
Abstract
We present the clinical and radiological results of a prospective study of a consecutive series of patients treated with the Birmingham Hip Resurfacing (BHR) prosthesis between 1999 and 2006 and followed for six to 12 years.
Patients were reviewed preoperatively and six, 12, 26 and 52 weeks postoperatively and annually thereafter. They were assessed clinically and radiographically and the Merle d'Aubigne Postel and Oxford Hip scores were calculated at each visit. A SF-36 form assessed general health. Patient satisfaction was assessed by a Visual Analogue Score. Kaplan Meier survival analysis was performed.
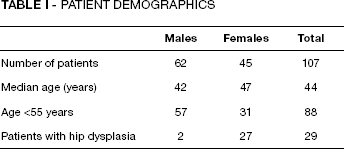
One hundred and seven patients (109 hips) were included (45 males, 62 females). Median age was 44 years. Mean follow-up was 97.4 months. Median preoperative Merle d'Aubigne Postel and Oxford hip scores were 10 (3-14) and 42 (26-55) respectively. Median SF36 score was 29 (0-65) and patients rated their level of pain as 7.7 on a scale of 0-10 (10 being the worst score).
At final follow-up, median MDP and OHS scores were 17 (16-18) and 25 (12-46). Median SF36 score was 72 (27-97).
Seven revisions were performed in six females and one male patient. Survival was 96.2% with revision for any reason as the end point. No revisions were performed in the group with hip dysplasia.
The BHR prosthesis provides pain relief, high levels of patient satisfaction and improvement of function and well being in the medium-term. Failures occurred primarily in the female group.
Introduction
Modern metal-on-metal hip resurfacing arthroplasty (MoM HRA) was developed in the United Kingdom in the early 1990s to specifically address the issue of wear and early failure encountered with conventional total hip arthroplasty (THA) in the active population. This prosthesis was promoted specifically for active individuals who wished to maintain normal activity levels after surgery (1). Traditional THA with metal-on-polyethylene bearing couples have demonstrated the least satisfactory results in this group due to increased wear and early failure as a result of osteolysis (2). Proposed benefits MoM HRA included improved stability (3), better wear characteristics and preservation of femoral bone stock. This led to enthusiastic use by surgeons as well as a proliferation of designs by several manufacturing companies, each with its own proposed benefits. Six different designs were in common use by the by the time of publication of the first report of the UK National Joint Registry in 2004 (4). The most popular device used in the UK has been the Birmingham Hip Resurfacing arthroplasty (BHR, Smith and Nephew, UK).
The early enthusiasm displayed was tempered by reports of early complications including femoral neck fractures (5) along with a spectrum of soft tissue pathology thought to result from a localised adverse reaction to metal debris (ARMD) (6). This has led to a general reversal of the initial enthusiasm shown for the use of MoM HRA (4).
In the face of this good clinical scores and activity levels have been reported in the medium term for the Birmingham Hip Resurfacing arthroplasty by several authors including designer surgeons (7) and specialist academic centres (8).
The aim of this study is to present the levels of patient satisfaction, clinical and radiological results as well as improvement in quality of life associated with metal on metal hip resurfacing arthroplasty using the BHR device at a district general hospital at six to 12 years post surgery.
PATIENTS AND METHODS
This prospective study was performed between 1999 and 2006. All patients having this procedure in our unit were enrolled in this study. The study was discussed with each patient and informed consent was obtained in all cases. We also obtained permission from patients to contact them by telephone if they were unable to attend our outpatient follow up clinics. An a priori power analysis with a statistical power of 0.8 and a probability of 0.05 revealed that 102 patients were required for the study.
One hundred and nine MoM HRA procedures using the BHR prosthesis were performed in 107 consecutive patients (62 females and 45 males) (Tab. I). Osteoarthritis was the primary diagnosis in 73 cases (66.4%). Twenty-nine patients in this cohort (29 hips) (26.6%) had osteoarthritis secondary to Crowe Type 1 hip dysplasia. The average age of this group was 36.4 years (range 23-53 years). It included two males and 27 females.
PATIENT DEMOGRAPHICS
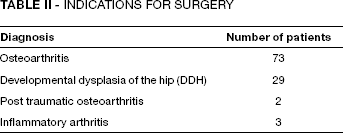
Indications for surgery are presented in Table II. Patients were offered this procedure if they were active, fit and wished to return to sport after their surgical procedure. Patients who had known metal sensitivity, renal impairment, poor proximal femoral bone stock as well as post menopausal females with osteopaenia or osteoporosis (based on dual energy x-ray absorptiometry (DEXA) scans) were excluded (Fig. 1). Forty-six females of childbearing age specifically requested hip resurfacing arthroplasty as their treatment of choice for their symptoms. Their decisions were made based on their desire to maintain a high level of sporting activity post surgery.
