
Abstract
Osteonecrosis of the femoral head is a pathologic condition that commonly affects young patients and requires treatment with total hip arthroplasty (THA). The most common factors associated with osteonecrosis in young patients have not been previously described in the literature. A retrospective study was conducted to describe the most common factors associated with osteonecrosis in patients aged 35 or younger requiring a primary THA. This study included 235 patients and found that the most common factor associated with osteonecrosis was corticosteroid use (61%), followed by idiopathic causes (11%), trauma (9%), other causes (8%), haemoglobinopathies (7%), and alcoholism (3%). There was no significant difference in age between risk groups (p-value = 0.35), however there were significant differences in sex (p-value = 0.02) and unilateral versus bilateral surgery (p-value<0.01). Several factors are associated with the development of osteonecrosis of the femoral head in young patients, and these factors should be given consideration in determining disease aetiology and counselling patients.
Introduction
Osteonecrosis or avascular necrosis of the femoral head is a pathologic entity that can be progressively debilitating and may eventually lead to destruction of the hip joint (1). In the literature, it is also commonly known as AVN, aseptic necrosis, and ischaemic necrosis, and it typically affects patients between the ages of 20 and 50 with a mean age of 38 at presentation (1). The prevalence of osteonecrosis is not known, however the incidence is estimated to be between 10,000 to 20,000 cases per year in the United States (2). In the majority of cases, the diagnosis of osteonecrosis is made at an advanced stage of disease, when non-operative treatments may not be indicated and where total hip arthroplasty (THA) is the most appropriate treatment option (1, 3). In fact, approximately 10% of all THAs are performed for the underlying diagnosis of osteonecrosis (4).
The aetiology of osteonecrosis can be divided into traumatic and atraumatic causes (1). Traumatic causes of osteonecrosis such as femoral neck fracture have been studied and shown to be related to interruption of the vascular supply of the femoral head. More specifically, the blood supply to the femoral head is derived from a vascular tree with limited collateral circulation. As a result, mechanical disruption of this blood supply leads to necrosis of the marrow, medullary bone, or cortex (4).
The mechanism of atraumatic osteonecrosis is not as clearly understood, but is most likely related to direct damage to osteocytes or dysfunction in blood flow leading to cellular necrosis and subsequent collapse of the femoral head (1). Atraumatic osteonecrosis has been associated with corticosteroid use, alcoholism, and systemic medical conditions such as thrombophilia, sickle cell disease, type I Gaucher's disease, caisson disease, and systemic lupus erythematosus (SLE). In young patients, Legg-Calvé-Perthes disease (LCPD) and slipped capital femoral epiphysis (SCFE) are also important causes of atraumatic osteonecrosis (1).
More recently, genetic predisposition has been suggested as a significant contributor in the development of osteonecrosis (5). A recent study showed that patients with decreased activity of a certain ctyochrome p450 enzyme have an increased risk of corticosteroid-associated osteonecrosis (6). Given the numerous associated factors that have been identified and the potential for overlapping factors, the development of osteonecrosis is now considered by some to be a multifactorial process (1). Despite these associated factors, approximately 10 to 20% of osteonecrosis cases do not have any identifiable risk factors and are therefore considered to be idiopathic in nature (1).
Even though osteonecrosis commonly occurs in younger patients at an advanced stage of disease requiring treatment with THA, there have been no studies to our knowledge focusing on the causes of osteonecrosis in this select population. As a result, in this study, we will describe the most common factors associated with osteonecrosis of the femoral head in patients aged 35 or younger, who underwent a primary THA at our institution. We will also describe any differences in patient demographics and the need for unilateral versus bilateral THA between osteonecrosis risk groups. We hypothesise that corticosteroid use will be the most common factor associated with osteonecrosis in this population, and there will be significant differences in patient characteristics between risk groups.
Methods and patient characteristics
Study design
This retrospective study was conducted at a major tertiary academic medical centre. This study was approved by the institution's IRB and all authors vouch for the accuracy of the reported data and analyses.
In order to identify patients with osteonecrosis, we first conducted a chart review of all patients aged 35 or younger, who underwent a primary THA at our institution between 1982 and 2011. These patients were identified from a hospital-based registry, and subsequently, each chart was reviewed in a chronological manner. The data gathered included demographic information, primary diagnosis or indication for surgery, surgical information, past medical history, implant information, and revision information (if applicable). This dataset was sorted by primary diagnosis that was listed in the pre-operative history and physical or operative note.
