
Abstract
In this update we searched the literature about the outcome of the lateral versus posterior approach in hip arthoplasty for osteoarthritis (OA) and femoral neck fracture (FNF) patients. The available evidence shows that the use of posterior approach in OA patients is associated with lower mortality and better functional outcome while the use of lateral approach in FNF patients gives lower dislocation rate. We recommend therefore the use of posterior approach in OA patients and lateral approach in FNF patients.
Introduction
The choice of surgical approach in hip arthroplasty for osteoarthritis (OA) or femoral neck fracture (FNF) patients is a crucial part of preoperative planning. Frequently considered aspects are soft-tissue sparing, accessibility to the proximal femur and acetabulum, prosthetic stability and postoperative pain and function. However, the surgeon's preference, usually based on previous experience, remains the main factor in making the final choice.
In clinical practice, there are three common approaches to hip arthroplasty, anterior, lateral and posterior. However, several modifications (and therefore new names) have been made to these approaches creating a great amount of confusion in analysing their reported suitability and safety. Furthermore, minimally invasive (MIS) modalities of these approaches have also been described with even more technical variability.
In the anterior approach (also known as direct anterior), the interval between the sartorius muscle and tensor facia lata is used to access the anterior joint capsule. The lateral approach (LA) has two main types, the anterolateral and direct lateral. The former uses the interval between the tensor facia lata and the anterior margin of the gluteus medius muscle while the latter includes either osteotomy of the greater trochanter or tenotomy of a variable length of the gluteus medius muscle attachment to the greater trochanter to access the anterior joint capsule. Some authors use the term modified anterolateral when the surgical dissection includes the release of the distal part of the gluteus medius tendon from the greater trochanter. In both anterolateral and direct lateral, supine or lateral decubitus positions can be used. The posterior approach (PA) (also known as posterolateral) comprises blunt dissection of the gluteus maximus muscle fibres followed by tenotomy of the hip short external rotator muscles with or without tenotomy of the periformis muscle to access the posterior joint capsule. In this approach, the patient lies in the lateral decubitus position.
The rate of use of different approaches varies among countries (1). However, the LA and PA are by far the commonest two alternatives in clinical practice both for OA and FNF patients (1-2-3-4). In this update, we aim to discuss the available evidence about the advantages and disadvantages of these two approaches.
OUTCOME OF LA VERSUS PA IN OA PATIENTS
Several authors have reported the results of hip arthroplasty for OA patients using LA or PA, either separately or in comparison to each other. Outcome variables like functional results, quality of life and postoperative complications were evaluated. However, most of these reports included small samples and were therefore of limited value.
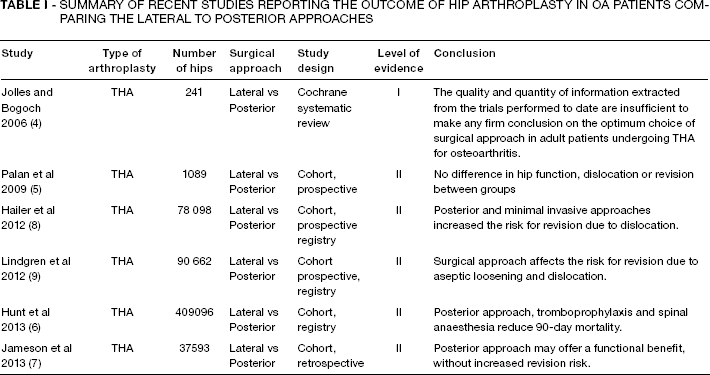
Table I presents a number of important papers that report the results of large samples of prospectively collected outcomes. Jolles and Bogoch (4) and Palan et al (5) found no significant differences in functional outcome or postoperative complications (nerve injury, leg-length discrepancy and prosthetic dislocation) between the two approaches. Hunt et al (6) and Jameson et al (7) in their separate analyses of the linked national databases of England and Wales respectively reported a lower 90-day mortality and a slightly higher functional outcome with PA. On the other hand, Hailer et al (8) and Lindgren et al (9) studied the Swedish hip arthroplasty registry and respectively found that PA gave a higher risk of revision due to dislocation and a lower risk of revision due to aseptic loosening.
SUMMARY OF RECENT STUDIES REPORTING THE OUTCOME OF HIP ARTHROPLASTY IN OA PATIENTS COMPARING THE LATERAL TO POSTERIOR APPROACHES
The introduction of MIS techniques has not significantly improved the results of hip arthroplasty over the standard approaches. In a recent meta-analysis (10), only a few advantages were demonstrated in MIS patients, these being shorter operative time and hospital stay.