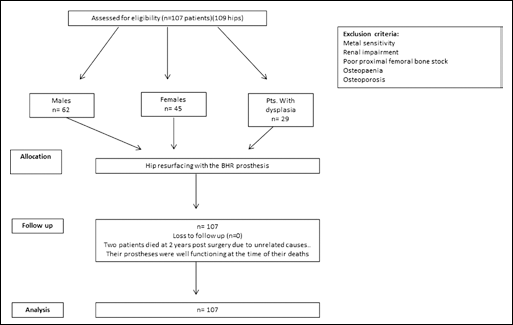
CONSORT flowchart.
INDICATIONS FOR SURGERY
All procedures were performed by a single surgeon (HDA) via a posterior approach. The short external rotators were routinely re-attached using sutures placed via drill holes along the posterior border of the greater trochanter. All patients were allowed to fully weight bear from day one post surgery – initially with a zimmer frame or two sticks. They progressed to one stick as confidence improved and were required to be able to climb stairs (if they performed this at home) with minimal discomfort prior to discharge. Sporting activities were discouraged for the initial three months postoperative period.
Preoperatively the Oxford Hip score (OHS) was calculated for each patient. Levels of pain, function and mobility were assessed using the Merle D'Aubigne Postel (MDP) score. Quality of life (QOL) scores were recorded using the short form 36 (SF36) questionnaire. A separate visual analogue scale (VAS) was used to assess levels of pain where 10 indicated significant symptoms and an unhappy patient and 0 represented a happy patient who was symptom free. These scores were also calculated when patients were followed at six weeks, three months, six months and annually thereafter.
In addition, at each postoperative review, patients were specifically asked if they were satisfied (with responses being not satisfied, partially satisfied and wholly satisfied) and the extent to which they felt they had been made better after their procedure (wholly better, moderately better, no better or worse off). Two patients moved out of the area at four and five years and did not wish to attend follow-up clinic but we were able to consult them by telephone and obtain OHS as well as SF 36, VAS and satisfaction scores.
Data distribution was assessed using the Kolmogorov-Smirnov test. Statistical analysis was performed using the Mann Whitney test. The level of significance was set as p = 0.05. Survival was calculated using the Kaplan Meier Method (Graph Pad software, CA, USA) (Figs. 2 and 3).
At each visit anteroposterior radiographs of the pelvis and lateral views of the operated hip were obtained. These were assessed by two separate reviewers for signs of loosening according to the criteria of Amstutz et al (9) for the femoral component. Acetabular loosening was classified according to the zones of Charnley and DeLee (10). Acetabular abduction angle was calculated using the method described by Hing et al (11).
Results
The median age of our cohort was 44 years (range 21-65 years). Average duration of follow-up was 8.2 years (range 5-12 years). Two patients died at two years postoperatively from unrelated causes with their prostheses intact and normal levels of function. Median femoral component size was 46 millimetres (mm) (range 46-59 mm).
Median preoperative MDP scores were 2 (range 0-4), 4 (range 0-6) and 5 (range 0-6) for pain, mobility and function respectively. Pre-operative SF-36, OHS and VAS scores were 29 (range 0-65), 42 (range 26-55) and 9 (range 4-10) respectively. At final follow-up median MDP scores were 5 (range 5-6), 6, 5 (range 5-6), for pain, mobility and function respectively (p = 0.00012). Median SF 36 score was 75 (range 27-97) (p = 0.048) and OHS 25 (range 12-46) (p = 0.005). The median VAS score improved to 1 (Tab. III). Survival of this prosthesis was 96.2% at an average eight-year follow-up (95% CI 90.9-99%) with revision for any reason as the end point (Fig. 2). At final follow-up two patients (1.9 %) reported being only partly satisfied. They were not sure that they had much improvement after their procedure. One hundred and five patients (98.1%) were highly satisfied (Fig. 4). Four patients reported that their operated hips felt only moderately better while 103 patients (96.3%) reported being wholly better (Fig. 5). Similar levels of improvement in functional and satisfaction scores were reported by male and female patients.
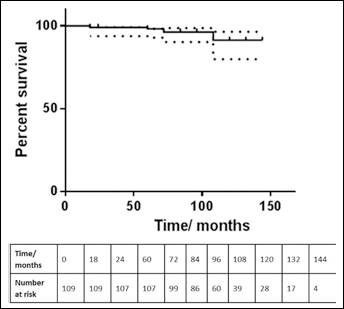
Kaplan Meier survival plot and life table for our entire cohort.
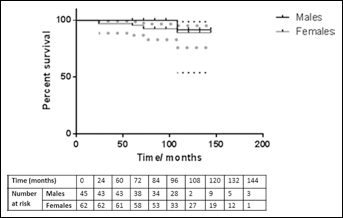
Kaplan Meier survival plot and life table for male and female patients.
