
Abstract
Aseptic loosening is the most common cause of prosthesis failure after total hip arthroplasty (THA). We measured serum cross-linked carboxyterminal telopeptide of type I collagen (ICTP), tartrate-resistant acid phosphatase 5b (TRAP5b), dickkopf-1 (dkk-1) and sclerostin; and urinary α isomer of C-terminal cross-linked telopeptide of type I collagen (αCTX-I) to investigate their potential diagnostic value detecting aseptic loosening after THA. Biomarkers were measured in 24 subjects with aseptic loosening of THA versus 26 control subjects without loosening after THA. Serum ICTP in the loose group (7.04 ng/mL) was higher than controls (5.15 ng/mL), (p = 0.0007). ROC analysis demonstrated that a serum ICTP >5.5 ng/L had a sensitivity of 91% and specificity of 69% for detecting aseptic loosening (area under ROC curve = 0.77, p = 0.0001), resulting in a positive predictive value (PPV) of 73% and a negative predictive value (NPV) of 90%. Serum TRAP5b in the aseptic loosening group (4.17U/L) was higher than controls (3.44 U/L), (p = 0.03). A serum TRAP5b >2.46 U/L had sensitivity of 100% and a specificity of 31% to detect aseptic loosening (AUC 0.67, p = 0.031), resulting in a PPV of 57% and a NPV of 100%. Serum dkk-1, serum sclerostin and urinary αCTX-I were not elevated in subjects with aseptic loosening (p>0.05).
Serum ICTP and TRAP5b show potential utility as screening biomarkers for excluding aseptic loosening, because of their ability to discriminate individuals without disease. Our finding of elevated ICTP, generated by the action of matrix metalloproteinases, suggests a role for this group of endopeptidases in aseptic loosening.
Introduction
Although total hip arthroplasty (THA) remains a highly successful operation with 1.3 million procedures carried out each year worldwide (1), a current meta-analysis of worldwide joint register data shows that 12% of first (primary) THAs fail within 10 years requiring their removal and replacement, termed ‘revision’ surgery (2). Aseptic loosening accounts for approximately 70% of failures (3).
Several studies have explored the diagnostic accuracy of biochemical markers of bone turnover for detecting aseptic loosening. The serum bone resorption markers N-telopeptide cross-links of type-I collagen (NTX-I), tartrate-resistant acid phosphatase 5b (TRAP5b) and Interleukin-1 beta (IL-1β) may be raised in aseptic loosening (4-5-6), with TRAP5b having the highest diagnostic accuracy, with a sensitivity of 83.3% and specificity of 91.7% (6). The urinary bone resorption markers NTX-1, deoxypyridinoline (DPD) and pyridinoline (PYD) may also be raised (7-8-9-9), with the most promising exhibiting a sensitivity of 82% and specificity of 87% for NTX-I (10). To date, serum osteocalcin (OC) is the only bone formation marker found to be raised in subjects with aseptic loosening after THA, with a sensitivity of 69% and a specificity of 65% (10).
Cross-linked carboxyterminal telopeptide of type I collagen (ICTP) and α isomer of C-terminal cross-linked telopeptide of type I collagen (αCTX-I) are markers of bone resorption that reflect type I collagen degradation (11). Dickkopf-1 (dkk-1) is a signalling molecule released by osteocytes and acts as a potent wnt signalling inhibitor. Low levels of dkk-1 cause proliferation of osteoblasts, but long-term high levels cause a loss of viability (9). Sclerostin, produced by osteocytes, is an antagonist of both Wnt and bone morphogenetic protein (BMP) signalling. Sclerostin concentration is inversely correlated with osteoblast cell number and activity in vitro, and high levels inhibit both the proliferation of osteoblasts and their level of mineralisation in vitro (12). TRAP5b is a bone resorption marker of osteoclast number (13).
We examined whether ICTP, αCTX-I, TRAP5b, dkk-1 and sclerostin are elevated in subjects with aseptic loosening versus subjects without aseptic loosening in the late period after THA and evaluated their diagnostic value as screening tools for aseptic loosening.