All patients with a primary diagnosis of osteonecrosis were identified and further subdivided into categories based on common factors associated with osteonecrosis. These common factors were determined after reviewing the first 300 patient charts and included the following: trauma; corticosteroid use; alcoholism; haemoglobinopathies (sickle cell disease or thalassaemia); other (genetic diseases or systemic conditions), and idiopathic. Risk factors for osteonecrosis were listed in several areas of a patient's chart including the pre-operative history and physical, operative note, and past medical history. For consistency, each patient contributed only 1 risk factor to our analysis. If multiple risk factors were listed in the patient's chart, the strongest risk factor was determined by the authors and included in the analysis. For example, if a patient had SLE and was treated with corticosteroids, he or she was listed under the “corticosteroid use” category, since corticosteroid use is an independent and consistent risk factor for osteonecrosis in patients with SLE (7, 8). We also identified the most common reasons for corticosteroid use, as well as the most common haemoglobinopathies and “other” diseases by reviewing each patient's past medical history.
Lastly, we conducted a sub-analysis to determine any differences in sex and age between the 6 osteonecrosis risk groups. The patient's sex and age at time of surgery were determined by chart review. We also compared the number of patients with unilateral THA and bilateral THA in the osteonecrosis risk groups in order to determine any significant differences. Patients undergoing one-stage and two-stage procedures were included, and information regarding lateralisation was available by chart review.
In this study, patients with a history of LCPD and SCFE were excluded, since these conditions have other associated long-term sequelae in addition to osteonecrosis, such as degenerative arthritis, that require treatment with THA (9). Our overall study design is shown in Figure 1.
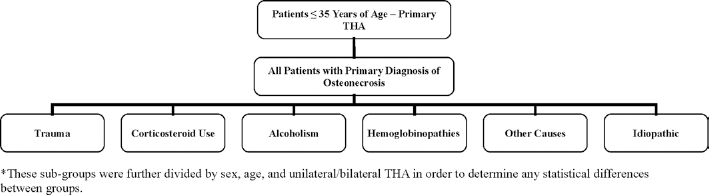
Overall study design.
Statistical analysis
Descriptive statistics were used to summarise disease information (primary diagnosis, osteonecrosis risk groups), patient characteristics (age, sex), and surgical details (time of surgery, laterality). Means and standard deviations were calculated for continuous variables such as age, while frequency and percentages were reported for categorical variables. Comparisons of categorical variables between the 6 common osteonecrosis factors were performed using the Chi-square or the Fisher exact test, and the association of age and osteonecrosis factors was evaluated using ANOVA. Post-hoc pair-wise comparisons were carried out on variables that were found to be significantly associated with osteonecrosis factors in the omnibus test. The comparisons were made correcting for multiple comparisons using the FDR method. All tests were two-sided with significance level of 0.05. All analyses were conducted using SAS for Windows 9.2 (SAS Institute Inc., Cary, NC, USA).
Results
Patient characteristics and dataset
In total, 711 patients aged 35 or younger underwent a primary THA at our institution between 1982 and 2011. Out of these patients, 235 patients (33%) had a primary diagnosis of osteonecrosis, and all THAs for osteonecrosis were performed between 1985 and 2010. In the osteonecrosis subset, 124 patients were male (52.8%) and 111 patients were female (47.2%). The mean age at the time of surgery was 27.5 (SD: 4.9 years) and the median age was 28 (Range: 13-35). In all, 107 patients underwent bilateral THA and 128 patients underwent unilateral THA for osteonecrosis, resulting in a total of 342 THAs.
Common factors associated with osteonecrosis
The most common factor associated with osteonecrosis in our population was corticosteroid use. In fact, 144 patients (61.3%) had a documented history of significant corticosteroid use in their medical record that was thought to be related to the development of their osteonecrosis. The most common reasons for corticosteroid use were SLE (31.7%), malignancy such as lymphoma (15.9%), organ and bone marrow transplantation (13.1%), and respiratory illnesses such as severe asthma (12.4%). Other less common causes for corticosteroid use included neurological disease (multiple sclerosis, optic neuritis, and encephalitis), rheumatologic disease (rheumatoid arthritis, vasculitis, sarcoidosis, and Lyme disease), gastrointestinal disease (Crohn's disease), endocrine disorders (Addison's disease), renal disease (minimal change disease), and infections (hepatitis B and mononucleosis).
