88% for both, however, the target zone for THA was defined as 30-55° for inclination and 5-35° for anteversion, a significantly wider range than that utilised by Callanan et al and the present study. Their findings with regards to surgeon volume echoed those of Callanan et al with low volume surgeons 2.16 times more likely to miss the target zone. Interestingly, they noted a linear increase in component malpositioning with increasing weight, such that the odds of missing the target increased by 0.2 for every 5 kg/m2 increase in body mass index.
Our findings support the conclusion of Callanan et al, that component positioning can be optimised by a high-volume surgeon using a posterolateral approach. In our study, obesity did not represent a risk factor for component malorientation, with the combined percentage of outliers from both cohorts being 25%. In contrast, Elson et al recently assessed the impact of morbid obesity on acetabular component position and noted an increased incidence of malpositioning in the morbidly obese group, as defined by a BMI >35. Patients were derived from a registry and were heterogeneous with regards to surgical approach as well as surgeon volume. Since it has been previously shown, by Callanan et al, that surgeon volume and posterolateral approach reduce the risk of malpositioning, and since the difficulties encountered in the obese patient would be magnified in the morbidly obese patient, it is not surprising that our findings differ from those of Elson et al (18).
The lack of a relationship between obesity and cup mal-orientation has been suggested by other authors (24, 27-29). Bosker et al reported on a smaller number of THAs, which were performed by 12 attendings and residents, through anterolateral and posterolateral approaches, with either cemented or uncemented fixation (24). Pirard et al conducted a retrospective study on 323 THAs but evaluated anteversion only (28). Todkar et al evaluated 111 THAs performed through the anterolateral approach (29). The present study is the largest comparing both inclination and anteversion angles of cups positioned free-hand by a single surgeon using a posterolateral approach.
Our study (Fig. 3) showed that obese outliers often had excessive inclination but normal anteversion, whereas non-obese outliers were more likely to present with both excessive inclination and anteversion. Abundant soft tissue in obese patients might prevent placing the cup in the desired inclination, particularly if straight cup holders are used.
In the present study females were found to be significantly over-represented in the outliers group compared to the non-outliers (p<0.001) (Tab. III). Females are at a greater risk of dislocation than males (30); accordingly, our senior author takes care to ensure sufficient anteversion to improve posterior stability, aiming for anteversion closer to 25°. Callanan et al (6) and Bosker et al (24) did not find any significant association between gender and acetabular component malorientation.
Our study has limitations. Firstly, we categorised patients on the basis of BMI alone. While proximal thigh circumference might have provided a clearer indication of the difficulty of exposure, we do not routinely measure this. This may represent an area for future investigation. Secondly, our study was not powered to detect a difference of 7% as described by Callanan et al, which would have required over 1600 patients. This is because our goal was not to disprove that obesity is a risk factor for malpositioning but rather to assess the degree to which obesity affected component positioning in our cohorts. Thirdly, all surgeries were performed by the same high-volume surgeon with over 40 years of experience, supported by a likewise experienced surgical team, which may not accurately reflect surgeon characteristics at other practices or institutions. While this certainly reduces the generalisability of our findings, it also makes an important point that the technical challenges of component positioning in obese patients can be well managed by an experienced surgeon. A number of recent studies, which have assessed the impact of obesity on component positioning have noted the impact of surgeon volume on component positioning as well (6, 17). Low surgeon volume has repeatedly been cited as a risk factor for malpositioning and it is intuitive that the risk of malpositioning would be greater in more difficult cases such as the high BMI patient.
In conclusion, when performed by an experienced high volume surgeon, through a standard posterolateral approach, the risk of component malorientation in THA may be significantly reduced compared to recently reported rates. Our senior author has found that the above noted techniques have yielded equivalent accuracy in obese and non-obese patients. Based on our findings, we believe obese patients seeking THA for severe hip pathology should consider seeking out an experienced high volume surgeon, supported by a likewise experienced surgical team.
Footnotes
ACKNOWLEDGEMENTS
We are grateful to Dr Amar Ranawat and Mr Matin Lendhey for their assistance in utilising the EBRA-Cup® software.