Materials and methods
Study design and population
All subjects provided written informed consent, and the study was approved by a research ethics committee. The study was carried out in accordance with the ethical principles stated in the declaration of Helsinki.
The study population and exclusion criteria for this patient population have been described previously (7). Briefly, men and post-menopausal women who had previously undergone cemented THA for primary or secondary osteoarthritis were studied. The aseptic loosening group comprised subjects with radiological evidence of implant failure using the criteria of Harris et al (14). The cases were further stratified by anatomic site of loosening into that affecting the femur or pelvis. The control subjects comprised a group of patients matched for age, sex and time since primary THA, but with no current radiological evidence of loosening.
Biochemical markers of bone turnover were measured from serum separated blood and second-morning void urine samples collected between 0800 and 1100 h after a complete overnight fast. Serum ICTP was measured by quantitative enzyme-immunoassay (UniQ ICTP EIA, Orion Diagnositica, Espoo, Finland). Urinary αCTX-I was measured by enzyme-linked immunosorbent assay (AlphaCrosslaps, Nordic Bioscience Diagnostics, Herlev, Denmark), and expressed as a ratio to urinary creatinine using Johnson & Johnson Vitros-250 analyser (Ortho-Clinical Diagnostics, High Wycombe, UK). TRAP5b was measured from fresh serum samples (samples that had not undergone a freeze-thaw cycle) using a Microvue TRAP5b EIA kit (Quidel Corporation, San Diego, California, USA). Serum sclerostin was measured using a TECOmedical Group Human Sclerostin EIA kit (Quidel Corporation, San Diego, California, USA). Serum dkk-1 was measured using enzyme immunoassay (Biomedica, Vienna, Austria). All measurements were performed twice and expressed as the mean of the 2 readings, with a coefficient of variation of less than 10% between results.
Statistical analysis
Between group comparisons of continuous data were made using Student's t-test or the Mann-Whitney test; categorical data were analysed using the Chi-Squared test (Tab. I). Biochemical marker data were not normally distributed, and were compared using the Mann-Whitney test (Tab. II). All analyses were conducted 2-tailed and made using Prism 6 for Windows (Graphpad software inc., San Diego, California, USA) using a critical p-value of 0.05. Where the marker was identified as being significantly different in cases versus controls, the diagnostic accuracy of the marker was quantitated by receiver operator characteristic (ROC) analysis using MedCalc software (MedCalc, Ostend, Belgium).
Demographics of study subjects
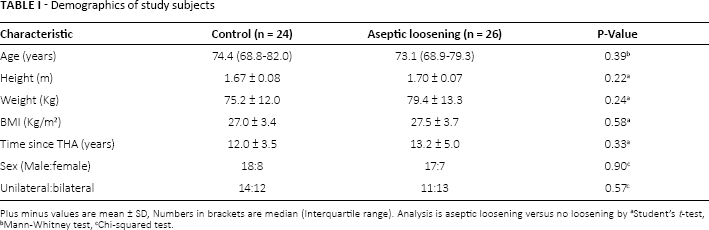
Plus minus values are mean ± SD, Numbers in brackets are median (Interquartile range). Analysis is aseptic loosening versus no loosening by
Student's t-test
Mann-Whitney test
Chi-squared test.
Diagnostic utility of bone turnover markers with significant difference between controls and aseptic loosening
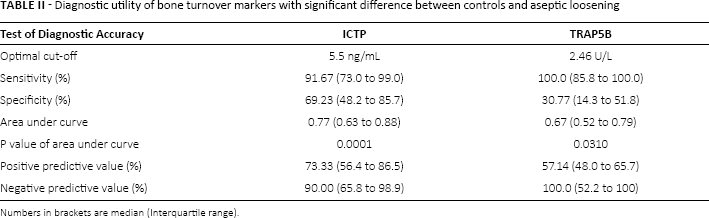
Numbers in brackets are median (Interquartile range).