The second most common factor associated with osteonecrosis was idiopathic causes (26 patients, 11.1%), followed by trauma (22 patients, 9.4%), other causes (19 patients, 8.1%), haemoglobinopathies (17 patients, 7.2%), and alcoholism (7 patients, 3%). Some of the diseases listed under “other causes” included caisson disease, HIV, and osteomyelitis. The most common haemoglobainopathies in this population were sickle cell disease and thalassaemia.
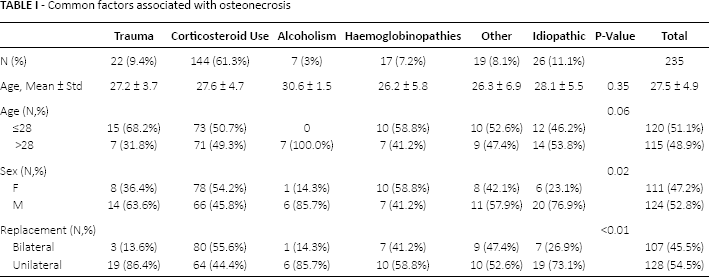
The most common causes in male patients were corticosteroid use (66 patients, 53%) and idiopathic causes (20 patients, 16%), while the most common causes in female patients were corticosteroid use (78 patients, 70%) and haemoglobinopathies (10 patients, 9%). The most common factor associated with osteonecrosis in younger patients, which was defined as patients younger than or equal to the median age of 28, were corticosteroid use (73 patients, 61%) and trauma (15 patients, 13%). In comparison, corticosteroid use (72 patients, 62%) and idiopathic causes (14 patients, 12%) were the most common categories in older patients. Lastly, the most common factors in patients requiring bilateral THA were corticosteroid use (81 patients, 75%) and other causes (9 patients, 8%), and the most common factors in patients requiring unilateral THA were corticosteroid use (64 patients, 50%) followed by trauma (19 patients, 15%) and idiopathic causes (19 patients, 15%). This data as well as patient demographic and surgical information is listed in Table I.
Common factors associated with osteonecrosis
Sub-group analysis
There was no significant difference in mean age at time of surgery between the osteonecrosis risk groups (p-value = 0.35). Similarly, there were no significant differences in younger and older patients between the different osteonecrosis factors (p-value = 0.06).
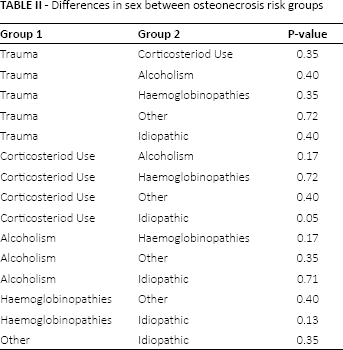
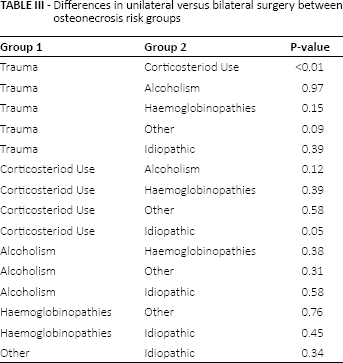
Using the omnibus test, significant differences in sex were noted between the osteonecrosis risk groups (p-value = 0.02), as well as in patients undergoing a unilateral or bilateral THA (p-value<0.01). Pair-wise testing showed that there were significant differences in sex between the corticosteroid use group and the idiopathic group (p-value = 0.05), and similarly, there were significant differences in unilateral and bilateral THA between the corticosteroid use and trauma groups (p-value<0.01) and the corticosteroid use and idiopathic groups (p-value = 0.05). The results of the sub-group analysis are shown in Table I and the results of the pair-wise tests are shown in Table II and Table III.
Differences in sex between osteonecrosis risk groups
Differences in unilateral versus bilateral surgery between osteonecrosis risk groups
Discussion
Osteonecrosis of the femoral head is a debilitating pathologic entity that is often diagnosed at an advanced stage and treated with THA (1, 3). Even though osteonecrosis commonly occurs in younger patients, there are no studies in the literature describing the most common factors associated with osteonecrosis in young patients requiring THA.