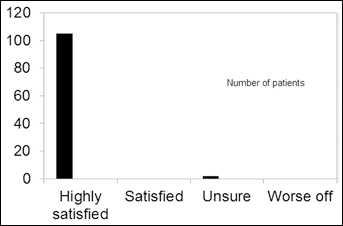
Patient satisfaction at final follow-up.
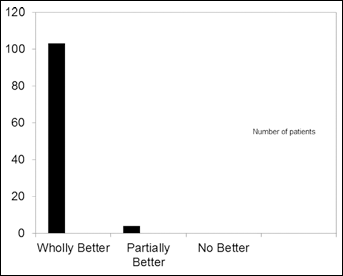
Patient reported improvement at final follow-up.
CLINICAL RESULTS AND PATIENT SATISFACTION SCORES
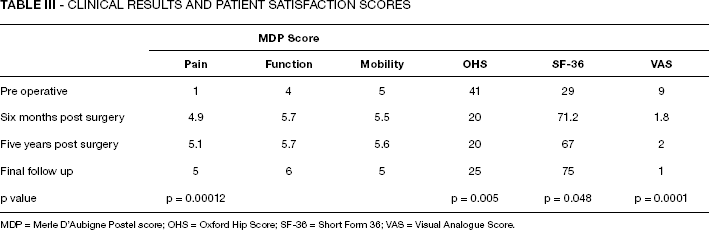
MDP = Merle D'Aubigne Postel score; OHS = Oxford Hip Score; SF-36 = Short Form 36; VAS = Visual Analogue Score.
Median abduction angle was 44 degrees (range 31-56°). No radiolucent lines (RLLs) were noted in any unrevised femoral or acetabular component up to the time of last follow-up. Of those which were revised, incomplete RLLs were noted in zones 1-3 (Amstutz score 7) in our patients. Signs of acetabular loosening were found in zones 1 and 2 in one patient. These findings were noted at two years. This patient was symptomatic hence her hip was revised.
REVISIONS
Seven revisions were peformed in six female and one male patient (Tab. IV). Three revisions were performed due to progressive pain secondary to aseptic lympoctic vasculitis associated lesion (ALVAL) at five years (two cases) and nine years (one case) post-op.
DETAILS OF PATIENTS WHO UNDERWENT REVISION SURGERY
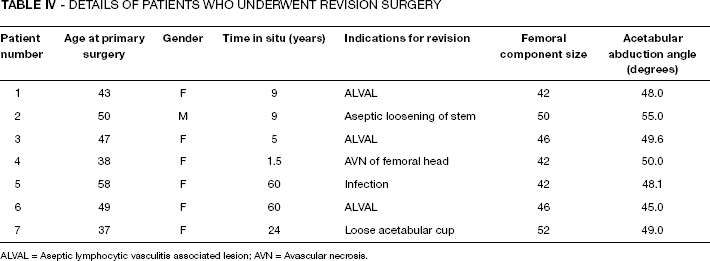
ALVAL = Aseptic lymphocytic vasculitis associated lesion; AVN = Avascular necrosis.
The earliest revision was performed at 18 months in a female patient. The cause was found to be avascular necrosis of the femoral head under the femoral component. Two cases of aseptic loosening occurred at two years and nine years. One patient developed a deep infection at five years and underwent revision to a conventional THA with ceramic on ceramic bearings. There were no impending revisions to the time of last follow-up. Median acetabular abduction angle in this group was 50 degrees (range 45.0-55.0°).
Complications
Notching the inferior border of the femoral neck occurred in one patient. This was managed with non-weightbearing mobilisation for six weeks postoperatively. This patient has had no clinical complaints. No femoral neck fractures, dislocations or symptomatic venous thromboembolism were encountered.
Discussion
The patient population presented in this study is younger than the national average for patients being treated with hip resurfacing arthroplasty in the United Kingdom (4). A larger number of female patients were treated with this procedure during the study period. Females of child bearing age were not offered this procedure routinely. Forty-six female patients specifically requested this procedure. They were counselled about the little understood effects of MoMHR on pregnancy and the developing foetus and well as the predictably successful results of conventional primary total hip arthroplasty and allowed to make an informed decision. Two have since had successful, full term pregnancies with no complications thought to be related to their HR prostheses. Postmenopausal female patients as well as those with inflammatory arthritis underwent dual energy x-ray absorptiometry (DEXA) scans of their proximal femur to confirm adequate bone stock prior to having this procedure.