OUTCOME OF LA VERSUS PA IN FNF PATIENTS
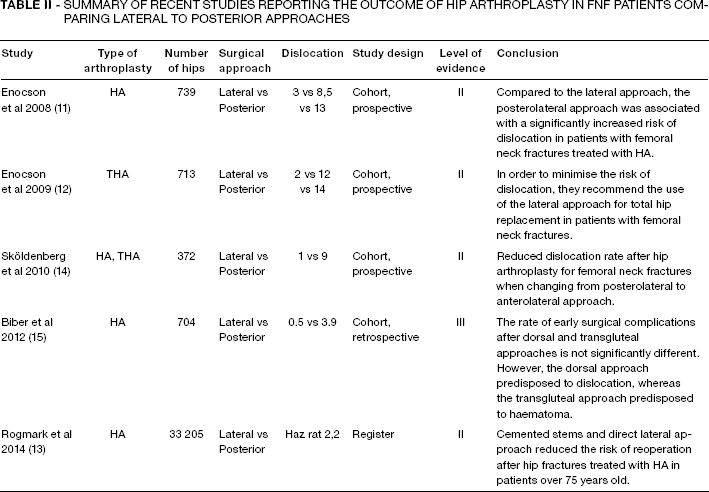
The surgical approaches in hip arthroplasty for FNF patients have gained importance in recent years. Table II summarises the findings of some important recent papers in this field. Enocson et al showed in their prospective comparative non-randomised studies (11, 12) that PA was the only risk factor for increased dislocation of both hemiarthroplasty (HA) and total hip arthroplasty (THA). These results agree with the findings of Rogmark et al (13) who analysed the Swedish hip arthroplasty registry. Sköldenberg et al (14) reduced their rate of dislocation from 9% to 1% by changing the routine at their department from PA to LA in managing FNF patients with HA and THA. Biber et al (15) showed higher dislocation rate but less haematoma formation after the PA while the overall complication rate was comparable between the two approaches.
SUMMARY OF RECENT STUDIES REPORTING THE OUTCOME OF HIP ARTHROPLASTY IN FNF PATIENTS COMPARING LATERAL TO POSTERIOR APPROACHES
Discussion
This update shows that it is still unclear which surgical approach is superior in hip arthroplasty. The hip arthroplasty registries from the Scandinavian countries show obvious discrepancies in the rate of use of different approaches. In Sweden for instance, PA is used in more than half of patients, whereas in Denmark it is used in 90% and in Norway in 25% of patients (3).
In OA patients, LA seems to give a higher 90-day mortality and slightly lower functional outcome and satisfaction than PA. This is probably due to postoperative pain, lateral hip tenderness and limping associated with the gluteus medius tenotomy. Furthermore, LA increases the revision risk secondary to aseptic loosening. One predisposing factor for this increase might be the possible varus positioning of cemented stems inserted in what is known as the C-position using this approach (Fig. 1). Another factor could be the improper entry point to the femoral canal with subsequent choice of a smaller stem size that loosens earlier. On the other hand, PA is found to increase the risk of revision secondary to dislocation probably because the exposure and positioning of the cup is more difficult resulting in an increased risk for retroversion and subsequent posterior dislocation (Fig. 2). The repair of posterior capsule and tendons and the use of a head size >28 mm can however give extra stability and is generally advocated by surgeons using this approach.

Lateral view of a THA inserted using the lateral approach. Note the C-position of the stem where the stem tip attaches to the posterolateral cortex of the femoral canal.

Lateral view of a THA inserted using the posterior approach. Note the 10° retroversion of the cup. This patient had recurrent dislocation.
The failure of MIS approaches in improving outcome could be due to limited role of soft tissue sparing in certain MIS variations especially if it is only confined to the skin and subcutaneous incisions. Also technical difficulties encountered with these surgeries can lead to malpositioning of the prosthetic components and increased risk of perioperative complications.
Patients treated with an arthroplasty for FNF represent a different group with a different rate of complications. The LA is well documented to give better prosthetic stability compared to the posterior approach. This difference is probably related to the mechanism of dislocation in the two approaches. In LA, the dislocation takes place with excessive extension and external rotation and the patient does not easily achieve this position. In comparison in PA the dislocation usually occurs with increased flexion and internal rotation associated with sitting or leaning forward. The FNF patients are generally older and weaker than OA patients and many of them have altered mental status. At the same time, the prefracture hip range of motion is well preserved compared to OA patients where the arthritic hip changes give limited motion. This combination makes the risk for dislocation higher in FNF patients. Therefore prosthetic stability is an important requirement to reduce the need for revision surgery in this fragile group of patients. Sköldenberg et al (14) successively reduced the dislocation rate in their department by changing the approach from PA to LA. Two surgeons taught their colleagues over a period of one year and the rate of complications during the learning curve period was not increased. A possible option to decrease the risk of dislocation is the use of a dual mobility cup especially in younger and more active patients whom would suffer more from complications such as postoperative limp and trochanteric tenderness. In this case, PA might be used to optimise the functional outcome together with a stable prosthetic design. However, the functional outcome and quality of life in FNF patients and in relation to the surgical approach has not been adequately studied in the literature and further evaluation of this is required.