In this study, the most common factor associated with osteonecrosis in patients aged 35 or younger treated with THA is corticosteroid use, followed by idiopathic causes and trauma. Several studies have previously elucidated the relationship between corticosteroids and osteonecrosis. For example, D'Aubgine et al (10) found that corticosteroid therapy was noted in 36% of osteonecrosis cases in adults, while Mont et al (2) concluded that corticosteroid use and alcoholism account for over 90% of all cases of osteonecrosis. While our results show that corticosteroid use is an important factor in the development of osteonecrosis in young patients, alcoholism does not appear to be a commonly associated factor in this population. The association between corticosteroid use and osteonecrosis is most likely due to the common use of high-dose corticosteroids in the medical management of various diseases that affect young patients (11). However, the diminished role of alcoholism in the development of osteonecrosis may be due to changes in patterns of alcohol consumption and demographic differences in our study population compared to other studies (12). Interestingly, Castro and Harris (13) found that the average age of patients with alcohol-related osteonecrosis is 49, which is outside of the age range included in this study. In fact, all 7 cases of alcohol-related osteonecrosis in our study occurred in patients over the median age of 28, which supports the finding that this condition occurs more commonly in older patients.
Furthermore, we found no significant difference in osteonecrosis factors stratified by patient age, however, significant differences were noted between males and females, as well as patients undergoing a unilateral or bilateral THA. More specifically, there were significantly more female patients in the corticosteroid group compared to the idiopathic group. This finding is most likely due to the fact that SLE was the most common reason for corticosteroid use in our study and SLE is significantly more common in females (14). Similarly, patients with osteonecrosis secondary to corticosteroid use were more likely to have bilateral THA compared to patients with osteonecrosis secondary to trauma or idiopathic causes. Since trauma is usually unilateral, the higher proportion of bilateral osteonecrosis in patients with systemic exposure to corticosteroids seems plausible. Furthermore, Goker and Block (15) as well as Castro and Harris (13) found that patients with osteonecrosis associated with corticosteroid use were more likely to have bilateral disease compared to patients with osteonecrosis related to idiopathic causes, which is consistent with our findings.
This study has several strengths. To begin with, our analysis includes a large sample size generated from an extensive and comprehensive chart review. Secondly, this dataset includes a comparable number of male and female patients as well as unilateral and bilateral cases from an urban referral centre, which allows us to compare across groups and improves the generalisability of our results. Thirdly, since this study was performed at a major academic medical centre, we were able to include a broad range of factors associated with osteonecrosis, and subsequently determine the most common factors associated with osteonecrosis in young patients undergoing THA. Lastly, given the prevalence of osteonecrosis in younger patients and the need for THA in disease management, this study focuses on a topic that is clinically relevant and has not been previously studied.
Nevertheless, this study has some limitations. For example, given the retrospective nature of this study and the proposed multi-factorial model of osteonecrosis, it is possible that patients were misclassified. However, as there is no reliable way to determine the aetiology of osteonecrosis except history, an attempt was made to classify all patients as accurately as possible by conducting a detailed chart review. Furthermore, other authors have used a similar approach to describe associations between risk factors and osteonecrosis (13, 15). Secondly, since this study spans approximately 30 years, it is possible that common causes of osteonecrosis in today's clinical practice, such as HIV and anti-retroviral therapy (16, 17), are underestimated in these results. Interestingly, a sub-analysis of our findings showed that from 2000-2010, the proportion of patients in the corticosteroid group decreased to 59%, while the proportion of patients in the “other causes” group increased to 11%. This trend may reflect that other causes of osteonecrosis such as HIV are becoming more relevant in this population; however, corticosteroid use continues to remain an important factor in the development of osteonecrosis in younger patients.
Overall, these findings have wide-ranging clinical implications. First and foremost, this study clearly describes the most common factors associated with osteonecrosis in young patients treated with primary THA. These findings allow clinicians to better understand the aetiology of osteonecrosis in young patients, and it improves their ability to counsel and educate patients regarding their disease process. In addition, these findings raise several important future research questions. For example, it will be interesting to compare the findings from this younger patient population to similar studies focusing on older patients. It will also be interesting to compare patient outcomes after THA between different osteonecrosis risk groups. This strategy has been previously proposed by Castro and Harris (13), who suggested that patient outcomes may be related to osteonecrosis aetiology due to the relationship between patient demographics and risk factors.
In conclusion, osteonecrosis commonly occurs in young patients and often requires THA for disease management. We found that the most common factor associated with osteonecrosis in patients aged 35 or younger treated with THA is corticosteroid use, followed by idiopathic causes and trauma. Furthermore, factors such as alcoholism that are commonly associated with osteonecrosis in the general population do not play a major role in younger patients. We also found no significant difference in age across all osteonecrosis risk groups, however, there are significant differences in sex and unilateral versus bilateral THA between groups. Overall, our findings show that several factors are implicated in the development of osteonecrosis in young patients, and these factors should be given consideration in determining disease etiology, educating patients, and studying outcomes.
Footnotes
Financial support: None.
Conflict of interest: None.