
Abstract
In total hip replacement surgeons can choose from a various number of approaches, from posterior, lateral or direct anterior. Excellent results can be achieved with all approaches and there is no evidence for the use of a specific approach. Minimally invasive operating techniques might further contribute to that success. Early rehabilitation and functional outcome can be improved by the introduction of evidence based clinical pathways irrespective to the used approach.
Introduction
It is well established that total hip replacement is one of the most frequent and most successful operations in orthopaedic surgery. Thus the reliability of the procedure is of major socio-economic importance. The operation should be effective in terms of pain relief and should come along with a preferably short hospital stay and fast recovery. The overall function of the hip and patient satisfaction should be high, aiming for a high percentage of patients with a “forgotten joint replacement” as soon as possible (1).
Posterior, lateral and direct anterior approaches are established for total hip replacement (Fig. 1). The operations can be performed in supine or in lateral position on standard or on trauma tables. More recently minimal invasive operating techniques (MIS) have been developed for all possible approaches in assumption that muscular damage is reduced and postoperative recovery is thus facilitated (Tab. I). The various different approaches and their variants which surgeons can choose from raises the question which is most appropriate for total hip replacement.
THE MOST FREQUENTLY USED APPROACHES IN HIP REPLACEMENT
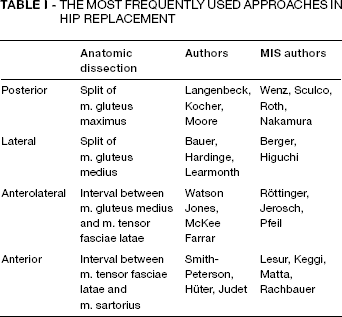
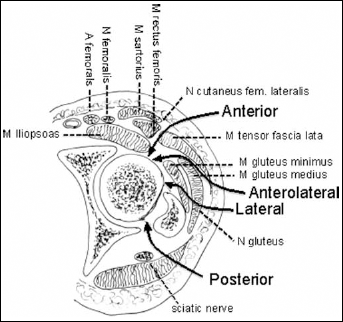
The posterior, lateral, anterolateral and anterior approach. Each approach has specific muscle groups that have to be mobilised and for each approach specific neurovascular structures are at risk.
APPROACHES
Posterior approach
The patient has to be placed in a lateral position (2). The m. gluteus maximus is bluntly split and the short external rotators need to be detached to get access to the femoral joint capsule. The surgeon needs to be aware of the location of the sciatic nerve. Refixation of the short external rotators after implant placement reduces the risk of dislocation.
Using the posterior approach makes it more difficult to control implant orientation and perioperative radiographic examination in lateral position is less feasible as compared to operations in supine position. However, the abductor and flexor muscles are not touched.
The posterior approach can be extended both for exposure of the acetabulum and the femur and thus is suitable for most indications in primary and revision hip arthroplasty.
Lateral and anterolateral approach
The patient can be placed in a lateral or in a supine position. Various techniques are described to elevate the muscular bridge of the ventral portion of the gluteal muscles and the m. vastus lateralis (3). In the anterolateral approach the m. vastus lateralis, in some variants, does not need to be detached (4). The lateral and the anterolateral approaches, with their variants, are often used synonymously.
The sciatic nerve can be irritated by retractors when elevating the femur, thus caution needs to be taken. Furthermore, the femoral nerve and the femoral vessels are at risk by retractors placed on the anterior rim of the acetabulum (5) and extensive splitting of the m. gluteus medius can damage the superior gluteal nerve (6). In the supine position implant orientation might be better reproducible and the use of the intensifier is facilitated. As a part of the abductor muscles is detached and the femoral reamers have to pass and thus might damage the insertion of the m. gluteus medius, it might be difficult to achieve early weight bearing.
The lateral approach can be extended and gives good exposure to both the acetabulum and femur, thus being suitable for primary and revision operations.
Anterior approach
The direct anterior approach has been well established for arthrotomies and periacetabular osteotomies (7) and recently has become more popular in hip replacement. The patient is placed in supine position on a standard table or on a fracture table (8). M. Sartorius, m. rectus femoris and m. iliopsoas on one side and m. tensor fasciae latae on the other side are mobilised and held back by retractors. The femoral nerve and vessels are at risk if retractors are placed on the anterior rim of the acetabulum and the lateral branches of the femoral nerve are at risk when using caudal retractors. During preparation and reaming parts of the m. tensor fasciae latae might be damaged.
The exposure of the acetabulum is good and it can be extended for acetabuar revisions but the posterior column can not be reconstructed. The femoral preparation is more difficult and femoral revisions with osteotomies can not be performed using this approach.
