
Abstract
Background
There is a lack of uniformity in the diagnostic criteria for femoroacetabular impingement (FAI), and few studies discuss the prevalence of radiographic changes in asymptomatic individuals. These factors make it difficult to establish a natural history of this disease. The aim of this study was to assess the prevalence of radiographic signs of CAM and Pincer FAI in an asymptomatic population.
Methods
A cross-sectional study was performed from July 2013 to December 2013. A total of 185 subjects were analysed. Inclusion criteria: no history of hip pain or orthopedic disease; and being 20-60 years old. Exclusion criteria: athletically active; or patients who would not allow acquisition of appropriate radiographs for analysis. Radiographs were obtained in anteroposterior and Dünn 45° view to access: alpha angle (AA), triangular index (TI), crossover sign (CS), lateral-centre edge (LCE) angle and acetabular index (AI).
Results
Median age was 34 years (27-49.5) and FAI was present in 53% of all subjects. 32.44% (60) was the overall CAM-type prevalence and 42.7% (79) the overall Pincer-type prevalence. Only 2 subjects presented the 3 overcoverage signs (AI, LCE and CS). An association was noted between the presence of AI <0° and the LCE >40° (p = 0.05).
Conclusions
Our study established a higher prevalence of radiographic markers of FAI in an asymptomatic population.
Introduction
Hip osteoarthritis (OA) is a multifactorial disease (1) and can be considered as the combination of systemic and local risk factors. However, not all risk factors have been clearly identified by medical studies (2).
The attempt to explain the origin of hip OA based on mechanical principles is an established approach. Previously, the degeneration provided by the slipped capital femoral epiphysis (3), the developmental dysplasia of the hip (4), and the Legg-Calvé-Perthes disease have been described. However, not all cases of early osteoarthritis are explained by these reported alterations. More recently, Ganz et al (5) and Leunig et al (6) sought to provide correlations between subtle morphological changes in the proximal femur and/or acetabulum and the development of hip OA. These subtle morphological changes were described as femoroacetabular impingement (FAI), and perhaps were considered the main cause of non-dysplastic hip OA (5, 7). Banerjee and McLean (8) have previously reported a succinct and detailed story of FAI.
Most of the researchers consider radiographs as the main method for assessing FAI (9, 10). Although the theory of FAI was proposed a decade ago, there is a lack of diagnostic criteria uniformity for both CAM and Pincer types. In addition, there are few studies on the prevalence of radiographic changes in asymptomatic individuals. These factors make it difficult to establish a natural history and its correlation with hip OA. The purpose of this study was to assess the prevalence of radiographic signs for CAM and Pincer FAI in an asymptomatic population.
Methods
A cross-sectional study was performed from July-2013 to December-2013 in the Hospital de Clínicas de Porto Alegre (HCPA) after approval by our Institutional Review Board (120132). The study followed the ethical guidelines of the 1975 Declaration of Helsinki. Subjects participated voluntarily after signing the consent form. Patients were enrolled based on inclusion and exclusion criteria in a medical screening appointment (criteria in the study flow diagram - Fig. 1). The study size was calculated based on the Kang et al (11) article in which they analysed 100 asymptomatic hips determining the prevalence of 39% of FAI. Estimating an error of 5% and a confidence level of 95% the minimum sample size was 59 subjects.
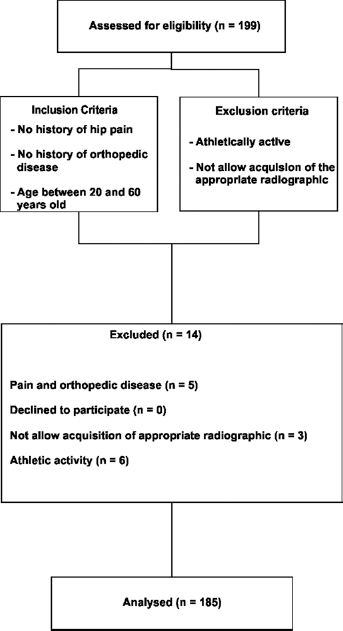
Study flow diagram.
Radiographs were obtained in the anteroposterior (AP) and Dünn 45° views. AP radiographs were taken in an orthostatic position with legs rotated 15° internally with a tube to film distance of 120 cm. The central beam was directed to the midpoint between the upper border of the symphysis and a horizontal line connecting both anterior iliac spines. The Dünn 45° view was taken as described previously (10). The AP pelvic radiographs were considered adequate if there was no lateral rotation of the pelvis. For this purpose, the Obturator Foramen Index was used (12).