Results
Population characteristics
In total 50 subjects were studied, 24 with aseptic loosening and 26 subjects with no radiological evidence of loosening. The demographic characteristics of the subjects in each group were similar (Tab. I). Within the aseptic loosening group 13 subjects had loosening around both the femoral and acetabular component, 6 had acetabular pelvic loosening only, and 5 had femoral loosening only.
Biomarkers in cases versus controls
The median serum ICTP concentration was 7.04 ng/ml (IQR: 6.02 to 8.71) higher in the aseptic loosening cases versus controls (p = 0.0007, Fig. 1A). The median TRAP5b concentration was 4.17 U/L (3.11 to 5.80) higher in the aseptic loosening cases versus controls (p = 0.04, Fig. 1B). The serum concentration of dkk-1and sclerostin were similar in cases versus controls (p>0.05), as was urinary αCTX-I (p>0.05).
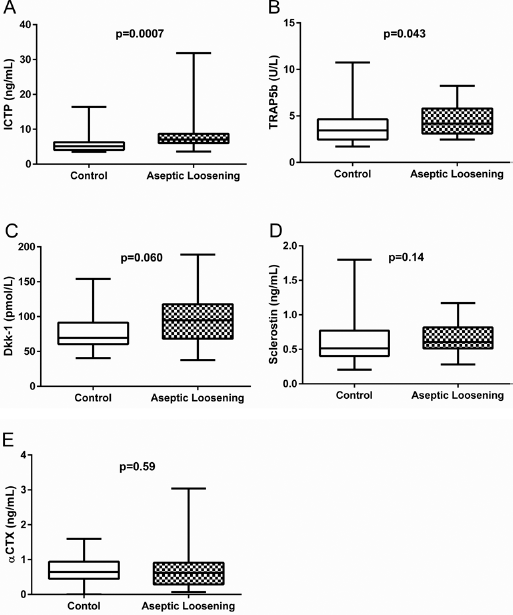
Bone turnover markers in study subjects. Box plots show median (Interquartile range). Comparison is cases versus controls by Mann-Whitney test.
Diagnostic accuracy
A ICTP value of >5.5 ng/mL had a sensitivity of 91% and specificity of 69% for detecting aseptic loosening, with a positive predictive value (PPV) of 73% and a negative predictive value (NPV) of 90% (Tab. II). A TRAP5b value of >2.5 U/L had a sensitivity of 100.0% and specificity of 30.8% for detecting aseptic loosening, with a PPV of 57% and a NPV of 100%.
Site-specific aseptic loosening analysis
The serum concentration of ICTP was higher in both those subjects with femoral aseptic loosening (p = 0.0002) and in those with acetabular loosening (p = 0.01) versus controls (Fig. 2A). A ICTP value of >5.5 ng/mL had a sensitivity of 100% and a specificity of 62.5% for detecting femoral aseptic loosening, with a PPV of 60% and a NPV of 100% (Tab. III). The same ICTP value gave a sensitivity of 89.5% and a specificity of 58.1% for detecting acetabular aseptic loosening, with a PPV of 57% and a NPV of 90% (Tab. III).
Diagnostic utility of bone turnover markers with significant difference between controls and those with evidence of site specific aseptic loosening
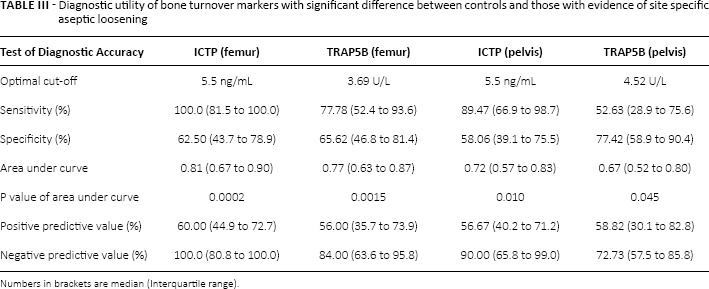
Numbers in brackets are median (Interquartile range).