The majority of encouraging results for hip resurfacing arthroplasty have emerged from high volume specialist units (1, 12, 13). Relatively little is known about medium to long-term results from general hospitals. This cohort consists of the surgeon's entire patient population treated with hip resurfacing, including his learning curve. The single case of notching of the inferior border of the femoral neck occurred within the first 50 cases. The overall survival of the BHR prosthesis our cohort at a mean of eight years was 96.2% (95% CI 90.8-100%) and 91% at 10 years (95% CI 65-96.8%). These results meet the criteria for acceptable implant performance set by the UK Orthopaedic Data Evaluation Panel (ODEP). They have been achieved in a younger than average cohort. They are comparable to results in older patient groups at a similar duration of follow-up (8). Pain, function and mobility and their overall quality of life were significantly improved in this group of patients as a result of having this procedure.
The size of the femoral component has been proposed to be more predictive of failure than gender (8, 14). As a result caution has been advised with the use of femoral components with a diameter of less than 42 mm (15). One patient in our study had a 38 mm femoral component inserted. She has exhibited no symptoms of ARMD to the time of her last follow-up and continues to be followed up closely. Six of our seven revisions (85.7%) were performed in female patients. This is in keeping with previous reports of higher failure rates in females (7). Survival at an average of eight years was 100% in the male group and 90.9% in the female cohort (Fig. 3). Mean femoral component diameter in the revised group was 46 mm (42-52 mm) compared to 48 mm (range 38-60 mm) for the entire group. Although our study consists of a relatively small cohort, these results suggest that it is possible that female gender does contribute to failure, although the reason for this is not fully understood. This finding is consistent with those of other authors (8).
Significant improvements in pain, function and quality of life were achieved with this procedure. Patients were able to return to their desired activities by six months post surgery. This correlated with the majority who continued to feel fully satisfied and wholly better up to the time of final follow-up. The four patients who felt only moderately better also reported being satisfied. Closer questioning revealed that they had higher expectations about returning to impact sport, including marathon running and kite surfing. They had no impairment of normal daily or normal exercise related activities and their preoperative pain had resolved. Inflammatory markers and metal ion levels were normal in this group. Two patients were only partially satisfied due to stiffness of their operated hips. They had no pain or restriction of daily activities.
Enquiring about satisfaction levels, VAS scores and asking patients subjectively how well they thought their joint was performing have been found to be very useful in our unit. Asking about simple outcomes such as satisfaction and how much better they thought they were after surgery not only allowed patients to simplify their responses as but also enabled us to get an accurate overall impression about the effect of this prosthesis on each patient's lifestyle. It was found to be a useful adjunct to the MDP and OHS questionnaires. Four revisions were performed on the basis of sudden deterioration of function and increasing pain but with no significant radiological findings. In each case changes in the VAS score and satisfaction levels preceded the increase in pain. During revision surgery both the acetabular and femoral components were removed and replaced with conventional stemmed THA prostheses using ceramic on ceramic articulations instead of retaining the socket and using a large diameter metal on metal stemmed THA. This was done to avoid potential complications associated with this group of THAs (8, 15).
At the time of revision no destructive soft tissue lesions or effusions were noted. These patients have all experienced resolution of the symptoms which they experienced prior to revision. We believe this was at least in part due to having a low threshold for early revision of painful, poorly functioning prostheses, which minimised the amount of potential soft tissue injury, in agreement with previously published findings (15). At each procedure tissue samples were sent for histopathological analysis as well as culture and sensitivity. The diagnosis of ALVAL which was made in three patients was made on the basis of histological analysis.
Suboptimal clinical outcomes and higher revision rates have been reported in patients with hip dysplasia who are treated with hip resurfacing arthroplasty (16, 20). Gross and Liu attributed higher failure rates in female patients specifically to hip dysplasia. Twenty-nine patients (27 females, two males) presented with osteoarthritis secondary to Crowe type 1 dysplasia. The average age for this group was 36.4 years (range 23-53 years). The mean femoral head size was 45 mm (range 40-54 mm). This group reported significant improvements in the MDP, VAS, SF-36 and OHS scores. One patient has reported pain in her resurfaced hip which started during her third trimester of pregnancy. No effusion has been found on ultrasound examination and she continues to be followed up closely. A definitive decision regarding revision will be made after she has given birth.
Results from this cohort contrast with previous reports of revision rates of 6% to 8% in patients with osteoarthritis due to dysplasia who are treated with hip resurfacing arthroplasty (17, 18). It must be stated that the BHR prosthesis was not used in these studies. Recent clinical results of the BHR used in the management of patients with dysplastic hips have been similar to our findings but at a shorter period of follow-up (19, 20).
This study is limited by the relatively short follow-up period.
In conclusion these results suggest that the BHR device provides excellent relief of symptoms and is associated with high levels of satisfaction in the hands of non-designer surgeons at the medium term. Failure rates do seem to be higher in female patients. An unexpected but encouraging finding was that patients with primary hip dysplasia can experience excellent levels of symptomatic relief, return to function and low revision rates in the medium-term with this prosthesis.