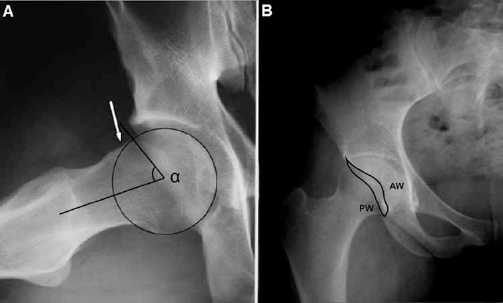
One blinded author analysed all plain radiographs to assess the prevalence of radiographic signs of CAM and Pincer FAI. The radiographs were analysed for: the alpha angle (AA) (13); the triangular index (TI) (14); the crossover sign (CS) (15); the lateral centre-edge angle (LCE) (15, 16); and the acetabular index (AI) (15). Figures 2 and 3 show and describe the measurement methods performed by the blinded author. This method is easily repeatable and reproducible since it uses anatomical parameters easily identified on a radiograph and the measurement is carried out by using a goniometer. Good reproducibility of the measurement methods is shown by the value obtained in the Kappa coefficient to verify the agreement between the observers. An AA ≥55° in the Dünn 45° view or an abnormal TI was considered radiograph evidence of CAM-type. An overcovered acetabulum, corresponding to a radiograph marker of Pincer-type FAI, was considered when: the crossover sign was present or the LCE >40° or AI <0°. Cutoff points were chosen based on the analysis of the main articles that analyze these radiographic signs of FAI (14-15-16-17).

Anteroposterior (AP) view. On the right hip the lateral centre-edge angle measurement (LCE), in this case with a value of 28°, being considered a normal hip. The LCE angle is measured by placing a perfect circle around the circumference of the femoral head. Starting from the centre of the circle is drawn a straight vertical line with upward direction. Also in the same central region of the circle another straight line arrives on the lateral edge of the acetabulum. Then, LCE is the value of the angle between these two lines. On the left hip the measurement of the acetabular index (AI), in this case with a value of 8°, being considered a normal hip. The AI is measured by drawing a straight line from the upper medial acetabular sclerotic zone (“sourcil”) laterally. From this same point is drawn another straight line, parallel to the straight line that defines the horizontal plane of the pelvis (teardrop to teardrop). The angle between the 2 straight lines that emerge from the “sourcil” is the AI.
Statistical analysis
Statistical analysis was performed using SPSS version 18.0 (SPSS Inc., IBM Corporation, Armonk, New York). Kolmogorov-Smirnov test was applied and all quantitative variables had non-normal distribution. Quantitative variables are given as the median and inter-quartile range, and qualitative variables are reported as frequencies. Mann-Whitney test was used to identify age differences between genders, as well as grades differences in AA, AI and LCE between genders and between the two hip sides. Fisher's exact test was used to verify possible correlations between the overcoverage signs. To obtain the Kappa coefficient 60 radiographs were selected randomly. These images were evaluated by 2 other blinded authors at temporally distinct moments with an interobserver reliability of 0.93. Differences were considered significant when the two-tailed p-value <0.05.
Results
Data from 199 subjects was initially screened and according to inclusion and exclusion criteria, 185 asymptomatic subjects were analyzed (Fig. 1) (18). The demographic population characteristics are shown in Table I. The distribution of the study population was homogeneous between the genders. The age median (interquartile range) at the time of medical appointment was 44 years (28-52) for women and 29 years (26.5-41.5) for men (p<0.001).
Demographic characteristics
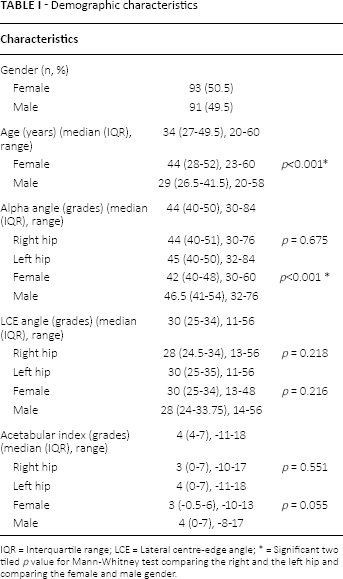
IQR = Interquartile range; LCE = Lateral centre-edge angle;
Radiograph findings of CAM-type were present in 18.92% (35) of asymptomatic subjects when considering the AA, and in 8.64% (16) when considering the TI. Bilaterally CAM type was observed in 8.1% (15) of the subjects when considering the AA and in 4.86% (9) when considering the TI. The radiograph markers of Pincer-type were diagnosed in 18.5% (34) of the asymptomatic subjects taking into account the CS, in 12.4% (23) taking into account the LCE >40° and in 27.6% (51) when considering the AI <0°. Differences in measured grades of AA, LCE and AI were shown in Table I. Important information concerning normal subjects and dysplastic subjects are shown in Table II.