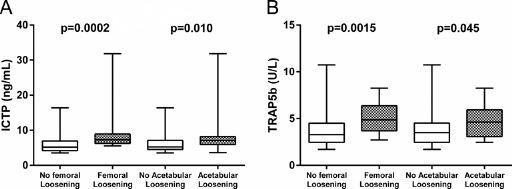
Bone turnover markers in study subjects. Box plots show median (Interquartile range). Comparison is site specific cases versus controls by Mann-Whitney test.
The serum concentration of TRAP5b was higher in both those with femoral aseptic loosening (p = 0.002) and in those with acetabular loosening (p = 0.045) versus controls (p = 0.045, Fig. 2B). TRAP5b of >3.7 U/L had a sensitivity of 77.8% and a specificity of 65.6% for detecting femoral aseptic loosening, with a PPV of 56% and a NPV of 84% (Tab. III). A TRAP5b of >4.5 U/L had a sensitivity of 52.6% and a specificity of 77.4% for detecting acetabular loosening, with a PPV of 59% and an NPV of 73% (Tab. III).
Discussion
We examined the diagnostic accuracy of several bone turnover markers for detecting aseptic loosening in a case control study. We found that serum ICTP, a pyridinoline crosslink of 2 αCTX-I chains generated by the action of MMPs on type-I collagen (11), was a sensitive biomarker for detecting aseptic loosening. Serum TRAP5b, an osteoclast-derived resorptive enzyme, was also sensitive for detecting aseptic loosening. Urinary αCTX-I, serum sclerostin, and serum dkk-1 were not discriminatory markers of aseptic loosening.
Li et al (2004) have previously shown that ICTP is elevated in the setting of aseptic loosening at the knee (15), which is also the most common cause of knee prosthesis failure. Our finding that elevated ICTP has potential utility as a marker of aseptic loosening at the hip supports its further investigation as a screening tool for prosthesis failure. The observation that ICTP is a sensitive biomarker of aseptic loosening also suggests that MMP-mediated collagen degradation plays a relatively greater role in this setting than found in non-inflammatory bone loss such as osteoporosis (16).
Elevation of ICTP occurs in bone loss due to myeloma (17), as well as other cancers causing bony metastases, including lung (18), breast (19) and prostate (20). Elevation of ICTP also occurs in rheumatoid disease (21), as it does with increased bone turnover secondary to coeliac disease (22). However, ICTP may also be elevated in non-bone related conditions, for example in liver disease, due to the metabolism of collagen within the organ (23), and in atherosclerotic disease (24), which may contribute to its lack of specificity for aseptic loosening.
Garnero et al have previously suggested that relative differences in the presence of type I collagen fragments ICTP versus CTX is indicative of distinct enzymatic pathways of collagen degradation, as ICTP is eradicated by the action of cathepsin K that is the principle protease involved in bone resorption by osteoclasts (13, 25). Our finding that αCTX was not elevated is supported by others findings (6, 9), and the notion that MMP-mediated collagen degradation may be a relatively more important mechanism of bone loss in this instance (26). Although osteoclasts secrete MMPs that contribute to collagen degradation, our data are consistent with the view that other cells also present in the loosening membrane, such as macrophages and fibroblasts (27), may contribute significantly to matrix degradation.
Hip and knee replacement in those over 60 years of age has a UK prevalence of 6% (28), and x-ray will remain the gold standard for diagnosing aseptic loosening. The development of a reliable systemic biomarker would enable asymptomatic screening to be conducted in primary care, and potentially reduce the population exposed to ionising radiation in this patient group. A primary care appointment costing £25 (29) and measurement of bone markers at £20-25 (30) would also indicate a cost saving compared to the tariff of £70 for an outpatient orthopaedic clinic appointment (31). Further research is required to confirm the role and cost of these biomarkers as a screening tool for aseptic loosening.
Footnotes
Financial support: None.
Conflict of interest: None.