Comparison of the various approaches
Hip replacement is a successful procedure proven for all approaches but there are some specific differences (Tab. II). The dislocation rate might be higher for the posterior approach (9, 10) however, the risk of dislocation is multifactorial and thus the used approach is only one of many aspects (11).
POTENTIAL ADVANTAGES (+) AND DISADVANTAGES (-) OF THE DESCRIBED APPROACHES
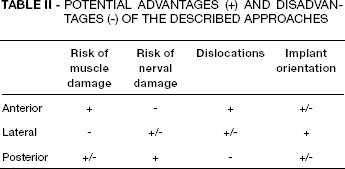
In the lateral approach the splitting of the m. gluteus medius might damage the superior gluteal nerve (6) and fatty degeneration of the m. gluteus medius and minimus have been shown in MRI studies but long lasting functional deficits are rarely found (12). The posterior approach gives less damage of the abductor muscles as compared to the lateral approach however a functional difference is not proven in clinical trials (13).
In the anterior approach the n. cutaneous femoris lateralis is at risk and numbness of the anterolateral tight might occur. However, performing a more lateral and distal skin incision of the tensor fascia might reduce this problem (14). To access the hip joint capsule using the anterior approach a real intermuscular and interneural plane is passed, thus the muscular damage is reduced as shown in MRI studies and with muscle damage markers (12, 15). Using the anterior approach facilitates early mobilisation and reduces hospital stay compared to the posterior approach (16), but a long-lasting functional benefit is not proven.
As the direct anterior approach only recently has been popularised for hip replacement there is a lack of studies with larger patient populations and with long-term results.
Minimal invasive hip replacement
There are many studies comparing standard and MIS procedures with posterior, lateral and anterior approaches. They have shown that according to MRI images there is less muscle damage (12) and a lower increase in markers for muscle necrosis and inflammation (15) as compared to standard procedures. Several studies have shown that MIS is accompanied by improved early function and facilitated rehabilitation (17). This might affect the length of hospital stay and time of recovery. In the mid- and long-term no functional advantages have been shown when using MIS compared to standard approaches (18, 19).
Curved instruments and short stems have been developed to facilitate preparation and implantation which might contribute to the reduction of complications (20).
However, there is a risk that the quality of cementing and primary fixation of uncemented implants is affected by MIS approaches and it is not yet established that the long-term fixation is not compromised by the use of MIS techniques and implants.
Increasing knowledge in anatomy and blood supply of the hip has contributed to reduce the surgical trauma in all approaches and there is a lack of definition of what is considered a MIS hip replacement. The length of skin incision is mainly cosmetic but might lead to a psychological bias. However, the aim of MIS should be a muscle preserving procedure although even so called standard procedures can be done carefully without considerable traumatisation of the soft tissue.
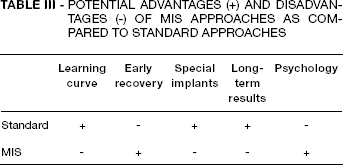
A multimodal and interdisciplinary pathway for joint replacement including anaesthesia, pain and blood management, a better awareness of the psychology of the patient and subspecialisation leading to a higher case load have contributed to enhanced early recovery and better outcome, independent from the used approach (21). A longer lasting effect of MIS procedures could not be proven yet but as standard hip replacement already shows good results there is a ceiling effect when assessing the outcome with classical instruments (1) and more detailed analysis is necessary (Tab. III).
POTENTIAL ADVANTAGES (+) AND DISADVANTAGES (-) OF MIS APPROACHES AS COMPARED TO STANDARD APPROACHES
Using a new approach
Each approach is accompanied by a learning curve and case-load might affect the complication rate. Sticking to one specific approach leads to a higher experience what means knowing the anatomical aspects in detail, introducing muscle sparing techniques, optimising surgical instruments and avoiding specific complications.
The introduction of a new approach has a learning curve for all people involved in the process. Intraoperatively there might be more complications like nerve damage, periprosthetic fractures, dislocations and infections. Problems in implant positioning, orientation and fixation can compromise long-term outcome. A change of the approach used as standard also means a change of the postoperative care, especially in the prevention of dislocations.
The introduction of a minimal invasive approach might be even more complex and have a flatter learning curve since it is technically more difficult and can lead to more complications (22). Intraoperative views are more limited thus new didactic tools like cadaver workshops, practice on plastic bones and visitations would be useful. But the introduction of MIS techniques can facilitated to do changes in peri- and postoperative care and help to introduce new concepts like enhanced recovery.