Subjects femoroacetabular impingement signs prevalence
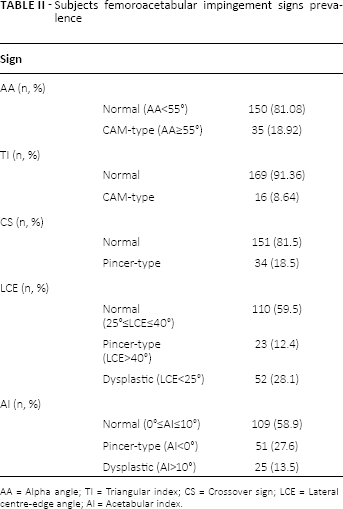
AA = Alpha angle; TI = Triangular index; CS = Crossover sign; LCE = Lateral centre-edge angle; AI = Acetabular index.
The correlations between radiograph markers of FAI are shown in Table III. A significant number of subjects (59.46% (110)) did not present with the crossover sign and did not present an AI <0°, but this correlation was not statistically significant (p>0.05). Only 1 correlation was significant. This was the correlation between the presence of a LCE >40° and the presence of an IA <0° (p<0.05).
Pincer femoroacetabular impingement signs distribution
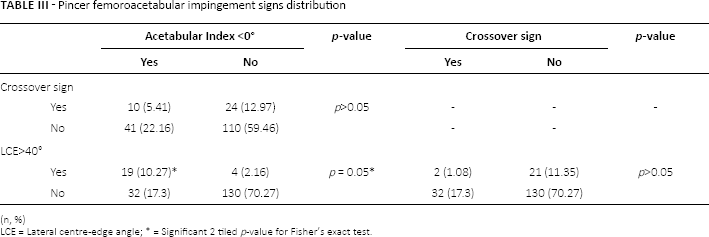
(n, %)
LCE = Lateral centre-edge angle; * = Significant 2 tiled p-value for Fisher's exact test.
The overall prevalence of CAM-type in our study was considered as the alteration of at least one of the two measurements (AA and TI); as well as the overall prevalence of Pincer-type that was considered as the presence of at least one of the three measurements (CS, LCE and AI). We found an overall prevalence of CAM of 32.44% (60) and an overall prevalence of Pincer of 42.7% (79).
Discussion
Our study found that a considerable proportion of asymptomatic subjects present radiograph signs of FAI. The overall prevalence of CAM-type markers in these individuals was 32.44%, and the overall prevalence of Pincer-type signs was 42.7%.
During the early 21st century, it was postulated that CAM and Pincer FAIs were precursors of hip OA (5, 7, 19, 20). The prevalence of hip OA varies, and is present in approximately 3-6% of the population (21), and Jorring (22) report that hip OA is present in 4.7% of individuals older than 40 years of age. Anticipating a potentially strong correlation between FAI and OA, we expected that the prevalence of both diseases would be similar, or that the prevalence of OA would be similar to the prevalence of some radiographic signs of FAI. In contrast, our study showed a higher prevalence of FAI (overall prevalence of 53%) and a slightly higher prevalence of each of the radiological signs of FAI compared to the reported low prevalence of hip OA. This overall prevalence of FAI are higher to those described by Kang et al (11) (39%) in a sample of asymptomatic patients undergoing computed tomography. Despite the high value observed, we believe that there is no influence of ethnic factors in our study. One of the few recently published articles (23) addressing the ethnic fact also reported no difference in the FAI prevalence in patients of different ethnicities.
One of the difficulties we had was to define the CAM type of FAI. Notzli et al (13) described the AA as a marker of the loss of femoral head sphericity and, therefore, as a marker of the CAM type. The authors arbitrarily chose a cutoff between the normal and the abnormal angle, with values above 50° being considered abnormal (13). The lack of uniformity in the criteria for defining CAM is an important issue. Similar to Notzli et al, we were had to define a cutoff for the AA. We consider an angle greater or equal to 55° as an abnormal AA. Using this same cutoff, Domayer et al (17) demonstrated a sensitivity of 96.4% in the Dünn 45° radiograph view compared to nuclear magnetic resonance (NMR). Domayer et al (17) considered angles below this value to have a high risk for giving a false-negative in the Dünn 45° view. By using 55° as the cutoff in a study of NMR images of asymptomatic patients, Hack et al (24) found a 14% prevalence of CAM. In comparison, we found a CAM prevalence of 18.9% in asymptomatic patients.
In a prevalence study, Gosvig et al (25) used the TI (14) to define the prevalence of CAM, and reported that CAM was present in 17% of men and 4% of women. While, the strength of this study was the large number of subjects (n = 4151), the weakness was that they used only one radiograph view (AP) to assess CAM-type. We disagree with the TI as a proposed measurement to screening CAM (25, 26). These authors reported that a good agreement between the AP and the lateral radiographs exist, and that only 3% of morphological changes in men and 5.5% in women would not be detected in the AP view. In contrast, our study showed that we failed to to diagnose 56.7% of CAM-type when Dünn 45° view (with AA measurement) was not considered and was considered only the TI.
Using the crossover sign, Ezoe et al (27) reported that 20% of subjects with OA and 5% of asymptomatic subjects were diagnosed with Pincer FAI. We disagree with these values, since we observed that of 18.5% of asymptomatic individuals were diagnosed with a Pincer-type FAI. In addition our study used other markers to diagnose the overcovered acetabulum found with Pincer-type FAI; we found 12.4% of Pincer FAI considering the LCE angle and 27.6% considering the AI. Another difference between our study and the Ezoe et al is that we use the Obturator Foramen Index described by Tönnis (12) and they used the Siebenrock et al (19) criteria. There were no age criteria for selection and athletic subjects were not excluded from the study, which may have affected the results of Ezoe et al.
Many authors (5, 7, 19, 20) believe that FAI is the main inducing factor for hip OA. Doherty et al (28) evaluated the correlation between hip deformities and the risk to develop OA. They found a risk for developing osteoarthritis that was 12 times higher in subjects with abnormal correlations between the head and neck of the femur. However, they concluded that the non-spherical shape of the femoral head and an enlargement of the femoral neck may be a consequence of the OA, and not necessarily its cause. Bardakos and Villar (29) evaluated the outcome of patients with CAM and the initial signs of OA for a minimum period of 10 years. They concluded that a hip with CAM did not always progress to the final stage of OA. They also concluded that other factors beyond the acetabulum and proximal femur geometry can influence this progression. They believed that when present, the altered morphology of the proximal femur (evidenced by measuring the proximal femoral medial angle) and the acetabular version (shown by the posterior wall sign) can be partially responsible for a progression to osteoarthritis.
Audenaert et al (30) analysed the radiographs of 121 patients with early stages of OA related to FAI. They concluded that there was uncertainty to the cause of the progression of these individuals to the final stages of OA, even in those with high physical activity. These authors believed that the role of genetic and environmental factors might be underestimated and recommended careful surgical indication in these patients due to the high prevalence of radiographic findings of FAI. Hartofilakidis et al (31) retrospectively evaluated 96 asymptomatic individuals with radiographic evidence of FAI. These patients were followed for an average period of 18.5 years (range 10-40 years). Only 17.7% progressed to OA. The authors advised against any prophylactic surgery (“preserver”) in the absence of symptoms.
One possible problem that could influence in our results would be the lack tomography or resonance images, however these images are considered by some authors (32, 33) as being of moderate reliability.
There is a lack of sufficient data to determine whether the CAM and Pincer are diseases in which the final outcome is the degeneration of the hip joint, or if they are only one risk factor for OA or just a radiographic sign. This difficulty in establishing a relationship between OA and FAI still persists and the aim of this study was not to clarify this relationship but show a possible way for this. It became clear after this study, that a relevant number of asymptomatic individuals have radiographic signs of FAI. It was hoped that these subjects had a prevalence of such radiographic signs lower than the related prevalence of OA. However we can only conclude that the cause-effect between FAI and OA is yet to be fully established. This study is one of the largest cross-sectional to evaluate asymptomatic subjects and together with future cohort studies, are essential for defining the roles of these radiographic markers in determine if FAI leads to OA.
Footnotes
Financial support: None.
Conflict of interest: None.